
Abstract
Even though 2-dose measles vaccination coverage rate was maintained at more than 95%, the largest measles outbreaks since 1996 still occurred in Wuhu city, P R China. A total of 916 cases were reported during 2005-2010. The annual incidence was 6.7 cases per 100 000 population with the peak incidence of 17.6 cases per 100 000 population in 2008. The highest age-specific incidence rate was 222.1 per 100 000 population and occurred in infants aged between 8 and 12 months; the second was 151.9 per 100 000 population in infants aged <8 months. Also, 200 cases occurred in those aged to 22 to 30 years old, accounting for 21.8% of total cases, with the age-specific incidence being 12.8 per 100 000 population. The characteristics related to age distribution have changed in recent measles outbreaks. It underlines the need for vaccination of susceptible young adults and timely administration of the first dose of the measles vaccine.
Introduction
The World Health Organization Regional Office for the Western Pacific has set 2012 as the target for elimination of measles in the region. To attain the goal, some control measures were implemented in China, including attaining and maintaining high vaccination coverage (95% with 2 doses of the measles vaccine), strengthening surveillance systems by rigorous epidemiological and laboratory investigation of all suspected cases, and implementing supplementary vaccination activities for older children and adolescents.
The measles vaccine was introduced in 1967 in China, and routine administration was started in the early 1980s; the 2-dose schedule of the measles vaccine (first dose at 8 to 11 months and second dose at 7 years) was introduced in 1985, and the age for the second dose was lowered to 4 years in 2000 (containing the measles antigen vaccine such as the MMR [measles-mumps-rubella] vaccine or the MR [measles-rubella] vaccine, also recommended since then) and then lowered to 18 to 24 months in 2006. During the prevaccine era (1956-1965), the overall annual incidence of measles in China was 772.4 per 100 000 population, and the mortality rate was 11.3 per 100 000 population. After the 1990s, the incidence of measles decreased substantially. In 1995, the annual incidence of measles was 4.84 per 100 000 population; it decreased by 98% when compared with the rate of 250 per 100 000 population in 1978. 1 Nevertheless, since 2005, an increasing trend in the incidence of measles in China was observed, accompanied by an increased incidence. The proportion of measles cases in those aged <8 months and 8 to 11 months was more than 10%, and the incidence in persons aged 25 to 30 years old was also high. 2
In Wuhu city, which is located in the southeastern region of the Chinese province of Anhui, from 1996, the coverage of vaccine against measles in children has been maintained at more than 96%, and the lowest annual incidence of 0.6 per 100 000 population was in 1999, which was maintained for more than 10 years. 3 This changed from 2005, and could be said to signify a “yellow light” for the present prevention and control strategies. In this study, we collected surveillance data from January 1, 2005, to December 31, 2010. The data show that the characteristics related to age distribution were changing significantly combined with an increased incidence.
Methods
Surveillance of Measles Cases
In China, measles is mandatorily notifiable. Information about the patients is collected by the local Chinese Center for Disease Control and Prevention (CDC) staff with a uniform questionnaire that includes demographic characteristics, clinical presentations, medications, vaccination status, and so on. Blood samples are taken when a case meets the criteria for a probable case. 4 If an initial specimen, obtained when a patient who met the clinical criteria for admission into a hospital/health center, tested negative for IgM antibodies against measles, a second serum sample would be obtained 4 weeks later. Blood samples were drawn into siliconized disposable plastic tubes. Antimeasles IgM/IgG antibody was measured using a commercially available ELISA kit. All tests were carried out in duplicate. Samples positive for IgM antibodies or with significant (at least 4 fold) increases in IgG antibodies titer were classified as laboratory-confirmed cases. A probable case that had noncontributory or no serological testing but was clearly epidemiologically linked to a confirmed case was defined as a clinical case. 4
Information about measles death was also collected by the local CDC. A measles death was defined as the death of a person with measles within 30 days of rash onset, unless the death was unrelated to the disease.
Surveillance of Immunization Coverage
The vaccination coverage was estimated based on data from the survey conducted in our city in October or November every year. Stratified 2-stage cluster sampling was used from 3 counties and 4 districts in Wuhu city. In the first stage, 25 villages were selected randomly from all villages (or communities) in each county (or district). In the second stage, 10 children aged 1 to 2 years were selected randomly from each selected village (or community); a total of about 250 children would be surveyed in each county or district. The second dose of measles vaccination was investigated in the 2- to 4-year-old age group (10 children per village) in 10 to 15 villages (or communities) from those selected.
The local CDC staff visited the parent or guardian of each selected child to complete a uniform, structured questionnaire, including demographic characteristics, date of the vaccination, and so on.
Statistical Analyses
Population estimates for the years 2005 through 2010 were based on the data obtained from the Wuhu CDC. A total of 9 groups were formed based on age: group 1 (age less than 8 months) and group 2 (age ≥8-12 months) were determined according to the immunization schedule of measles vaccination in China (the first dose of measles vaccine is recommended at the age of 8 to 12 months). Group 3 (age ≥1-3 years), group 4 (age ≥3-6 years), group 5 (age ≥6-12 years), group 6 (age ≥12-18 years), and group 7 (aged ≥18-22 years) were determined according to the main levels of education in China. In group 8, the age was between 22 and 30 years and included women of childbearing age; those in group 9 were 30 years and older.
The incidence rates (new cases per 100 000 population) and age-specific incidence were calculated according to year. The age-specific incidence was estimated by dividing the number of measles cases by the number of persons in each age group and calculated according to year. The proportion of the cases was calculated by age groups.
Ethical Considerations
This study was approved by The Research Ethics Committee of Guangdong Medical College.
Results
A total of 1296 probable cases of measles were reported from January 1, 2005, to December 31, 2010, among persons residing in the Wuhu area (total 2010 population: 2 263 641). In all, 471 cases were eliminated, and 916 cases of measles were confirmed, which met the criteria of either confirmed or clinical cases. According to the case definitions, 753 (82.2%) were cases confirmed by laboratory examinations, and 163 (17.8%) were defined as clinical cases. The number of cases increased in 2005; 157 cases were reported, and the epidemic reached its peak in March 2005 (73 cases). Then they decreased to 61 and 55 cases a year in 2006 and 2007, respectively. However, a large measles outbreak with a total of 401 cases occurred in our area in 2008, and the increase in trend continued from January to the peak in May (127 cases); the annual incidence rate reached 17.4 per 100 000 population. In 2009, a similar trend was observed with the outbreak peaking in April (52 cases); 224 cases were reported in the whole year, and the annual incidence rate was 9.4 per 100 000 population. The outbreak abated in 2010; only 18 measles cases were reported, and the annual incidence rate was 0.8 per 100 000 population (Table 1). The average annual incidence from 2005 to 2010 was 6.7 per 100 000 residents. No death was reported during the study period.
Incidence of Measles in Wuhu City Per 100 000 Population During 2005-2010 (Total and by Age Group).
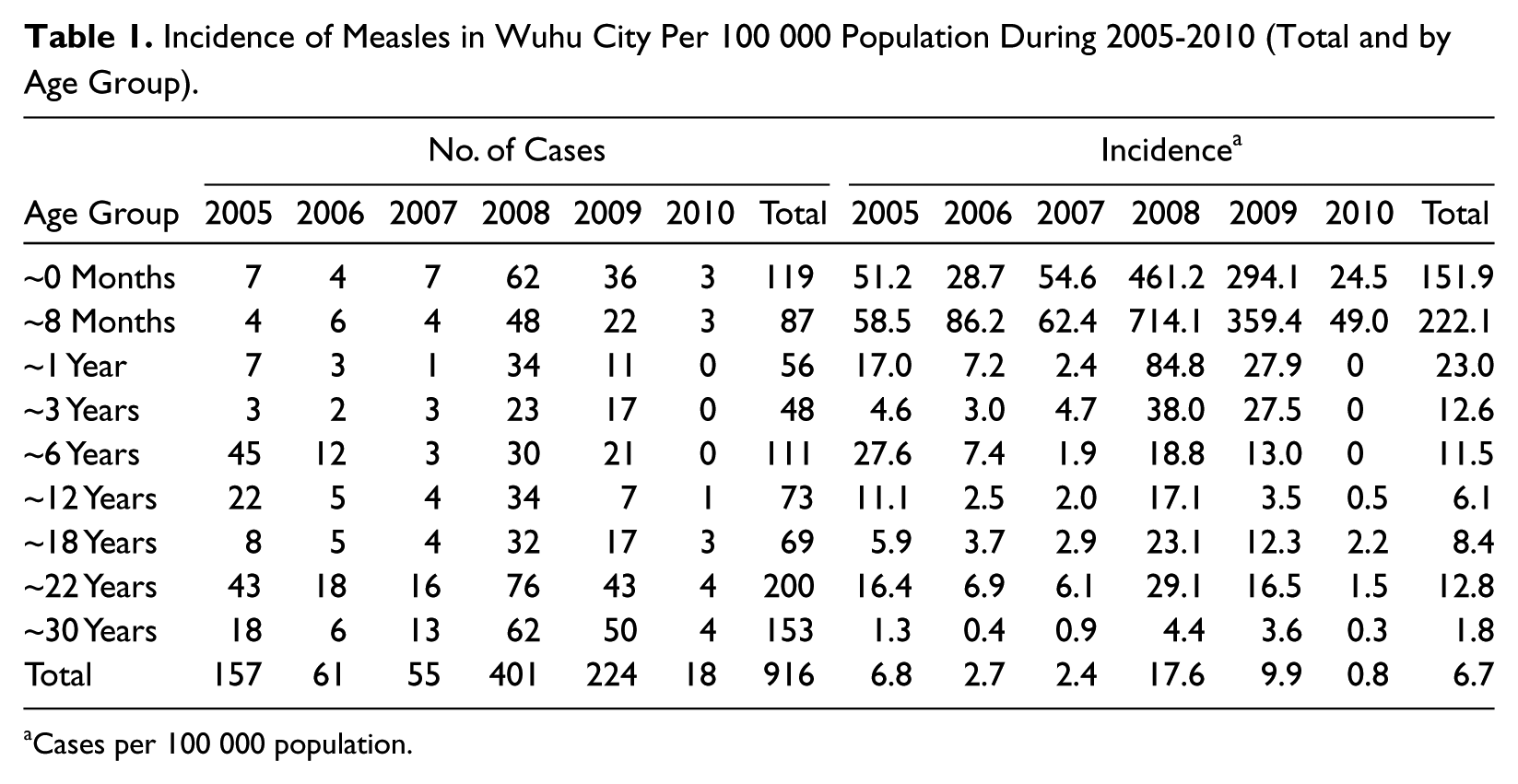
Cases per 100 000 population.
The median age of the 916 patients was 14.5 years (ranging from 18 days to 66.0 years). By age group, the age-specific incidence in children age between 8 and 12 months was highest (222.1 per 100 000 population), followed by that in children <8 months old (151.9 per 100 000 population). Among those younger than 1 year, 119 were younger than 8 months (accounting for 57.8% of the cases in those <1 year old). The number of cases increased dramatically after the infants reached 5 months of age: there were 107 cases in infants aged between 5 and 8 months (accounting for 51.9% of the cases in those <1 year old; Figure 1). There were 200 cases that occurred in those aged ≥22 to 30 years, accounting for 21.8% of the total cases; the age-specific incidence was 12.8 per 100 000 population.
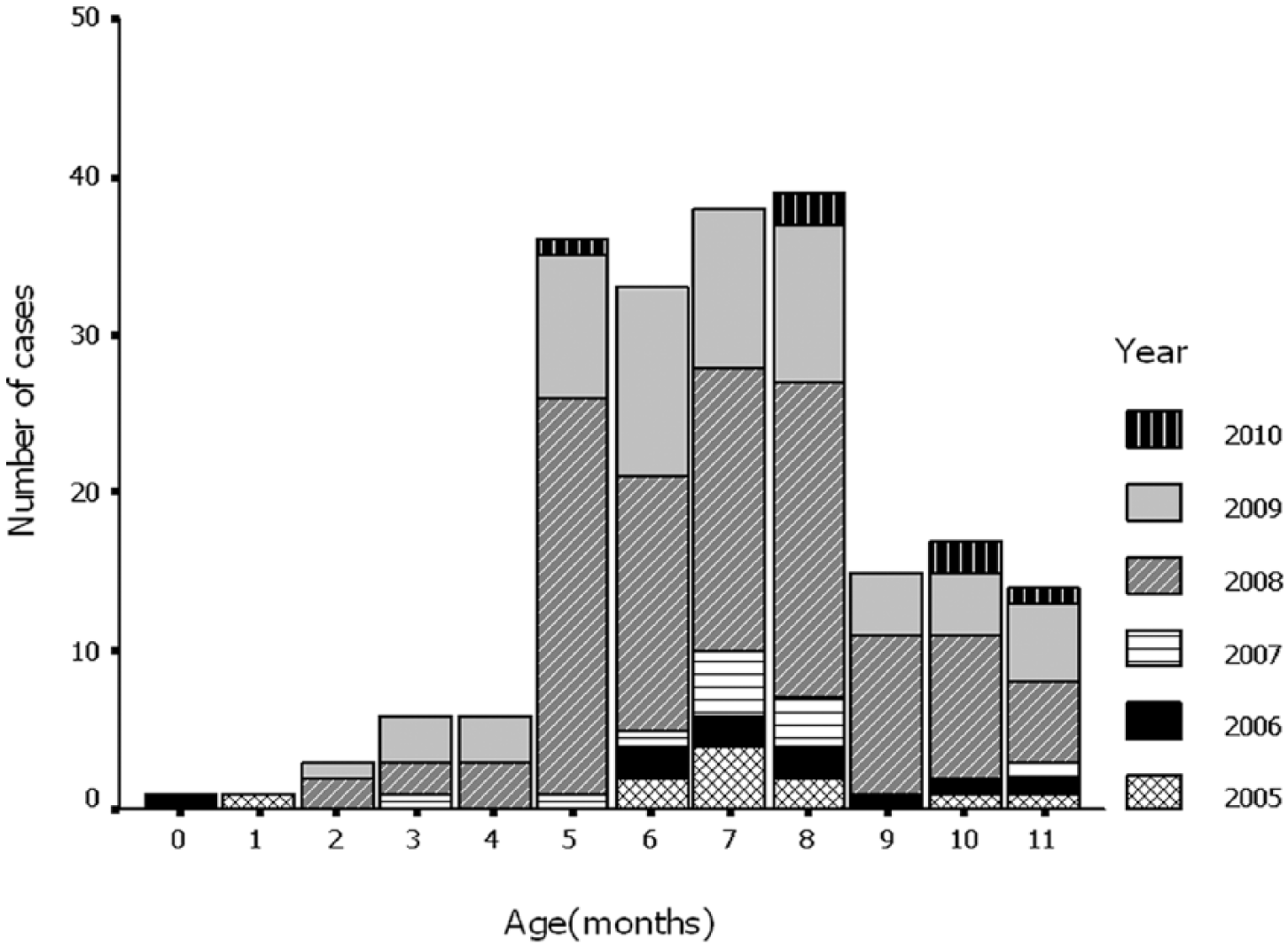
Number of measles cases by age (those <1 year old).
In the outbreak between 2008 and 2009, the number of cases in infants aged <1 year increased remarkably—a total of 168 cases (26.9%) occurred in this age group. The age-specific incidence in infants aged <8 months was 461.2 and 294.1 per 100 000 in 2008 and 2009, respectively. The incidence reached 714.1 and 359.4 per 100 000 population in the 8- to 12-month-old age group in the same 2 years. Also, 119 cases (19.0%) occurred in those aged ≥22 to 30 years in the 2 years; the age-specific incidence was 22.4 and 12.7 per 100 000 population, respectively (Table 1).
In all, data on vaccination status were available for only 516 cases (57.5%), and most of them were obtained through patient or parent recall. Of these 400 patients (excluding 116 cases among those <8 months), 180 (45.0%) reported that they had had at least 1 doses of a measles-containing vaccine. In 8- to 12-month-old infants, just 54.5% (30/55) had been immunized with a measles-containing vaccine (Figure 2).
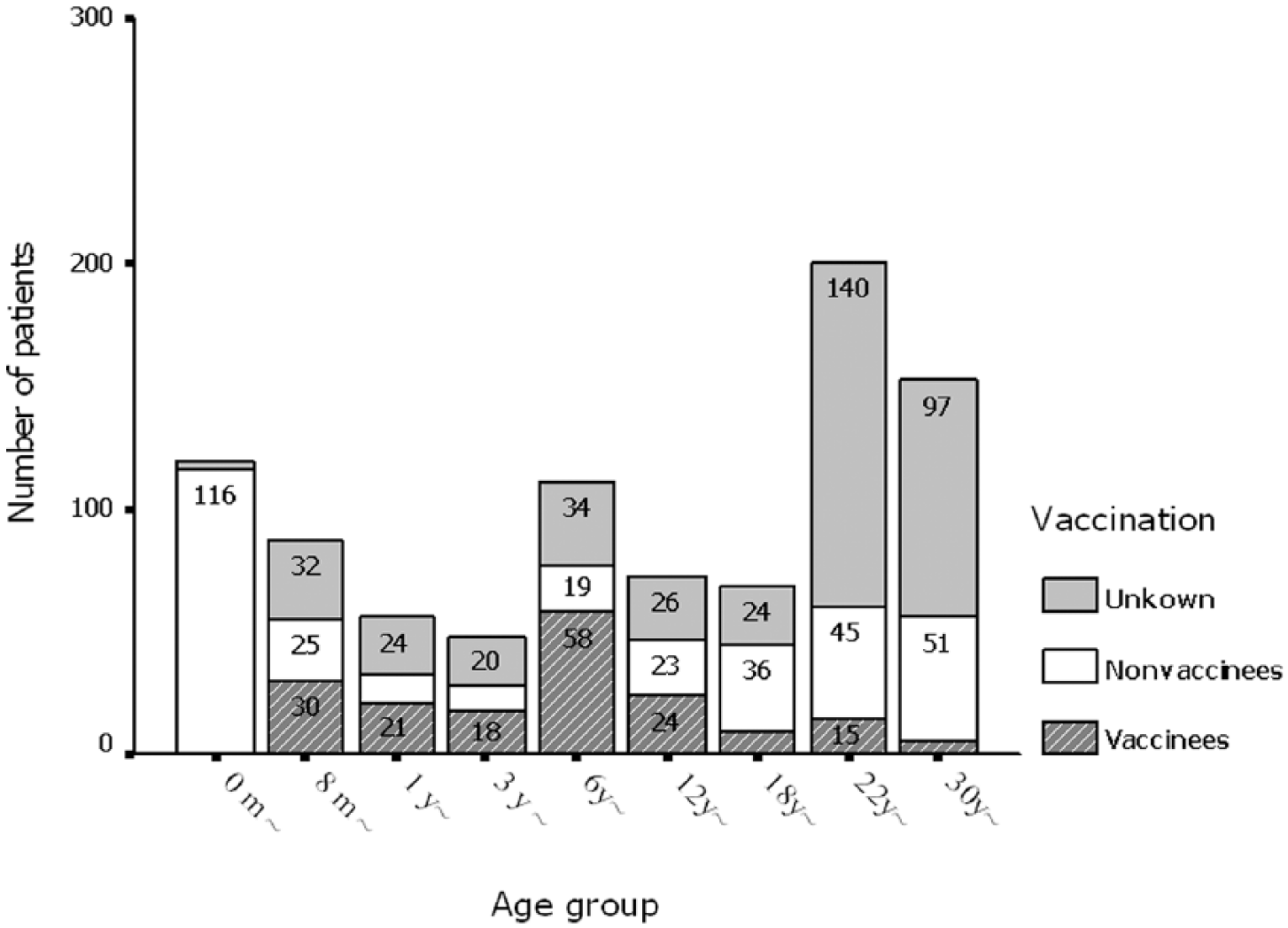
The age distribution of patients according to the history of measles vaccination.
In Wuhu city, the vaccination coverage was 97.8% (range 96.2%-99.6%) for the first dose of a measles-containing vaccine, and it was 96.4% (range 95.3%-98.2%) for the second dose between 2005 and 2010 (Table 2).
The Measles Vaccination Coverage Rate in Wuhu City, 2005-2010.
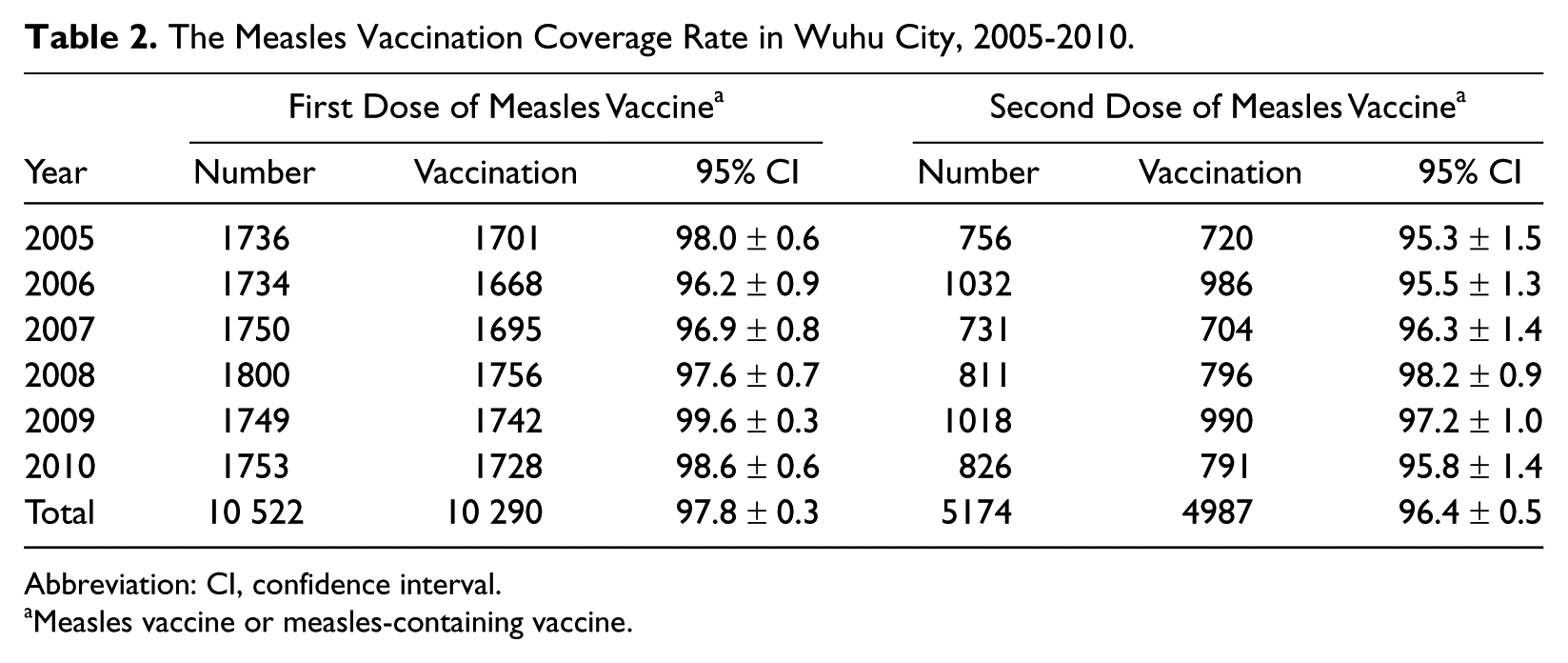
Abbreviation: CI, confidence interval.
Measles vaccine or measles-containing vaccine.
Discussion
Sustaining high measles vaccine coverage provided a scenario of prospective elimination of the disease in the past decades. However, the incidence of the disease has increased since 2005. In Wuhu city, there was a new outbreak observed from 2005 to 2010, and the reported cases were more than 10 times the average annual number in the 1996-2004 period. 5 If we take into account the fact that certain unavoidable underdiagnosis and underreporting may still exist, the actual epidemic situation may be worse. The same increase in trend was also observed in the country as a whole and in other countries.2,6-9
It should be noted that the recent outbreak was accompanied by new age distribution characteristics. Infants younger than 1 year and adults (≥22-30 years old) were the new susceptible population, which was not observed before. Our results are consistent with those of other studies and revealed similar age distribution characteristics.10,11
In the prevaccination era, measles was a disease with the highest age-specific incidence among children aged 2 to 5 years; it was rarely found in infants younger than 1 year. Peña-Rey et al 12 suggested that use of the measles vaccine has changed the age distribution of measles cases, and different vaccination histories and coverage may cause different age-related susceptibility patterns. Our observations also support this hypothesis.
In the early stage when the measles vaccine was introduced, the susceptible subgroup was protected by the vaccine; meanwhile, most adults were immunized by natural infection. With consistent use of the vaccine, the incidence decreased gradually leading to a vaccine “honeymoon” period. During this period, countries maintained a low incidence with high measles vaccine coverage, which led to a lower chance of getting enhanced immunity from the natural infection. Absence of complete measles vaccination and not being able to obtain enhanced immunity from the natural infection combined with waning of immunity from the vaccination may have contributed to the increase in young adults’ susceptibility. There was evidence that there was low serum-positive rate of measles antibodies in young adults. 13 In addition, more and more mothers got immunity protection from the vaccine instead of through natural infection. Because the immunity protection antibody titer attenuates faster than that for natural infection, these mothers gave their offspring less and limited passive protection against the measles virus in their children’s first year of life than mothers in earlier periods.14-16 All these might explain why our data showed the outbreak peak to be at age <1 year.
In China, recommendations have been made for the first dose of measles vaccine to be given at 8 to 12 months of age. The age-specific incidence in this age group was the highest. It may be a result of the waning of antibody acquired from mothers and also because the proportion of infants vaccinated in time at 8 months was not high enough. In Zhejiang province of China, the age-appropriate immunization coverage rates for the first dose of the vaccine was only 64.5%, whereas the immunization coverage rates of the Expanded Programme on Immunization (EPI) vaccine were all greater than 90%. 17 Moreover, a high floating population made some children “hard to reach” for age-appropriate immunization. 18
Low measles vaccine coverage was putatively considered to be the main cause of the increased measles cases in China. 6 However, we should not ignore the fact that a large proportion of the data regarding vaccination status of patients was collected by patient or parent recall, so the recall bias was unavoidable. In addition, the vaccination coverage threshold required for measles elimination was determined based on the total population, not on patients. The shift in age distribution of measles told us that some age groups of adults and young infants were also susceptible to measles. Therefore, the data on the measles vaccine coverage rate based on the children cannot represent the general population’s immunity against measles in contrast to the situation earlier.
In the context of the current measles situation, in addition to maintaining optimum routine vaccination coverage, it is necessary to use additional vaccination on susceptible young adults and strictly follow the first-dose schedule at 8 months for infants. These are the cornerstones of the measles elimination plan for China.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was partially supported by the Science Foundation of Dongguan (201010815214) and Guangdong Medical College PhD Grant (XB0814).