
Abstract
Introduction. Worldwide interest in problem-based learning (PBL) has grown in past decades. This article aims to evaluate the perceived effectiveness, appropriateness, benefits, and challenges attributed to the use of PBL in public health education in Vietnam with a view to providing recommendations for curricular design and future policy. Methods. Teachers at 2 universities in Hanoi participated in group interviews, and students from these 2 universities completed Likert-style questionnaires. Results. Students and teachers regarded PBL positively. However, there was consensus that hybrid models that used PBL alongside other methods are probably the most beneficial for public health education in Vietnam. Teachers discussed the educational and systematic advantages and difficulties associated with PBL. Conclusion. Themes arising from this analysis may be helpful in guiding future research—namely, regarding the application of PBL in low- and middle-income countries and in public health. Further exploration of the use of PBL hybrid models is discussed.
Introduction
Problem-based learning (PBL) is a teaching method that traces its roots to 1968 at McMaster University in Canada, where it was originally pioneered for the purpose of improving medical education. 1 PBL emphasizes student-centered learning in small groups where the instructor facilitates discussion through probing questions and provision of appropriate resources. Since then, PBL has been implemented at universities around the globe 2 and has spread to other areas of study, including engineering, 3 nursing, 4 educational administration, 5 and public health. 6 This dissemination has been driven in part by an increased demand for students who are adequately prepared to enter the globalized workplace3,7,8 and perhaps equally so by the desire of universities to avoid lagging behind current educational trends.
Despite PBL’s burgeoning popularity, there are many who have questioned its effectiveness in producing more competent practitioners.9,10 There are a number of concerns that must be taken into account when PBL is implemented in any context—most notably, the increased time constraints imposed on students and teachers, which exacerbate preexisting deficits in staff numbers and training.7,11-14 Other features to consider prior to implementing PBL include the following: committed staff15-16; external support from the ministry of health or the ministry of higher education 11 ; existing or developing program infrastructure, that is, facilities in which to meet, administrative design, well-stocked libraries, and Internet access3,13-15; a dynamic group of leaders who are able to cast a cohesive vision for change3,13; cultural appropriateness7,8,17; and access to sufficient financial resources.13,14 In low- and middle-income countries, gaining access to extensive libraries or the necessary human and financial resources may be an even greater challenge.14,18
In North America, Western Europe, and Australia, where the use of PBL in medical curricula has proliferated, the body of literature seeking to understand and evaluate PBL is extensive.12,19,20 However, there is little research into PBL’s application in low- and middle-income countries, in Asia, and in particular in public health. Further exploration of the use of hybrid models—those combining PBL with other methods—is also merited.
Since the introduction of open-door policies and market mechanisms in 1986, Vietnam’s economy has grown rapidly, and national trends in tertiary education are changing with a similar sense of urgency.11,21 With a society that is experiencing a deficit in health care workers and a system of preventive health that is receiving greater attention than in decades past, there has been a recent push for a new direction for public health curricula. 11 One of the primary designs being considered in Vietnam is PBL, reportedly for its focus on integrated, student-centered learning and students’ dedication to independent and collaborative examination of ideas.1,22
The aim of this article is to provide an initial exploration of the application of PBL in public health settings in low- and middle-income countries. Although it is not comprehensive in its size or scope, it may serve as a platform for future research. Specifically, this study sought to evaluate the perceived effectiveness, appropriateness, benefits, and challenges attributed to the use of PBL in public health education in Hanoi, Vietnam—as understood through the eyes of teachers and students—with a view to providing recommendations for curricular design and policy.
Methods
Participants
There are 2 public universities in Hanoi that educate public health professionals: Hanoi School of Public Health (HSPH) and Hanoi Medical University (HMU). The whole of HSPH is given to teaching public health, whereas at HMU public health education accounts for only 1 faculty. At HSPH, there are 87 professors and 1500 students. At HMU, there are 16 professors and 416 students in the Faculty of Public Health.
A snowball sampling technique 23 —one where study participants recruit future participants from among their acquaintances—was used in the selection of both teachers and students from each Vietnamese public health program. Several contacts in Hanoi were initially established through preexisting connections to Australian public health programs. Teachers were then selected for participation in group interviews via their connection with these initial contacts; in like manner, these teachers then selected several classes from which students were then selected. An announcement was made in these classes, and all students who volunteered were selected. No incentives were provided to any participant in this study. The snowball sampling technique is one that acknowledges and takes advantage of the unique and interactional nature of social networks. 23 This method facilitated the sampling of a distinctive group of educators and students intimately engaged with the unfolding of an emergent educational trend.
All data were collected in Hanoi during November 2010.
Procedure
Question prompts to guide the teacher group interviews (Table 1) as well as the student questionnaires (Table 2) were developed through collaboration with the director of the Medical Committee Netherlands-Vietnam and a medical doctor at HMU with a master’s degree in health professions education. The literature has shown that the definition of PBL as a concept or methodology varies greatly across cultures, universities, and even individuals.7,24 Thus, questions were developed to better comprehend each participant’s understanding of PBL, the application of PBL in the classroom, and participants’ assessment of its utility and appropriateness in Vietnam.
Teacher Group Interview Questions—Teacher Perceptions of PBL in Public Health Education in Vietnam.
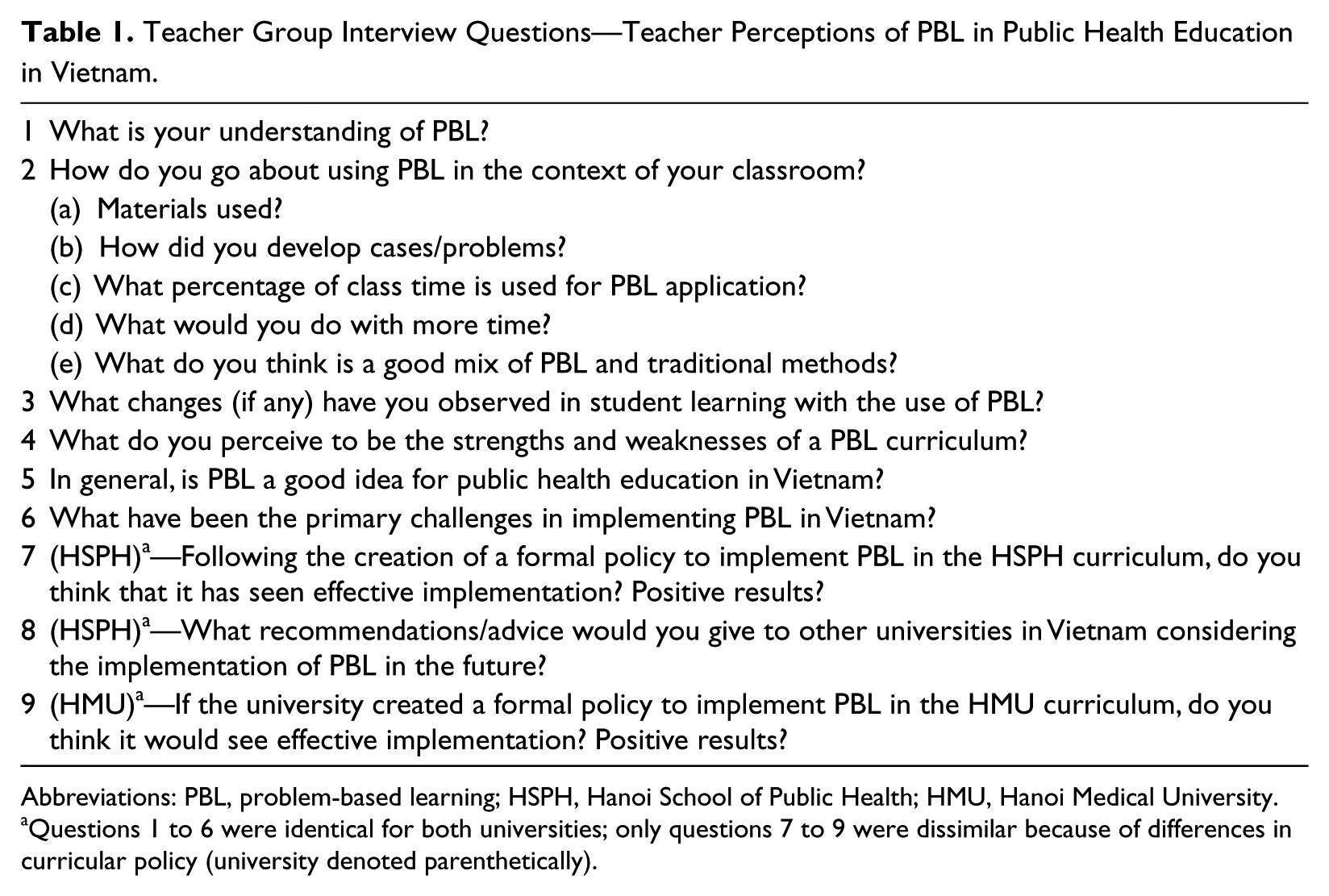
Abbreviations: PBL, problem-based learning; HSPH, Hanoi School of Public Health; HMU, Hanoi Medical University.
Questions 1 to 6 were identical for both universities; only questions 7 to 9 were dissimilar because of differences in curricular policy (university denoted parenthetically).
Student Questionnaire: Student Perceptions of PBL in Public Health Education in Vietnam n (%).
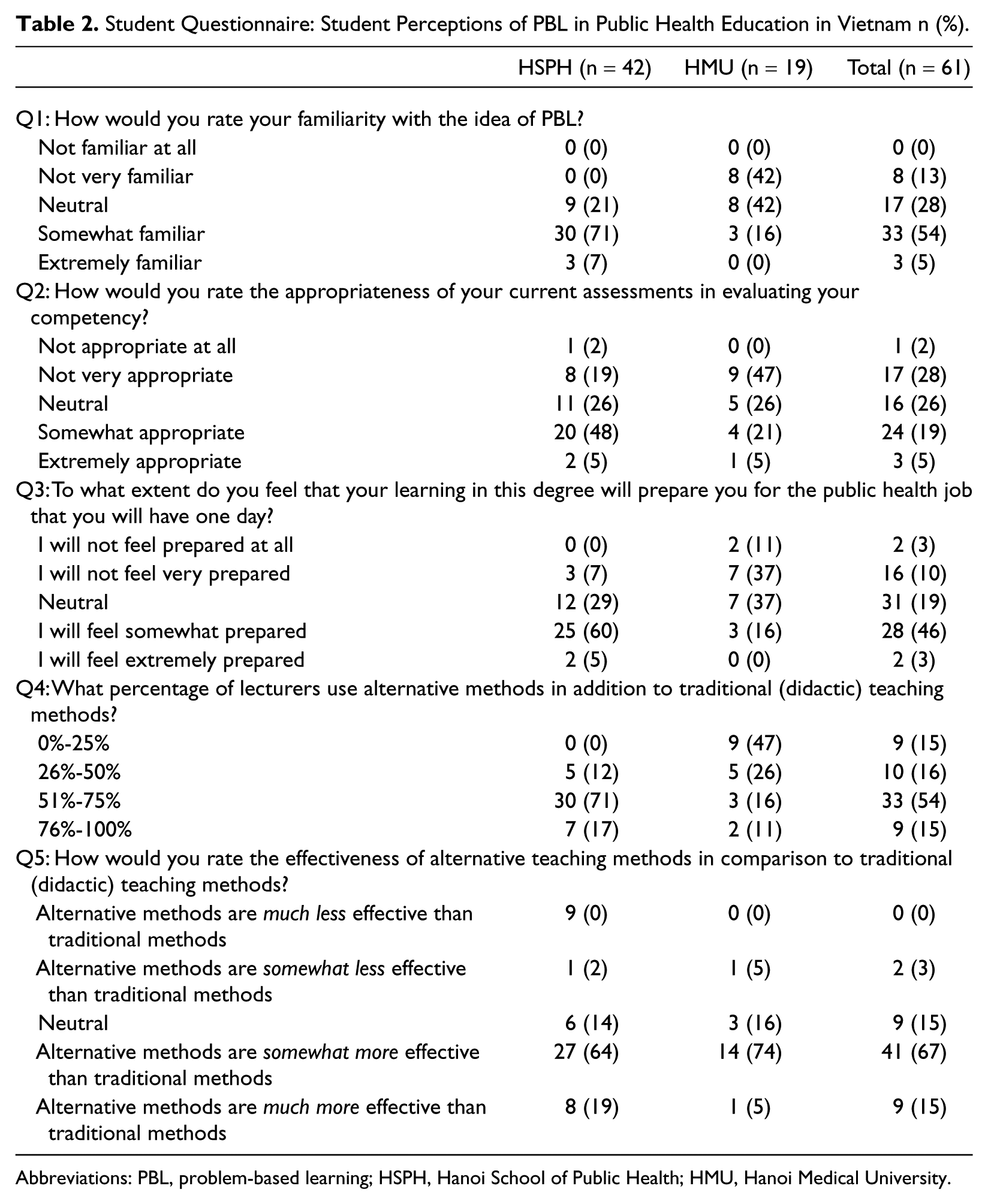
Abbreviations: PBL, problem-based learning; HSPH, Hanoi School of Public Health; HMU, Hanoi Medical University.
Group interviews were conducted in a semistructured manner, with a written interview guide distributed to each teacher at the beginning of the meeting. Data were collected until saturation was reached—that is, until responses became redundant and all participants had exhaustively explicated their perspective; each group interview lasted about 1 hour. Group interviews were carried out in English. All answers were summarized in detail and recorded by the researcher as ideas developed during the meeting.
Student questionnaires were originally written in English; they were then translated, typed, and printed in Vietnamese.
Analysis
An inductive content analysis of the teacher group interviews was carried out using a Policy Delphi technique 25 to identify points of consensus and divergence of opinion regarding the issues at hand. The Policy Delphi technique is a variant of Helmer and Dalkey’s classical Delphi technique and is typically used with the purpose of creating a forum for the exchange of ideas—one in which the researcher is interested in having an informed target group present opinions and evidence rather than necessarily reaching a group consensus. 25
Student responses were all numerical and based on a Likert scale, and thus, analysis was possible without any backtranslation. Student questionnaires were analyzed using Microsoft Excel to assess for trends within the quantitative data, by university.
Results
At HSPH, 1 group interview with 3 teachers—aged 30, 32, and 36 years—was conducted (3.4% of total teaching staff). Likewise, 1 group interview with 3 teachers—aged 37, 52, and 53 years—was carried out at HMU (18.8% of total teaching staff).
At HSPH, 42 students completed questionnaires (2.8% of the total number of HSPH students). At HMU, 19 students completed the same questionnaire (4.6% of total number of students in the faculty of public health).
HSPH has recently initiated the implementation of a schoolwide policy requiring the application of PBL techniques by every teacher in every classroom; on the other hand, teachers at HMU are not required to use PBL techniques, but a number of teachers have nonetheless chosen to use such techniques of their own accord.
The lecturers at both HSPH and HMU demonstrated a similar working knowledge of PBL concepts, and both programs recognized Dutch universities as having provided the necessary guidance for starting up (Maastricht and Erasmus Universities, respectively). Both spoke extensively of the Maastricht 7-jump method—a series of steps designed to simplify and streamline the process of PBL. 22 Representatives from HSPH and HMU—some of whom were present in the group interviews—directly observed PBL being carried out in a setting outside of Vietnam, attended a series of workshops, and then returned to Hanoi to prepare their own adapted version of such a curriculum. Lecturers at both universities said this opportunity to observe PBL was invaluable.
Lecturers at both institutions stated that their experience supports the notion that PBL is most appropriate in Vietnam when hybridized with traditional methods (ie, didactic) and other alternative teaching methods. At HSPH, where there is a formal PBL policy in place, lecturers estimated that 80% of coursework time is spent using PBL methods; at HMU, where there is no formal policy, lecturers (those who are implementing PBL of their own accord) said that only 20% of their coursework time goes to PBL methods.
Staff attributed many strengths and weaknesses to PBL methods. Strengths included the following: saving time in preparation for lectures, development of closer relationships with students, and observing students as being more active, participatory, enthusiastic, and engaged. They also, however, cited a number of potential difficulties: spending far more time in the preparation of the curriculum and materials, inadequate numbers of lecturers and tutors, increased demands on already busy students, lack of curricular integration and collaboration between departments, and inability to access certain materials necessary for PBL.
When asked if PBL is a good idea for public health education in Vietnam, lecturers at HMU (with no PBL policy) all responded affirmatively. The lecturers at HSPH (with a PBL policy) also voiced affirmation of PBL but not without some uncertainty.
Lecturers at HMU (with no PBL policy) stated clearly that they thought that a university policy requiring the use of PBL methods could be beneficial because of its ability to mobilize monetary and educational resources for an otherwise underresourced initiative. They also added that a PBL policy could facilitate access to improved facilities and provide for a cohesive interdepartmental vision for public health education, both of which, they said, were currently lacking.
Lecturers at HSPH (with a PBL policy) acknowledged the potential ability of their university policy to bring about the sort of change HMU staff hoped for but voiced a measure of hesitancy, noting that PBL is now required in all courses, regardless of their shared belief that some courses are not well suited to it. They also noted that such a policy requires certain teachers to participate in the PBL method who are resistant, distrustful, or incapable. Finally, they said that PBL was an excellent method for learning but that the breadth of external materials necessary for successful implementation are simply not presently available in the Vietnamese language, and thus, much time is consumed in the translation of materials for students. PBL, as is repeatedly acknowledged throughout the literature, requires that the student have access to a broad scope of external resources that allow him or her to independently research and problem solve.3,5,6,14,15
The student questionnaires yielded a clear trend—a differentiation in scores between the 2 surveyed programs (Table 2). It was evident that students at HSPH (with policy), when compared with students at HMU (with no policy), were more familiar with the concept of PBL (with 79% and 16%, respectively, recording either “somewhat familiar” or “extremely familiar”); claimed that a greater percentage of their lecturers used alternative teaching methods (with 88% and 27%, respectively, recording that more than half of their lecturers use some form of alternative teaching methodology); thought that their assessments were more appropriate (with 53% and 26%, respectively, recording either “somewhat appropriate” or “extremely appropriate”); and felt better prepared to take a public health job (with 65% and 16% respectively recording “somewhat prepared” or “extremely prepared”). Students at both schools overwhelmingly answered that alternative methods of teaching are more effective than traditional methods (with 83% at HSPH and 79% at HMU reporting that they would rate alternative teaching methods as “somewhat more effective” or “much more effective” than traditional teaching methods). It should be noted that in the last 2 questions, the term alternative methods was used because both the HMU and HSPH programs draw on a combination of PBL and other methods.
Discussion
Key Findings
Teachers were, for the most part, positive as they discussed their experiences involving PBL, although a number of reservations were mentioned as well—namely, time constraints on students and teachers, lack of supportive infrastructure, inadequate human and monetary resources, and lack of access to libraries/materials in Vietnamese. Participating teachers said that PBL would be most appropriate in a hybrid form (either in conjunction with traditional methods or other alternative methods like scenario-based learning) 26 when applied in public health curricula in Vietnam. Other research corroborates the strength of the PBL hybrid model.14,27,28
The other major point of discussion that rose to prominence in teacher group interviews was a debate surrounding the advantages and disadvantages associated with implementing a university-wide policy requiring PBL. Teachers pointed out that a university-wide policy has the capacity to mobilize additional human and monetary resources and to create an administrative structure more able to support the cohesive move toward full-scale curriculum change. However, they also noted that creating a blanket policy that applies to most teachers and courses may, if not rigorously preceded by necessary preparatory measures, cause more harm and disunity than good. Over the course of the past decade, the system of medical education in Hanoi has undergone a shift toward a more active style of learning, which has motivated teachers to work collaboratively to develop more and better materials.
Students at both universities were enthusiastic about the concept of PBL, were positive when referring to their exposure to it, and perceived that alternative teaching methods were more effective than traditional didactic methods. Students who had been exposed to PBL methods more consistently perceived that they were better prepared for a public health job than those who had not been widely exposed to PBL.
Strengths and Limitations
This study included participants from the only 2 public universities educating public health professionals in Hanoi. Additionally, triangulating data collection with a quantitative component helped supplement and corroborate the qualitative data gathered through the more subjective group interviews.
Teacher group interviews were conducted in participants’ second language (English), but each spoke well enough to be clearly understood and to communicate their own thoughts; however, error in communication remained a possibility. Other factors may also have altered group interview results: thoughts not verbalized, implied points of view, desire to provide expected answers to the researcher, and bias introduced by the researcher’s word choice.
In both the qualitative and quantitative components of this study, the sample size was small, and the snowball sampling technique was subject to bias, thus leaving the potential for data that are not representative of the whole population of students and teachers. It is also possible that a sampling bias was introduced as result of the fact that those who participated were those who were most interested in the study’s content. They may have been inclined to like PBL or have been more knowledgeable about PBL than some of their fellow teachers. The selection of students may also have been affected in this way.
Implications and Recommendations
Based on opinions gathered from the literature and students and teachers in Hanoi, the PBL method is perceived as beneficial for public health education in Vietnam. Study participants spoke of the value of PBL, effectiveness aside, in that it likely helps break systematic inertia, allows for university- or region-wide academic cohesion, and mobilizes human and monetary resources.
It is known that implementing “pure” PBL is a venture that requires an extensive investment of time and monetary resources 12 and is relatively difficult to put into action anywhere in the world. And, as has been recommended by a number of other universities in contexts similar to those in Vietnam, perhaps it is a hybrid model that is best suited—one that capitalizes on several of the easily accessible benefits of active learning (eg, student engagement and facilitating work in small groups) and neglects those that are not culturally appropriate or economically feasible.7,14,28
If a university implements PBL or a PBL hybrid program, it may be beneficial to reward teachers and facilitators involved in curriculum change—considerations for promotion, monetary reward, and opportunities for professional development.13,15 Additionally, it is crucial to engage in rigorous staff development and student preparation prior to and in the midst of the change—that is, to secure excellent leadership teams capable of casting vision, answering questions, directing the flow of resources, training teachers, facilitating implementation, overseeing a responsive system of monitoring and evaluation, and organizing workshops so that students can become better acquainted and prepared for the changing expectations that will be placed on them.14,15,22 It would be prudent to consistently involve all stakeholders—the government ministries of health and education, communities, teachers, students, and professionals—in the process of curriculum change.29,30 Finally, it would be sensible to work toward a unified shift in curricular policy within a university or, better yet, across a region or nation. Such a collaborative shift will allow all participants to pool their resources and reduce the burden placed on the individual teacher or university.11,29
Conclusion
The public health students and teachers in Vietnam involved in this study perceived PBL positively, despite its challenges. In Asia, this perception exists for a number of reasons, some of which are far removed from considerations of effectiveness or appropriateness—namely, that a PBL-style curriculum seems to pave the way for a better-prepared entry into a quickly evolving global marketplace 7 ; that PBL seems to challenge current educational cultures and defy systematic inertia 7 ; that PBL helps students and teachers think in new ways 8 ; and that PBL’s consistent popularity among students, teachers, and the governments or foundations who are supplying resources for education makes it an attractive consideration for those who are dedicated to the forward progress of education in their institution, region, or nation. Resources for education, financial and otherwise, are consistently scarce, but finding ways to access them is crucial in order to continue to improve public health education in many low- and middle-income countries. Even though the results of this study have demonstrated similarities between the implementation of PBL in the public health setting and the existing literature of PBL’s use in clinical medicine, there still exists a great deficit in the literature surrounding PBL’s application in diverse contexts. This article provides an initial exploration into this area of study, but further research should continue to explore the effectiveness, appropriateness, and alternative utility of PBL and PBL hybrids in public health education.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Hoc Mai Foundation.