
Abstract
The use of medicines and nurses’/midwives’ adherence to standard treatment guidelines (STGs) were examined in Timor-Leste during the early stage of the nation’s new health system development. A cross-sectional study was conducted as the quantitative element of mixed methods research. Retrospective samples from patient registration books and prospective observations were obtained in 20 randomly selected rural community health centers. The medicines use indicators, in particular the level of injection use, in Timor-Leste did not suggest overprescription. Prescribers with clinical nurse training prescribed significantly fewer antibiotics than those without such training (P < .01). The adjusted odds ratio of prescribing adherence for clinical nurse training, after accounting for confounders and prescriber clustering, was 6.6 (P < .01). STGs for nonphysician health professionals at the primary health care level have potential value in basic health care delivery, including appropriate use of medicines, in resource-limited communities when strategically developed and introduced.
Keywords
Introduction
Improving physical access to medicines alone will not make the medicines beneficial. It is estimated that more than half of all medicines are inappropriately prescribed, dispensed, or sold and about half of the patients fail to take them correctly. 1 The findings of previous studies suggest irrational patterns of medicine use, by both patients and providers. When used inappropriately, medicines lose their therapeutic efficacy; rather, they harm health by inducing adverse side effects, iatrogenic diseases, and antimicrobial resistance. In addition to the individual and public health outcomes, the inappropriate use of medicines is a threat to both household and national health budgets.2-4 Improving the use of medicines, particularly in resource-limited settings, is a critical factor for closing the access gap to essential medicines. 5
Standard treatment guidelines (STGs) can improve health professionals’ use of medicines. However, merely distributing materials or any other type of single intervention is reported to have little or no impact.2,6 Introduction of STGs with active training methods to health professionals has been shown to be effective.7,8 Multifaceted interventions have been recommended to disseminate and implement STGs, although the evidence base is still imperfect.6,9,10 The effects in one setting may not occur in another health care setting and none of the approaches is superior in all situations. 11 In under-resourced countries, where strategies used in affluent nations are unlikely to be successful, locally adapted STGs are required.12,13
During the beginning stage of the nation’s health system rehabilitation and development in the Democratic Republic of Timor-Leste (hereafter Timor-Leste) after the 1999 crisis, medical doctors and laboratory tests were not available in primary health care (PHC) facilities in the public sector, which were called level 2 community health centers (CHCs). Apart from few exceptions, one level 2 CHC was allocated to every subdistrict that is not the district capital, where an upper-level CHC with beds or a referral hospital exists. In level 2 CHCs, nurses and midwives (hereafter nurses/midwives) were responsible for managing patients, including making clinical decisions and prescribing medicine, which is dispensed in each CHC free of charge. The majority of these personnel graduated from basic nursing schools (vocational high schools established under Indonesian administration) with or without an additional 1-year midwifery course. Based on the Basic Package of Services policy in the nation’s initial Health Policy Framework, the major needs for public health and curative treatment are planned to be delivered at such PHC facilities. 14 Nationally standardized practices, including the use of essential medicines, were developed to help these health workers so that PHC facilities could deliver basic health care for important illnesses, such as acute respiratory tract infections (ARTIs), high fever assumed as malaria, and diarrhea. Standardized treatments were disseminated through various kinds of training for nurses/midwives in CHCs, such as the clinical training program and the Integrated Management for Child Illness (IMCI) program (see Box 1). Materials developed and introduced in these programs can be considered Timor-Leste versions of STGs. Development of practice standards and implementation of various training programs were linked to the Basic Package of Services policy and other policies on health system structure and organization, resource allocation, capacity building of health professionals, and medicines supply, which are interrelated. 14
Clinical Nurse Training and IMCI Training. a
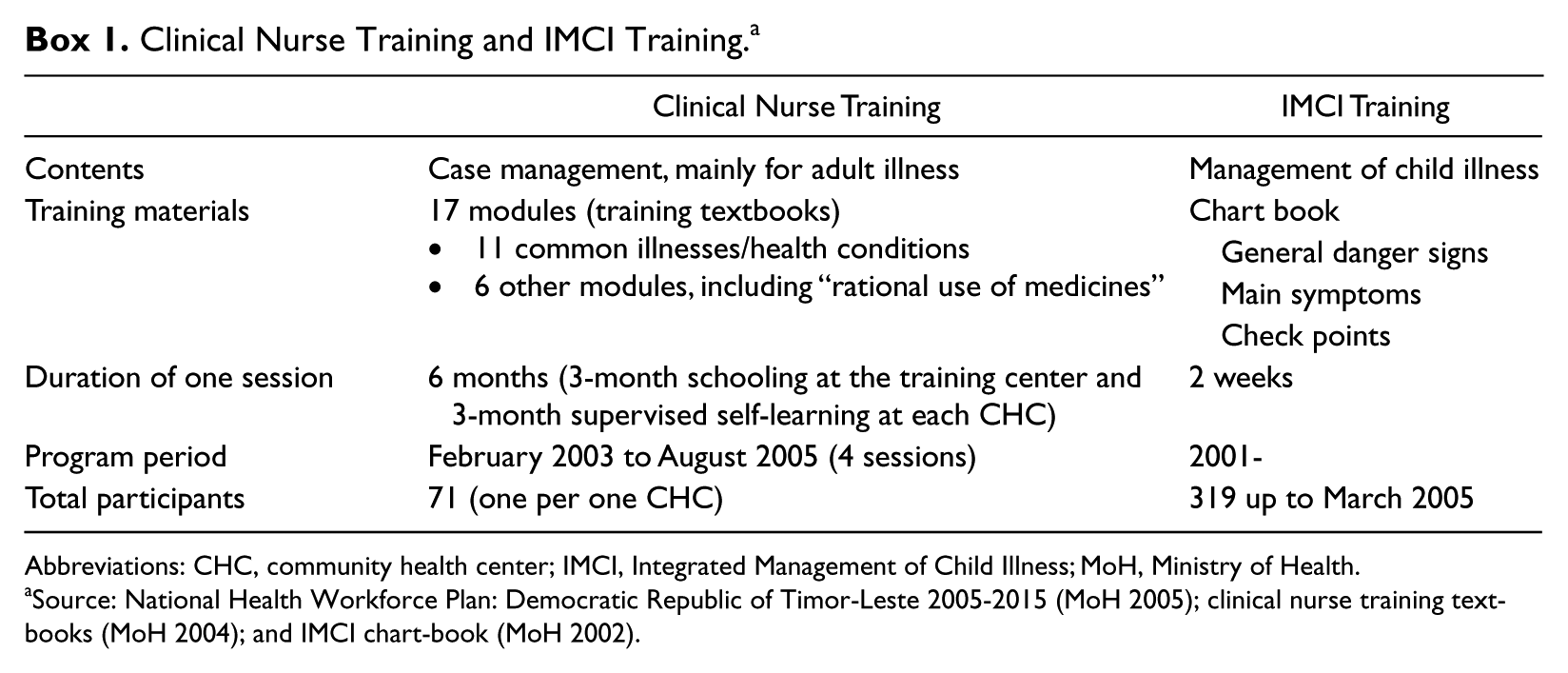
Abbreviations: CHC, community health center; IMCI, Integrated Management of Child Illness; MoH, Ministry of Health.
Source: National Health Workforce Plan: Democratic Republic of Timor-Leste 2005-2015 (MoH 2005); clinical nurse training textbooks (MoH 2004); and IMCI chart-book (MoH 2002).
The aim of this study was to investigate the use of medicines and examine adherence to STGs in Timor-Leste during the early stage of the nation’s new health system development.
Methods
Study Design
A cross-sectional study was conducted as the quantitative element of mixed methods research. 15 The qualitative element of the original research has been published elsewhere. 16 The quantitative methods used in this study were closely based on the well-established methods that had been developed by the International Network for the Rational Use of Drugs (INRUD) and the World Health Organization (WHO) and was published by the WHO in 1993. 17
Sampling
Two-stage sampling was applied: CHCs for the first stage and cases for the second stage. CHCs that were categorized as “level 2” at the time of sampling (hereafter CHCs) were targeted. Twelve of the 56 CHCs were excluded from the study, including those in the capital city and enclave district and those where the pretest had been conducted. Twenty CHCs were randomly sampled from the remaining 44 CHCs. The selected CHCs, shown in Figure 1, were visited by the principal investigator and 8 Timorese data collectors from February 2006 to August 2006.
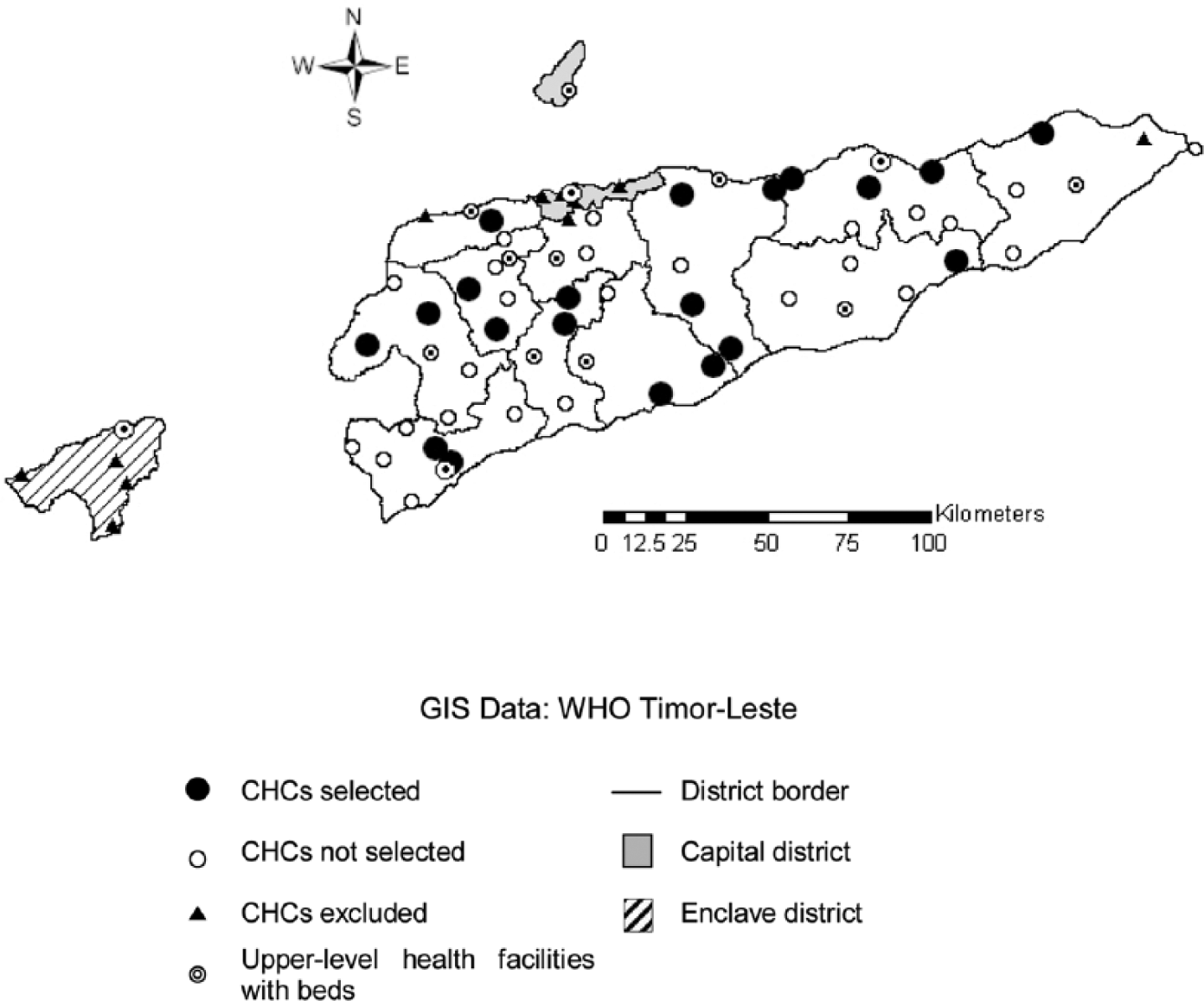
Selected CHCs and other health facilities in Timor-Leste when data were collected.
For the second-stage sampling, 2 methods were used. In each CHC, 100 cases were collected from patient registration books in 2005 by systematic random sampling (retrospective data). Furthermore, 30 consecutive cases in each CHC were observed (prospective data). Checklists were used for each data collection method. All collected data were used to assess the use of medicines. For examining adherence to STGs, only the cases recorded with at least 1 of 3 target diseases (ARTIs, malaria, and diarrhea) were used. Since there was no equipment for gold standard diagnoses, the decision on whether a case included a target disease relied on records according to criteria set in advance.
Assessment of the Use of Medicines
Eight of the 12 core INRUD/WHO indicators were applied to assess the use of medicines, and an additional prescribing indicator was specifically included for this study. “Prescribing indicators” were evaluated using both retrospective data and prospective data, whereas “patient care indicators” and “facility indicators” were obtained only from prospective observations, due to the nature of data.
The sample sizes vary among indicators, based on the INRUD/WHO definitions. An “adequate label” was defined as one that included all 4 components: patient name, medicine name, dosage schedule, and duration of medication. Percentage of “patients with knowledge of correct dosage” was evaluated in 2 stages. A patient was counted as having correct knowledge of a medicine if he/she knew the dosage schedule, duration of medication, and medicine name. Furthermore, if the patient had accurate knowledge of all medicines taken home, he or she was considered to have correct knowledge. In addition to the indicator, questions were asked about the reason(s) for the antibiotic prescription and vitamin prescription to elicit additional information on patient’s knowledge. Thirty “key medicines” for a facility indicator were selected based on the essential medicines list for level 2 facilities, which has been published by the Ministry of Health (MoH), Timor-Leste.
Assessment of Adherence to STGs
Prescribing adherence to STGs was examined on the basis of the clinical nurse training textbooks and the IMCI chart book, both of which were published by the MoH, Timor-Leste. Prescription practices were compared with the record of “clinical decision making.” If all medicines that are indicated in the aforementioned STGs were prescribed and any medicines that are contraindicated in the STGs were not prescribed, the case was counted as adhering to STGs (see Box 2).
Criteria for Classification and Prescription.
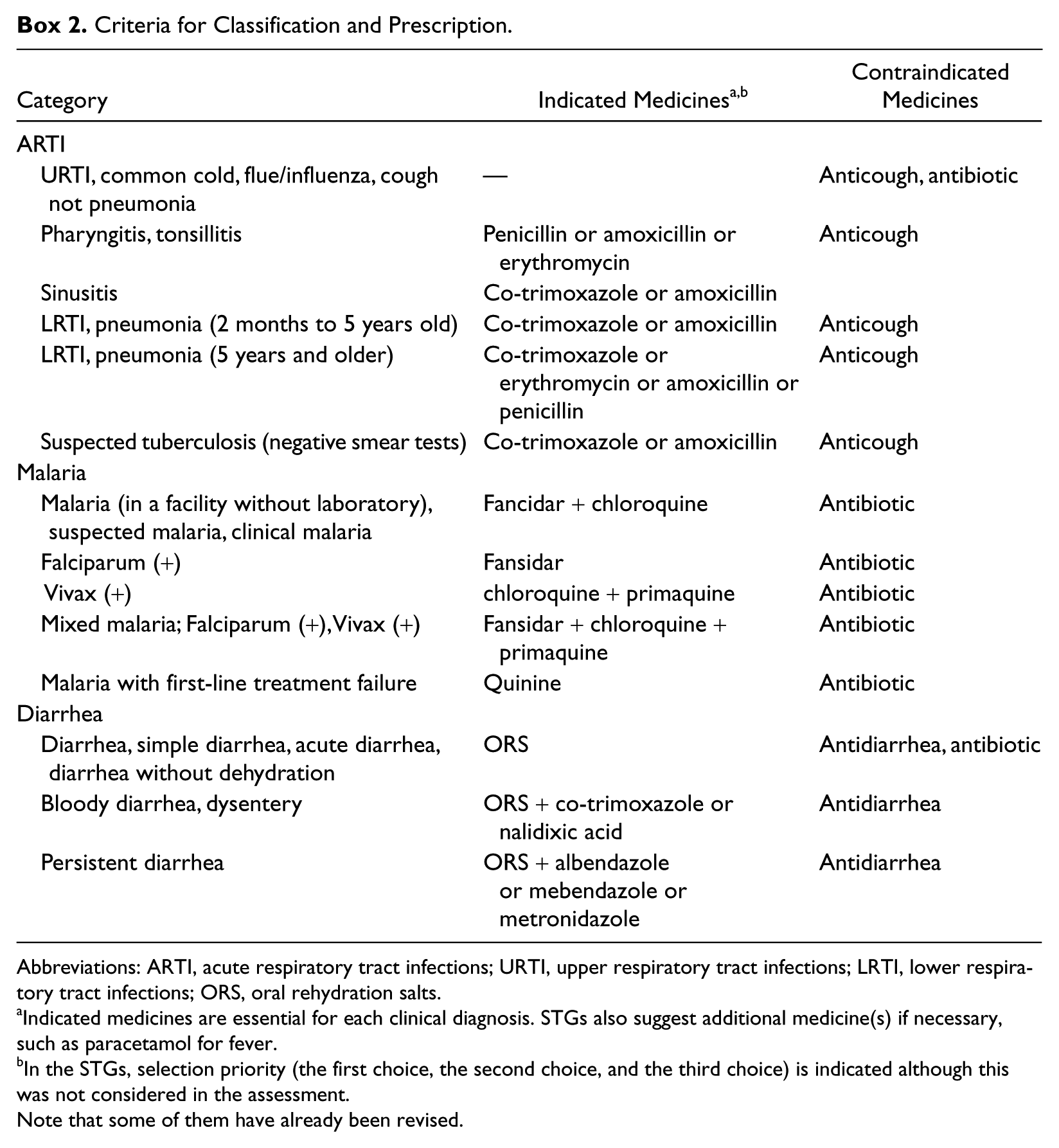
Abbreviations: ARTI, acute respiratory tract infections; URTI, upper respiratory tract infections; LRTI, lower respiratory tract infections; ORS, oral rehydration salts.
Indicated medicines are essential for each clinical diagnosis. STGs also suggest additional medicine(s) if necessary, such as paracetamol for fever.
In the STGs, selection priority (the first choice, the second choice, and the third choice) is indicated although this was not considered in the assessment. Note that some of them have already been revised.
Statistical Analysis
Three prescribing indicators were analyzed according to the training received by a nurse/midwife who prescribed the medication (hereafter prescriber) by using the Wilcoxon rank-sum test.
Prescriber’s individual adherence was analyzed by prescriber characteristics (age group, sex, occupational category, work experience, attendance of clinical nurse training, and attendance of IMCI training), and CHC’s overall adherence was analyzed by CHC characteristics (population size in the catchment area, annual cases per person, number of health personnel, percentage of people trained, total period of training per person, and availability of key medicines) by using the Wilcoxon rank-sum test.
Furthermore, influential factors of individual adherence were examined. First, univariate analyses were performed. The odds ratio for each of the prescriber characteristics was investigated, taking account of prescriber clustering. Logistic regression analyses, using random effects, were performed. Next, to explore possible confounders, the odds ratio for a possible influential factor, adjusted by each of the other variables, was calculated. If the odds ratio was changed when adjusted by a variable, the variable was considered as a possible confounder and was then included in the final model. Evidence of the possible effect of modification by the variable was also examined using likelihood ratio tests. In the final model, the odds ratio was calculated, taking account of identified confounders and prescriber clustering.
In the retrospective data, there was no information on prescribers. Therefore, analyses of prescribing indicators and adherence according to prescriber used only prospective data. Because a new policy to allocate foreign doctors to level 2 CHCs was implemented during the data collection, cases managed by foreign doctors were unexpectedly included in some CHCs; however, such cases were excluded when the data were analyzed by prescriber.
Ethical Considerations
The research proposal was approved in advance by the Proposal Review Panel of the MoH, Timor-Leste, and the Research Ethics Committee of the London School of Hygiene and Tropical Medicine.
Results
Use of Medicines
The total number of cases from patient registration books (retrospective cases) was 1799. This number was less than we expected (2000) because patient registration books were not available in the conditions we needed at 2 CHCs and 1 record was invalid. The final number of observed cases (retrospective cases) was 583, whereas the planned number was 600 because we could not conduct the planned number of observations in 2 CHCs. Table 1 shows medicines use indicators in Timor-Leste.
Medicines Use Indicators in Timor-Leste.
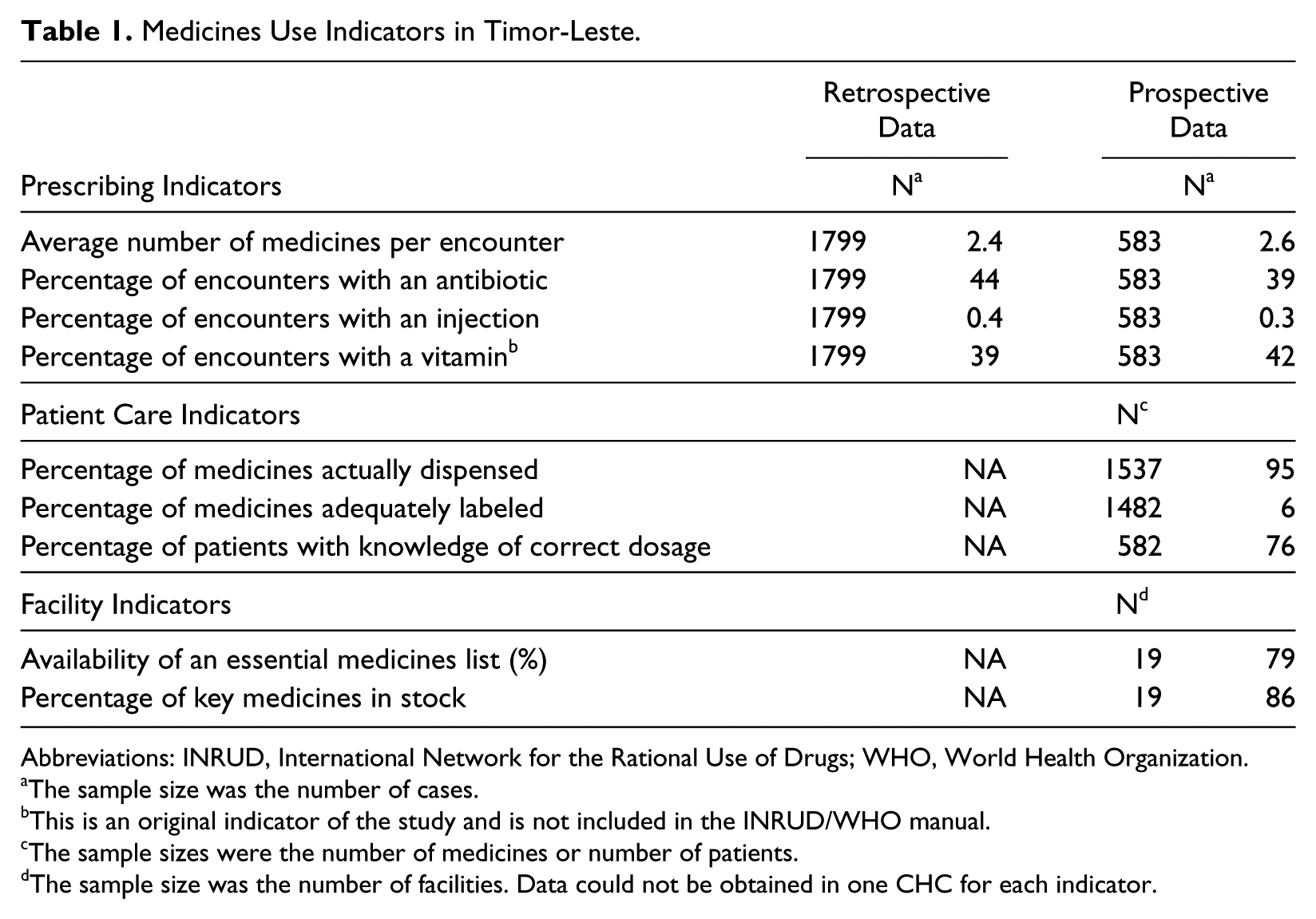
Abbreviations: INRUD, International Network for the Rational Use of Drugs; WHO, World Health Organization.
The sample size was the number of cases.
This is an original indicator of the study and is not included in the INRUD/WHO manual.
The sample sizes were the number of medicines or number of patients.
The sample size was the number of facilities. Data could not be obtained in one CHC for each indicator.
Of the 1537 medicines prescribed, 1461 (95%) were dispensed as prescribed; however, 42 kinds of medicines were excessively dispensed. Twenty-one medicines were taken at the dispensing counter. Among the 1482 medicines taken home, only 88 (6%) were adequately labeled. Of the 582 patients who took medicine home, 445 (77%) had correct knowledge of all the medicines. The comparisons in Table 2 show that patient knowledge of dosage schedules and duration of the treatment was better than the information provided in the labeling of these medicines.
Percentage of Medicines Labeled and Patients With Correct Knowledge by Component of Information.
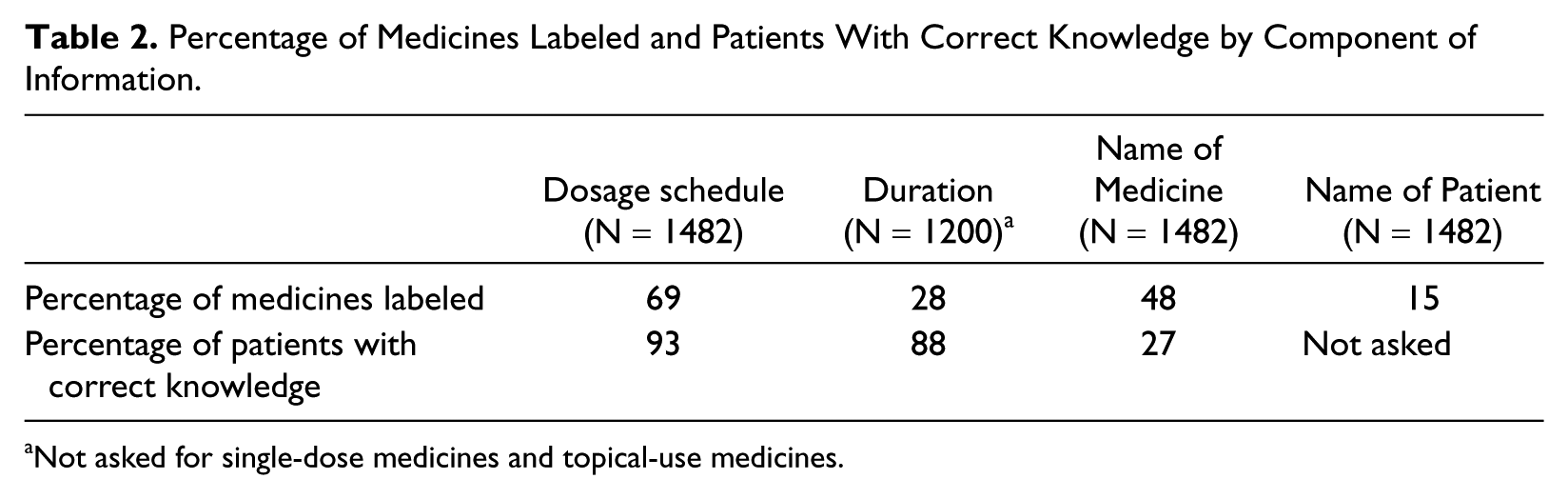
Not asked for single-dose medicines and topical-use medicines.
As shown in Figure 2, more than half of the patients who received antibiotics answered that antibiotics were given for their respiratory symptoms. Patients believed that vitamins could treat a variety of symptoms, such as respiratory symptoms and anorexia.
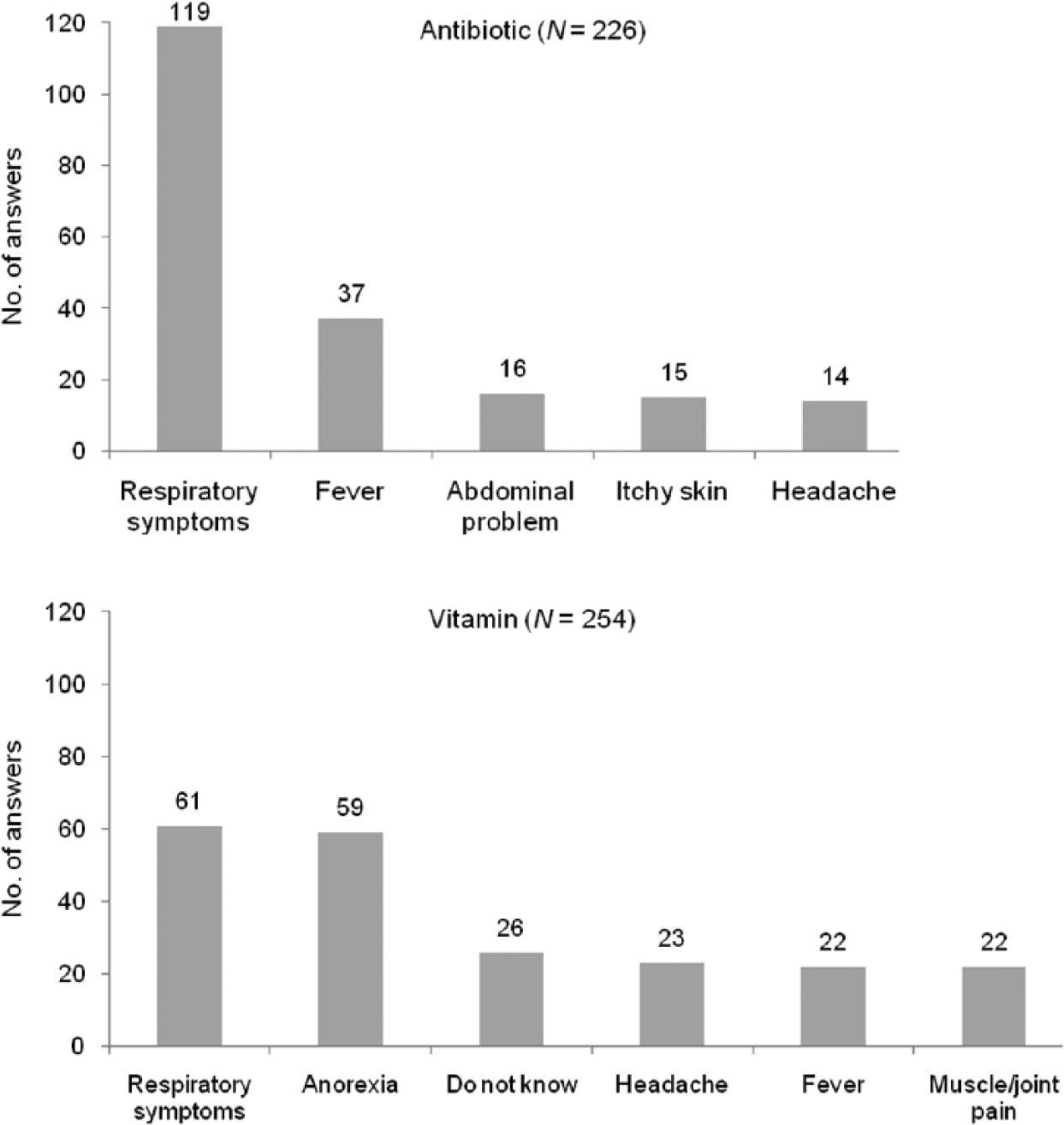
Top 5 reasons for prescription as understood by patients.
Three hundred fifty cases among the 583 observations were prescribed by 32 local nurses/midwives. Of these prescribers, 15 had attended clinical nurse training while 17 had not, and 22 had attended IMCI training while 10 had not. Table 3 shows 3 prescribing indicators analyzed according to prescriber training. Prescribers with clinical nurse training prescribed significantly fewer antibiotics than those without clinical nurse training (P < .01). However, the 2 other prescribing indicators (average number of medicines and vitamin prescriptions) did not show a significant difference between the groups. None of the 3 prescribing indicators showed a significant difference between the prescribers who had attended IMCI training and those who had not.
Comparison of the Prescribing Indicators by Prescriber Training.
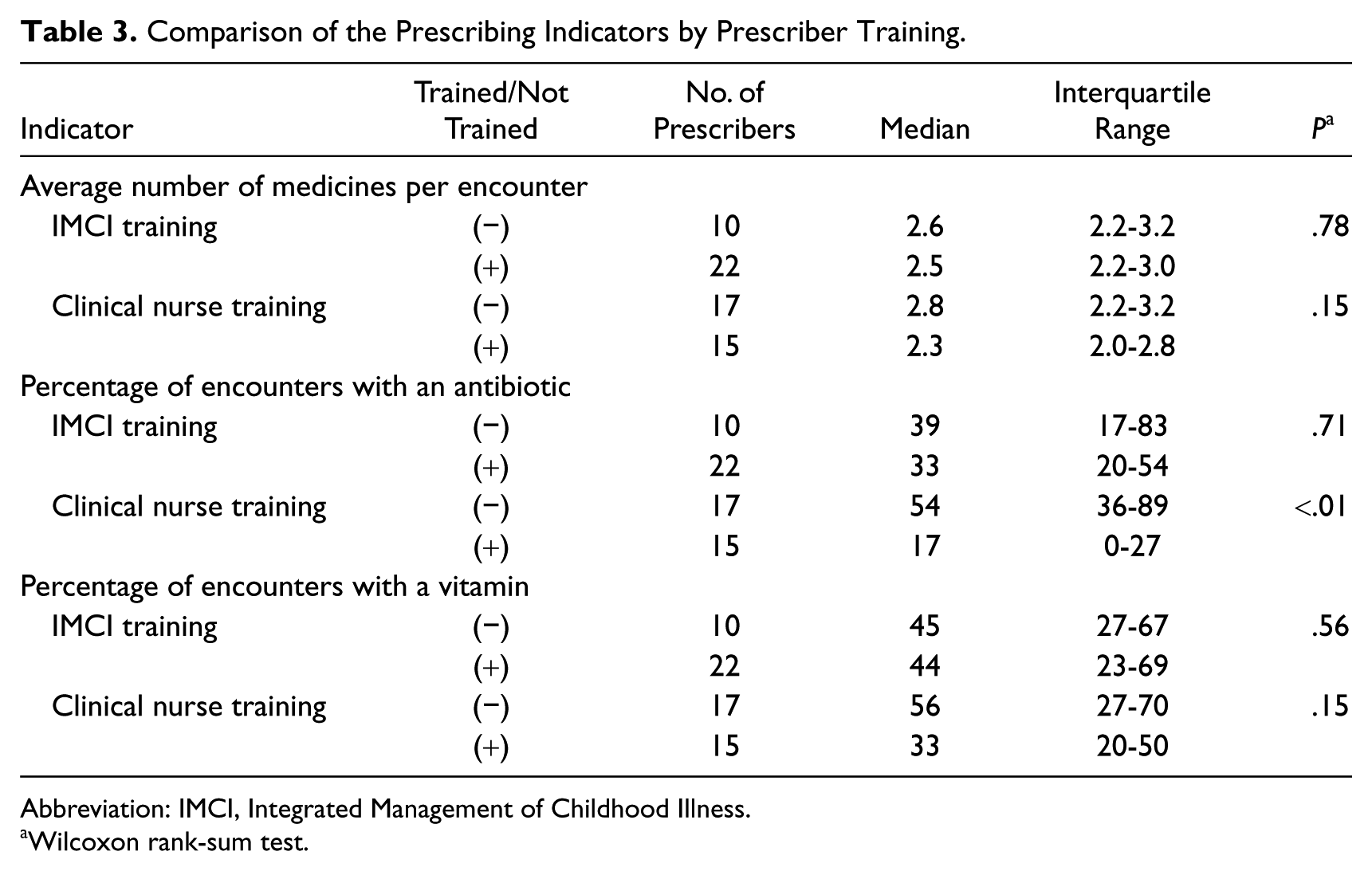
Abbreviation: IMCI, Integrated Management of Childhood Illness.
Wilcoxon rank-sum test.
Adherence to STGs
Numbers of cases that involved at least 1 of the 3 target diseases (ARTIs, malaria, and diarrhea) were 1145 out of 1779 retrospective cases and 380 out of 583 prospective cases. Prescribing adherence to STGs of these 3 target diseases was calculated to be 56% of all the cases with any target disease, either from retrospective data or from prospective data (641/1145 and 213/380, respectively).
Among 380 prospective cases with a target disease, 240 were managed by 32 local nurses/midwives. Table 4 shows a comparison of the median and interquartile range of individual adherence according to prescriber characteristics and the P value by the Wilcoxon rank-sum test. Of the prescribers, those who had attended clinical nurse training showed significantly higher adherence to STGs than those who had not attended such training (P < .01). Furthermore, a higher level of adherence was observed among the prescribers with both kinds of training than among those with only either clinical nurse or IMCI training (Figure 3). However, due to the small sample size in each group, it was difficult to establish a statistical difference. There was no significant difference in CHC’s overall adherence analyzed in terms of each CHC characteristic examined.
Comparison of Prescribing Adherence (%) by Prescriber Characteristic.
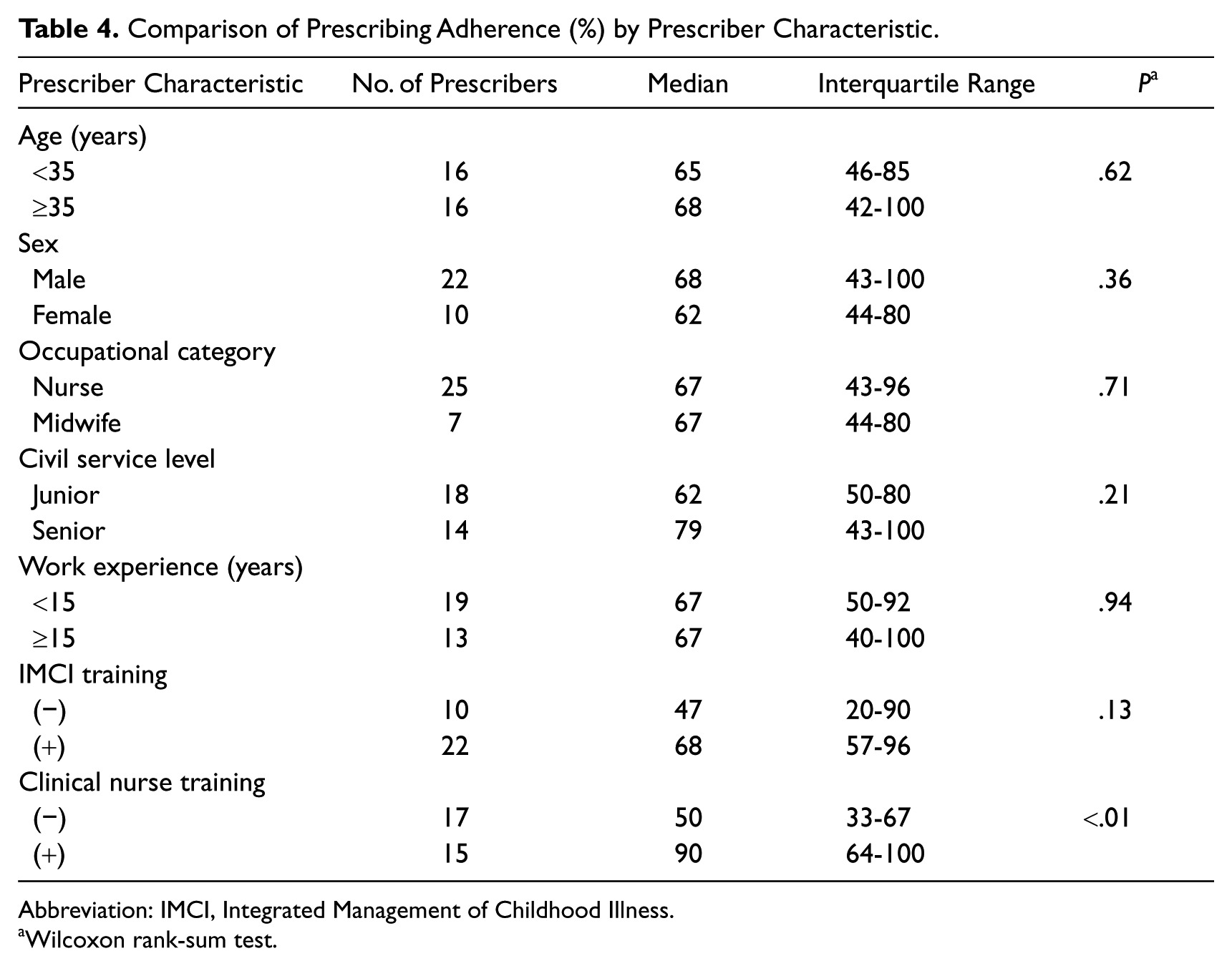
Abbreviation: IMCI, Integrated Management of Childhood Illness.
Wilcoxon rank-sum test.
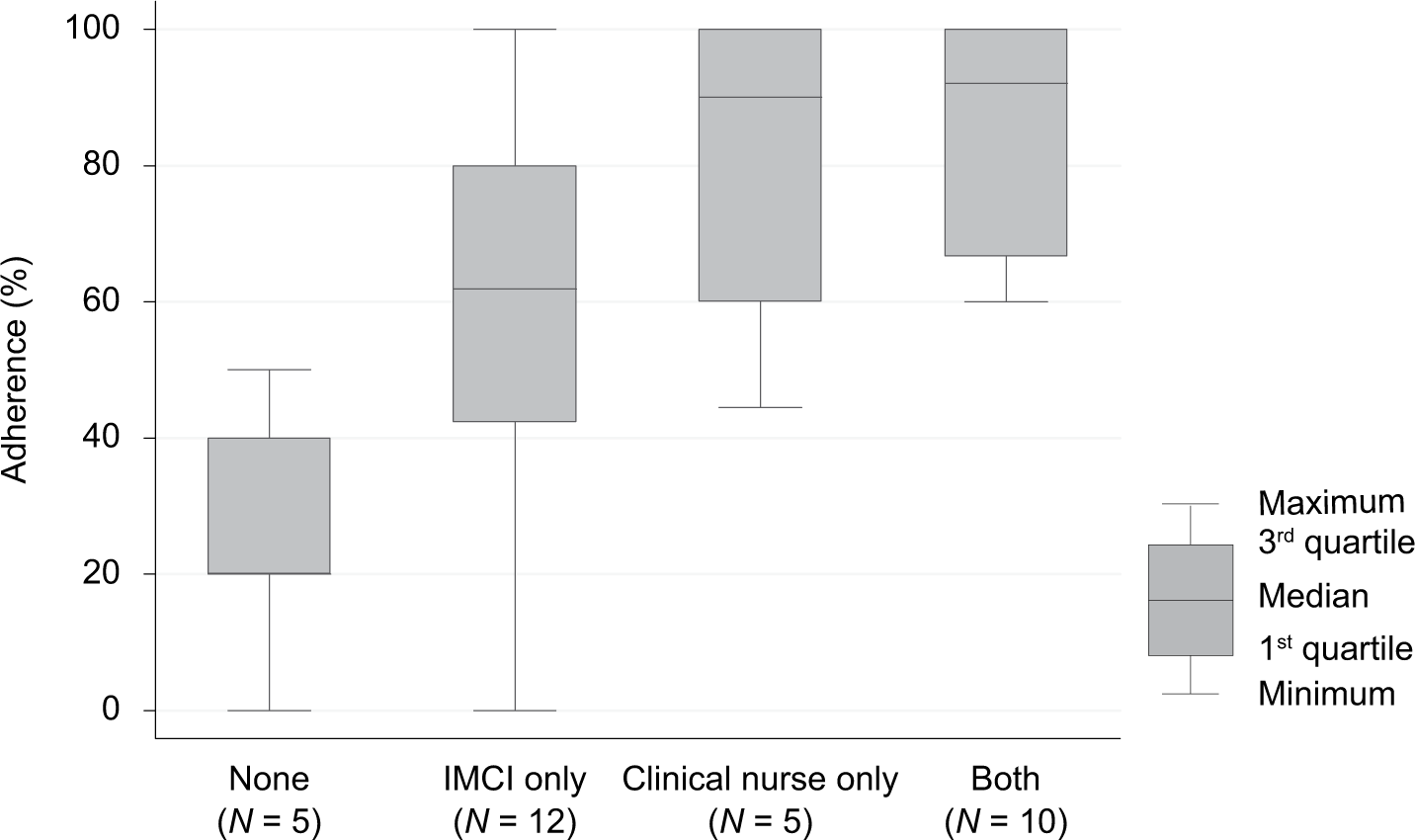
Comparison of prescribing adherence by prescriber’s training.
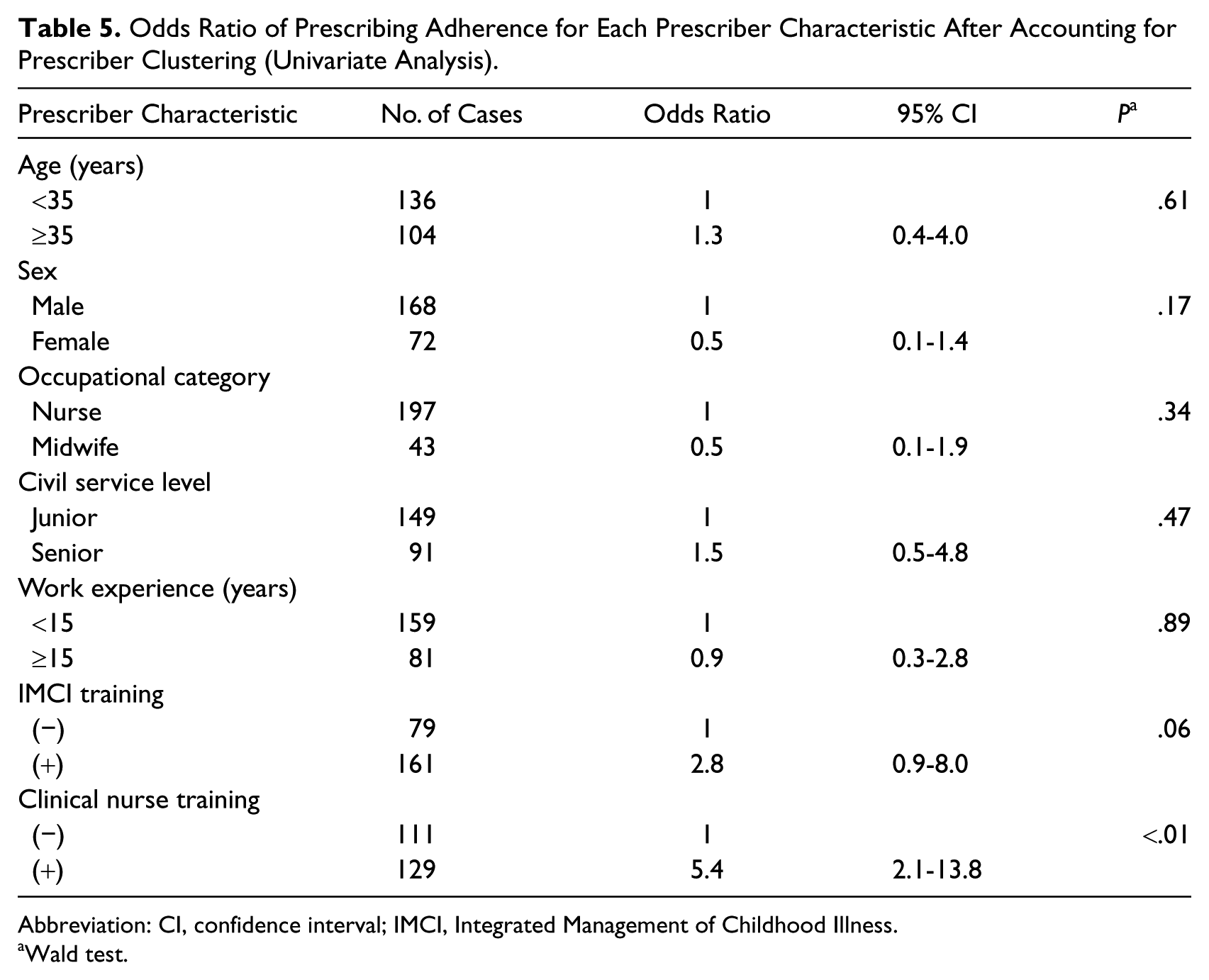
Table 5 shows the odds ratio of prescribing adherence for each prescriber characteristic after accounting for prescriber clustering. Prescriber’s clinical nurse training was considered as the most influential factor. It was found that sex, civil service level, and work experience were possible confounders for the association between prescribing adherence and prescriber’s clinical nurse training. There was no evidence of effect modification between prescriber’s clinical nurse training and each of these 3 variables. In the final model, after accounting for the confounders and prescriber clustering, the adjusted odds ratio of prescribing adherence for clinical nurse training was 6.6 (95% confidence interval [CI] = 2.5-17.6) at a significant level (P < .01). As shown in Table 5, there was a weak association between prescribing adherence and prescriber’s IMCI training by univariate analysis (P = .06). Prescriber’s clinical nurse training was considered as the possible confounder. The adjusted odds ratio of prescribing adherence for prescriber’s IMCI training after accounting for prescriber’s clinical nurse training and prescriber clustering was 2.9 (95% CI = 1.2-6.8) at a significant level (P = .02).
Odds Ratio of Prescribing Adherence for Each Prescriber Characteristic After Accounting for Prescriber Clustering (Univariate Analysis).
Abbreviation: CI, confidence interval; IMCI, Integrated Management of Childhood Illness.
Wald test.
Discussion
The number of medicines per encounter and percentage of encounters with an antibiotic prescribed in Timor-Leste were similar to the median of the studies reported to the WHO. 18 The use of injections was extremely low. Overall, the results from Timor-Leste did not imply serious overprescription.
In comparison with a study from Nepal, in which it was calculated from morbidity data that 1.3 to 1.4 items per patients should be prescribed and that 22% to 27% of the patients need antibiotics, 19 slightly excessive medicines might have been prescribed in Timor-Leste. Although the INRUD/WHO indicators cannot be used to ascertain whether the obtained results are correct or appropriate, they help identify a tendency toward heavy use of medicines so that the next action, either a further investigation or an intervention, can be taken. 17
The low level of injection use in Timor-Leste is encouraging, considering that unsafe and unnecessary injections have been widely reported. 20 Timor-Leste’s essential medicines list (EML) for level 2 CHCs lists injections as “E-medicines” (mainly antibiotics and antimalarials), which can be used as the initial treatment for severely ill patients while referring them to a higher level facility. 21 Thus, only limited kinds and numbers of injections were procured at these CHCs. The national EML specifies that the initial treatment and referral of severely ill patients should be guided by the clinical nurse and IMCI programmes 21 and that the potential harm caused by unnecessary injections should be repeatedly taught during clinical nurse training and IMCI training. The low percentage of injection use in Timor-Leste was realized by combining EML development with the medicine procurement system, as well as with the health system structure, including the referral system, and STGs with the related training programs. In reality, however, patients may have difficulties with referral to an upper level facility, which remains an issue.
The low percentage of adequate labeling might have influenced patient adherence because labeling of a medicine bag has been identified as one of the measures to improve patient knowledge and adherence.22,23 Patient knowledge is considered a prerequisite for patient adherence, 24 but it does not always guarantee patient adherence to the prescription. 25 Correct knowledge of medicines measured in this study relied on only short-term memories, and patient adherence throughout the treatment was unknown. Given the low literacy rate in rural Timor-Leste, labeling might not have had an influence on patient adherence. The ability of nurses/midwives to encourage patients to take medicines properly at home, which was not assessed in this study, should be important.
The study showed strong evidence that clinical nurse training was associated with lower use of antibiotics and greater adherence to STGs. Prescribing adherence to STGs was associated with IMCI training, too. A previous research in Cameroon, which used the INRUD/WHO methods and undertook similar analyses, also identified that training and supervision were effective methods of promoting appropriate medicines use. 26 Timor-Leste’s clinical nurse training was, however, more extensive than what was suggested by the Cameroon study to influence complex prescribing behaviors. The contents, methods, and duration of training should be carefully designed according to the local needs and reality.
A value of STGs in Timor-Leste was their comprehensive strategy to cover multiple prioritized illnesses in nationwide programs, when considering a previous study, which found that in-service training of case management for one specific disease may negatively influence the quality of care for another disease. 27 Previous studies have shown that multifaceted interventions are required so that STGs are effectively applied in practice.6,9,10 This was also suggested in a review on the effect of guidelines in nursing and other professionals allied to medicine. 28 This study was observational and did not evaluate the effect of training interventions; however, by combining the quantitative results with the qualitative element of mixed methods research, which was conducted alongside this cross-sectional study, it was revealed that training, in particular clinical nurse training, positively influenced knowledge of and attitudes toward the STGs, as well as their prescribing practice. 15 As already discussed in relation to the low level of injection use, the STGs existed across various programs. Standardized practices recommended by other programs are integrated into the STGs. Development and dissemination of STGs within a policy framework is believed to be a key factor.
Interestingly, in spite of the overall positive results, vitamins were unnecessarily prescribed regardless of the training. Furthermore, the majority of patients knew that the prescribed medicine was a vitamin but mistakenly believed that it would treat symptoms such as respiratory problems and anorexia. The concurrently conducted qualitative study revealed nurses’/midwives’ misunderstandings about vitamins even though they showed good knowledge regarding other STGs. 15 Similar misunderstandings about vitamins to those of the patients were revealed in interviews with nurses/midwives. On integrating these findings, it was assumed that patients and local prescribers shared the same incorrect knowledge. A previous study showed that prescriptions with more items are associated with poorer dispensing practice and patient knowledge, which suggests that even biomedically less harmful medicines, such as vitamins, can be risky. 29 Unnecessary vitamin prescription should therefore be avoided. Although vitamins are not recommended either in the clinical nurse training textbooks and in the IMCI chart book, contraindications for and harms of vitamins are not emphasized as much as antibiotics and injections. Therefore, training might have failed to control vitamin over prescription.
Nurses/midwives are expected to play a role in delivering appropriate information on medicines. These personnel have always responded to the changing health care needs and demands. 30 In many resource-limited settings, nurses/midwives prescribe medicines to provide essential health services and fill a gap in health care; however, strong political will to support this caregiving and adequate training for the role are often lacking.30,31 In this study, Timor-Leste’s STGs for nurses/midwives at the PHC level, whose pre-service education was basic, show potential. The responsibilities of nurses/midwives after new medical doctors are appointed in rural communities will be a new challenge in Timor-Leste.
Conclusions
The experience in Timor-Leste showed favorable results for the use of medicines and adherence to STGs among nonphysician health professionals at the PHC level. Training was effective to reduce antibiotic use and increase adherence to STGs. When strategically developed and introduced, STGs have potential value in basic health care delivery, including appropriate use of medicines, in resource-limited communities.
Footnotes
Acknowledgements
We are grateful to the Ministry of Health, other collaborators, and respondents in Timor-Leste, as well as the 11 Timorese research assistants.
Authors’ Note
This article is based on the DrPH thesis of the principal investigator, which was submitted to the London School of Hygiene and Tropical Medicine. The work was supported by academic advisors (Dr Gill Walt, Dr Stuart Anderson, Dr James Hargreaves, and Dr Julia Mortimer).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed the receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Takagi Fund for Citizen Science, the Dr Gordon Smith Travelling Scholarship, and the Toyota Foundation.