
Abstract
Objectives. To study whether the prevalence of overweight and obesity in children and adolescents is restricted by habitat (urban vs rural). Methods. A total of 753 healthy children and adolescents, out of which 293 (159 boys and 134 girls) were collected Santiniketan (rural area) and 460 (241 boys and 219 girls) were from Calcutta and the suburbs (urban area), aged 8 to 18 years took part in the study. Participants were subsequently divided into 3 age groups: group I, 8 to 12 years; group II, 13 to 15 years, and group III, 16 to 18 years. Results. It was observed that the overall prevalence of overweight and obesity in the study was 9.6% and 5.7%, respectively. Urban residence and high level of parental education are associated with overweight and obesity in children and adolescents (R2 = 40.3%). Conclusion. Prevalence of overweight and obesity among children and adolescents is not restricted to any particular habitat and warrants early intervention if this global epidemic is to be checked.
Introduction
Obesity has become a growing concern because of its high prevalence and association with morbidity.1-3 The prevalence of obesity is increasing worldwide at an alarming rate in both developed and developing countries.4-6 The increasing number of obese children and adolescents all over the world demands an investment in the primary and secondary prevention of overweight and obesity in this age group.7,8 Most individuals develop their eating and activity patterns during childhood and the adolescent years. The changes in nutrition and lifestyles brought about by the popularity of fast foods, soft drinks, sedentary lifestyle, lack of exercise, and increased television watching and computer use may be the causes of overweight seen in children of both rural and urban areas.9,10
The probability that children with high BMI will be overweight and obese during adulthood increases markedly throughout childhood.11-13 In children, the BMI changes substantially with age, and it has been shown that at birth, the median BMI is around 13 kg/m2, and at the age of 1 year it is 17 kg/m2; this decreases to 15.5 kg/m2 at age 6, and then increases to 21 kg/m2 at age 20. Hence, the cutoff point needs to be related to age to define childhood obesity. Many studies have used reference centiles and in most studies, percentiles of BMI for age and sex have been used as cutoff points to identify overweight and obesity in children. 14 BMI between the 85th and 95th percentiles is widely accepted as the definition of overweight, and BMI greater than the 95th percentile as the definition of obesity.15,16
In a study in Costa Rica, the prevalence of overweight and obesity was higher in urban regions compared with rural regions. 17 In a another study in the United States, using US standards, it was reported that the BMI percentile was nearly equal across rural and urban children, but the rural children were more often at risk of overweight, and urban children were more overweight. 18 Excessive weight was found to be more prevalent in urban children than rural ones. 19 Another study on Australian children and adolescents, the prevalence of overweight and obesity was observed to be up to 4% higher in urban than in rural participants. 20 In an Indian study (Punjab state), 21 the prevalence of overweight and obesity in urban children were 11.63% and 2.35%, respectively, which was significantly higher compared with rural children and adolescents (4.7% and 3.63%, respectively). In fact, in India, the studies comparing the prevalence of overweight and obesity between urban and rural children and adolescents are very few.22,23 Though the children and adolescents of urban areas are more prone to becoming obese because they maintain a sedentary lifestyle, their rural counterparts are no less vulnerable to overweight and obesity owing to changing lifestyles, including change in food habits.
Keeping this view in mind, the present cross-sectional study aimed to study the prevalence of overweight and obesity among children and adolescents by habitat (rural vs urban) and also to find out how well BMI could be explained by sociodemographic covariates.
Participants and Methods
Study Population
The present study was a cross-sectional one and comprised 753 healthy children and adolescents, aged 8 to 18 years, selected from the rural as well as urban areas of West Bengal, India. The number of participants from rural and urban areas were 293 (159 boys and 134 girls) and 460 (241 boys and 219 girls), respectively. The participants were divided into 3 age groups: group I = 8 to 12 years; group II = 13 to 15 years, and group III = 16 to 18 years. The participants in rural areas were selected randomly from 3 schools at the Bolpur subdivision, Birbhum district, West Bengal, India. Urban participants were selected randomly from 10 schools in Calcutta and its suburbs in West Bengal, India. To obtain a better picture, different categories of schools such as private, government-sponsored, and government schools were considered using a stratified randomization procedure: that is, schools in each category were selected randomly from a list of private, government-sponsored, and government schools in the study areas. The school enrolment rates (approximately) in the study areas were 98% (urban) and 90% (rural). This sample size was sufficient to represent the general population at a 5% level of significance with a power of 80% (β = .80). The study was undertaken between March and September, 2008. The age of all participants was ascertained from the date of birth. Written consent was obtained from the school authorities before the actual commencement of the work. The institutional ethics committee approved the study.
Socioeconomic and Demographic Characteristics
An open-ended schedule was used to obtain information on socioeconomic and demographic characteristics. The responses to the open-ended schedule were free and spontaneous, and respondents were not limited in their replies to a particular question posed to them. The name, age (date of birth), sex, marital status of parents, and maturation status as well as information on socioeconomic characteristics, including family type, approximate monthly family income and expenditure, occupation and education of parents, and so on were obtained using the same schedule.
Anthropometric and Body Composition Measures
Height, weight, waist circumference, and skinfold thickness at the biceps, triceps, subscapular, and suprailiac were obtained using standard techniques. 24 Height (to 0.1 cm) and weight (to nearest 0.1 kg) of lightly clothed participants were measured using an anthropometer and a weighing scale, respectively. Skinfold thickness at the biceps, triceps, subscapular, and suprailiac were measured on the left side of the body to the nearest 0.2 mm using a Holtain skinfold caliper (Holtain Corporation, UK). The sum of the 4 skinfolds (SF4) was calculated subsequently. Minimum waist circumference (MWC) and hip circumference was measured with an inelastic tape to the nearest 0.1 cm. MWC was measured at the narrowest part of the torso (in between the lowest rib and iliac crest). Waist to hip ratio (WHR) was computed accordingly. Percentage of body fat (%BF) and BMI were measured using an Omron HBF 356 body fat analyzer (Omron Corporation, Tokyo, Japan).
Statistical Analyses
Descriptive statistics such as mean and standard deviation (SD) were determined separately for both rural and urban participants and for both sexes. Comparison of groups for anthropometric and body composition measures was done using a sex-specific t test. For the 3 age groups, the internally derived (calculation of percentiles out of collected data) age-specific percentiles of BMI were used to assess the prevalence of overweight (≥85th to <95th percentile) and obesity (≥95th percentile) in the study population. A χ 2 test was undertaken to assess the differences in the prevalence of overweight and obesity by habitat. Finally, multivariate regression analysis of BMI by sociodemographic covariates—namely, habitat, sex, parental education and occupation, approximate monthly family income, and expenditure—was also undertaken to determine the relative contribution of these covariates to explain BMI during childhood and adolescence. However, only those covariates with a significant contribution to BMI were considered.
All statistical analyses were performed using the SPSS (PC+ version 10; SPSS Inc, Chicago, IL). A P value of <.05 (2-tailed) was considered as significant.
Results
The mean age of participants in urban and rural areas was 13.4 ± 2.0 and 12.7 ± 2.5 years, respectively. The average monthly family income (approximate) among the urban and rural participants was 17,041 and 13,107 rupees, respectively (1 US$ = 48 rupees in Indian currency). It was also observed that about 52% and 38% of parent(s) had education up to class 12 and graduation, respectively.
The mean and SD of anthropometric and body composition characteristics by habitat are presented in Table 1. Sex-specific (rural boys vs urban boys and rural girls vs urban girls) t tests revealed that there were significant (P < .001) rural–urban differences for weight, BMI, MWC, SF4, and WHR. It is imperative to mention that urban participants had higher mean values for weight, BMI, MWC, SF4, and WHR than rural participants.
Anthropometric and Body Composition Characteristics in the Study Population (n = 753)
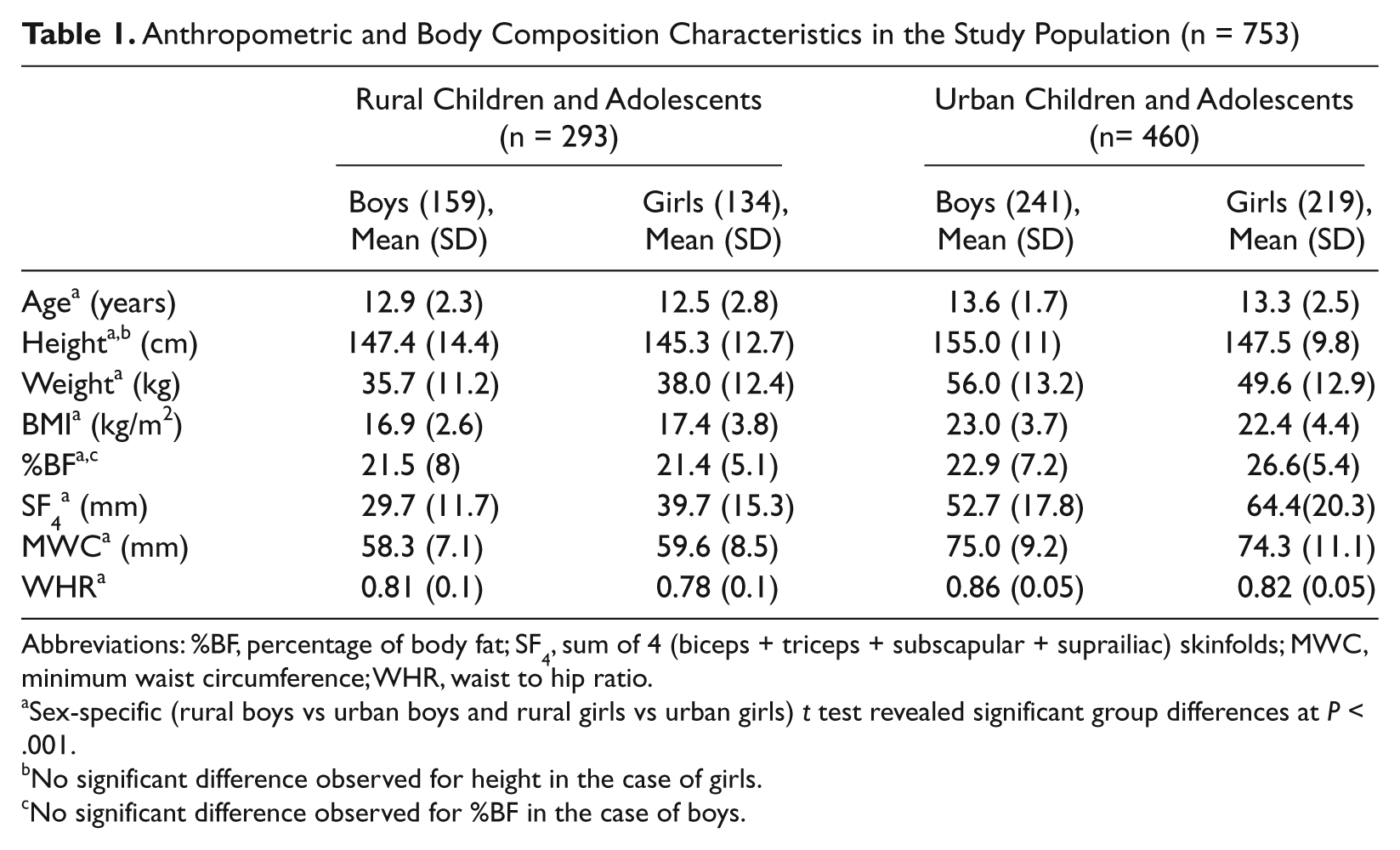
Abbreviations: %BF, percentage of body fat; SF4, sum of 4 (biceps + triceps + subscapular + suprailiac) skinfolds; MWC, minimum waist circumference; WHR, waist to hip ratio.
Sex-specific (rural boys vs urban boys and rural girls vs urban girls) t test revealed significant group differences at P < .001.
No significant difference observed for height in the case of girls.
No significant difference observed for %BF in the case of boys.
The prevalence of overweight and obesity as a function of the 3 age groups and habitat is presented in Table 2. It was observed that the prevalence of overweight (BMI for age between ≥85th percentile to <95th percentile) and obesity (BMI for age ≥95th percentile) in the study was 9.7% and 5.6% (not shown in the table), respectively. However, the prevalence of overweight and obesity for the 3 different age groups were 9.4%, 9.7%, and 10%, and 6.1%, 5.3%, and 5.4%, respectively. The prevalence of overweight in rural and urban children and adolescents were 10.2%, 9.4%, and 10.3%, and 8.7%, 9.9%, and 9.7%, respectively, for the respective age groups. On the other hand, the prevalence of obesity was 5.9%, 5.1%, and 5.2%, and 6.3%, 5.3%, and 5.6% for the rural and urban children and adolescents in the 3 age groups, respectively. However, no significant differences were observed in the prevalence of overweight and obesity between the rural and urban areas.
Prevalence of Overweight and Obesity by Age Groups and Habitat (Rural vs Urban) a
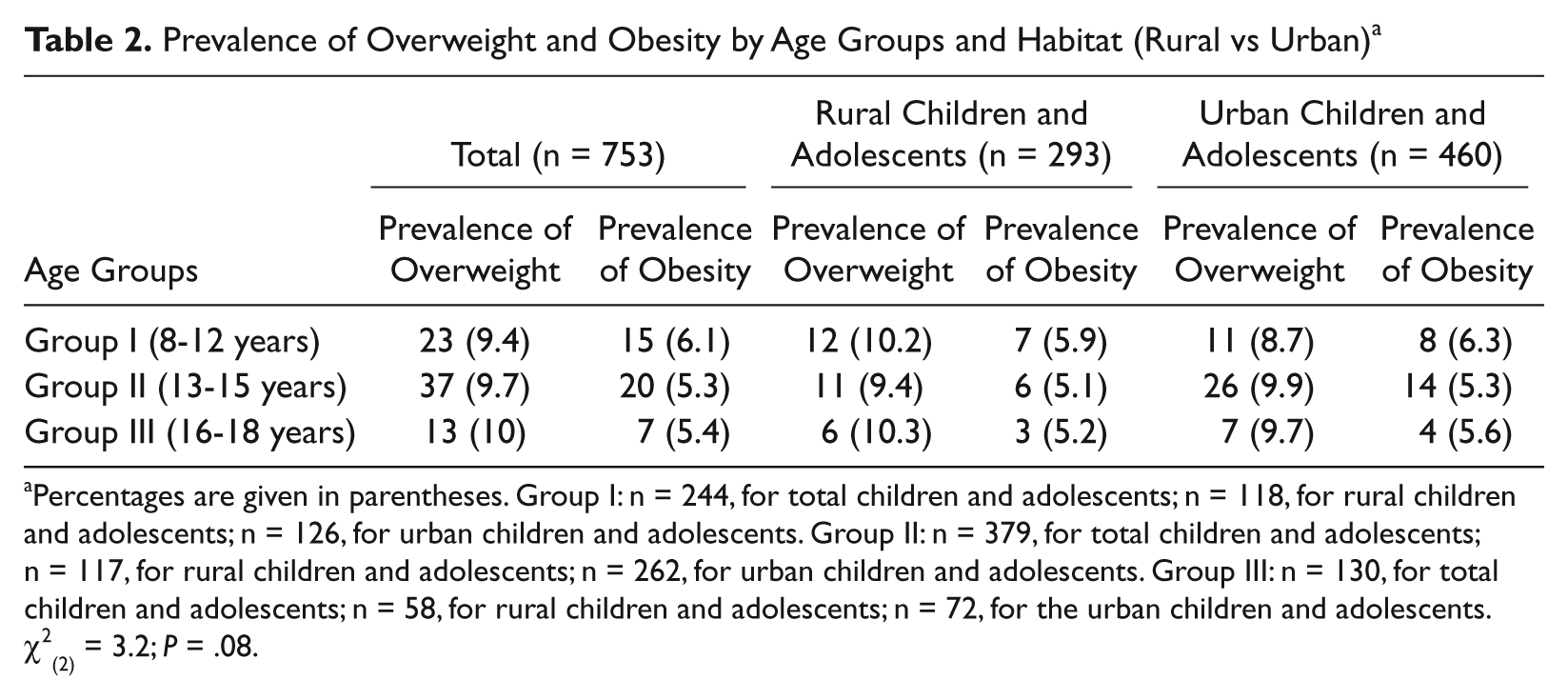
Percentages are given in parentheses. Group I: n = 244, for total children and adolescents; n = 118, for rural children and adolescents; n = 126, for urban children and adolescents. Group II: n = 379, for total children and adolescents; n = 117, for rural children and adolescents; n = 262, for urban children and adolescents. Group III: n = 130, for total children and adolescents; n = 58, for rural children and adolescents; n = 72, for the urban children and adolescents.
Multiple regression analyses of BMI (adjusted for age and sex) by sociodemographic covariates were also undertaken and are presented as β coefficients or parameter estimates (B), standard error of B (SE B), value (T), and full model (R2) in Table 3. It was observed that about 40% (R2 = 0.403) of the total variance in BMI was explained by habitat and parental education in the study population.
Multivariate Regression Analyses of BMI (Adjusted for Age and Sex) by Sociodemographic Covariates a
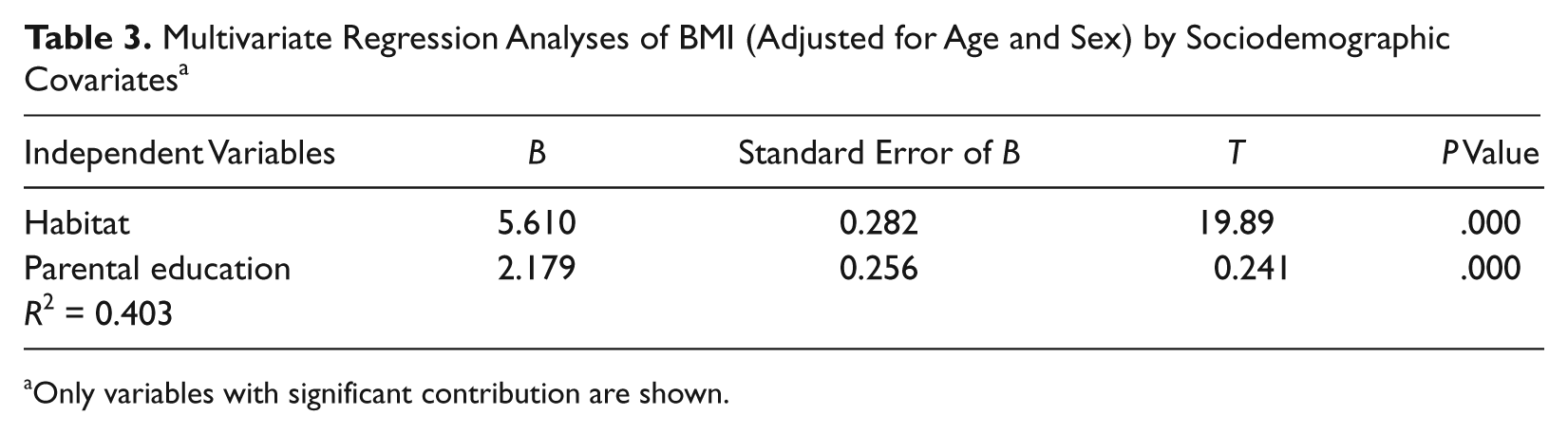
Only variables with significant contribution are shown.
Discussion
The present school-based cross-sectional study aimed to examine the prevalence of childhood overweight and obesity by habitat (rural vs urban) and also to find out how well childhood BMI could be explained by sociodemographic covariates. The results suggested that the prevalence of overweight and obesity was not restricted to any particular habitat; however, participants (irrespective of sex) in urban areas were more prone to become overweight and obese in the study.
It has become increasingly important to identify the risk factors predisposing to overweight or obesity. Examination of the factors involved in weight gain and obesity during childhood in developing countries, where socioeconomic changes are going on, is crucial for predicting the future impact because the problem of obesity is emerging at a time when undernutrition remains a significant public health problem in the developing world. 5
In India, studies regarding the prevalence of overweight and obesity among rural and urban children and adolescents are virtually absent, and most of the studies undertaken pertain to children and adolescents in metropolitan cities. People in the Indian subcontinent have faced undernutrition for many generations, and Indian babies are among the smallest in the world. 25 However, the obesity epidemic is of recent origin, and it is more common among urban than rural Indians despite the higher birth weights of urban babies. This suggests that postnatal factors must also contribute to rising obesity during childhood.25,26 In the present study, significant rural–urban differences were observed in different anthropometric and body composition variables among children and adolescents. Urban boys showed significantly increased stature, body weight, BMI, SF4, MWC, and WHR compared with rural boys. Similarly, the girls in urban areas had significantly higher means for weight, BMI, %BF, SF4, MWC, and WHR compared with their rural counterparts. The reason is that urban children and adolescents are more exposed to urbanized patterns of behavior and as a consequence of an increasingly sedentary lifestyle, and the level of physical activity among children and adolescents in urban areas has been declining steadily compared with that of their rural counterparts. Concomitant with that, children and adolescents belonging to urban areas become more habituated and predisposed to sedentary lifestyles and consumption of fast foods owing to influence of the media and television. Although the etiology is complex, a number of findings suggest that television watching time and the use of computer games has significantly reduced energy expenditure and is positively related to weight gain.27,28 Moreover, parents with higher educational levels are more likely to be involved in outdoor activities (activities outside the home, including their own profession) and in turn become less attentive toward their children. Therefore, children whose parents were engaged in work away from home consumed processed or fast foods more often than children whose parents were less educated or for whom only 1 parent was engaged in work outside the home. In fact, in this part of the world, both parents working outside the home is less common in rural areas compared with urban areas or metro cities. This implies that family attitude is important in the causation and predisposition of children to childhood overweight and obesity. 29
The prevalence of overweight and obesity among children and adolescents across age groups was almost overlapping. In the present study, although there was some difference in the prevalence of overweight and obesity among the children and adolescents of urban and rural sectors in the 3 age groups, the difference was not statistically significant. Therefore, it seems reasonable to argue that the prevalence of childhood overweight and obesity is not restricted to urban or metropolitan areas only; rather, rural children and adolescents are also exposed to this, possibly owing to behaviors characterized by lack of physical activity and excess consumption of fast foods. In a study conducted in central India, a higher prevalence (9.7%) was also found among children in English-medium schools as compared with those in other schools (3.7%). 29 Studies from rural areas mainly emphasized undernutrition, and data on overweight or obesity are virtually absent; however, in rural area of Wardha district, Gujarat, India, the prevalence of overweight/obesity was 2.2%, using the same definition as in the present study. 30
It was also observed in the present study that sociodemographic variables such as habitat and parental education had contributed significantly to explain 40% of the total variation (R2 = 0.403) of BMI even after adjustment for age and sex. In fact, in a number of studies, authors were of the opinion that place of residence of the participants was an important factor because the participants from urban areas were more prone and habituated to an urbanized form of behavior.27,28,31
However, some shortcomings are associated with the present study, including the relatively small sample size. Owing to ethnic and cultural heterogeneity in the Asian Indian population, it is necessary to study other ethnic groups to see if the observed trend also exists among them. Investigation should also be initiated in the Indian diaspora worldwide to elucidate if they (migrant Asian Indian children and adolescents) also show trends similar to that of residents in India or the native population of the respective countries. Such studies would generate valuable information about the childhood prevention of adult chronic diseases, which are becoming a concern because of the morbidity and mortality caused in children and adolescents. Moreover, prospective studies are required to better understand the underlying physiological mechanisms in childhood obesity.
Footnotes
Acknowledgements
AG received financial support (Via Grant No F. 5-163/2006 [HRP]) from the University Grants Commission (UGC), Government of India, New Delhi. The author is grateful to Rupak Dutta, Sanjib Kumar Bala, and Minakshi Bhagat for the collection of data materials. The author is also grateful to the school authorities as well as the participants for their sincere cooperation during data collection.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research, and authorship of this article: AG received financial support (Via Grant No F. 5-163/2006 [HRP]) from the University Grants Commission (UGC), Government of India, New Delhi.