
Abstract
The objective of this study was to investigate whether the relationships of appendicular muscle mass (ASM) with insulin resistance (IR) and metabolic syndrome (MS) vary by gender or obesity. Data of 10 146 normal-weight and obese men and women aged 19 to 93 years from the Korea National Health and Nutrition Examination Survey in 2009 and 2010 were analyzed. In normal-weight men and women, unadjusted odds ratio (OR) of being MS and IR significantly increased with lower ASM/wt. After adjusting for lifestyle factors, these ORs were still significant in normal-weight men but not in women. After controlling for other covariates, lower ASM/wt was related to higher risk for IR but not to MS in obese men. In obese women, relationship of lower ASM/wt with higher risk for MS disappeared after adjusting for covariates. Association between skeletal muscle mass and cardiometabolic abnormalities is dependent on gender and obesity in Korean adults.
Introduction
There is growing awareness about the association of skeletal muscle mass with cardiovascular disease and risk factors.1,2 Although inverse association of muscle mass with metabolic syndrome (MS) or insulin resistance (IR) has been reported,1,3 influence of gender and obesity on these associations has not been assessed. Given the gender, ethnic, and weight-related differences in skeletal muscle mass,4,5 gender and body size phenotypes (normal weight and obese) might influence association between muscle mass and cardiometabolic abnormalities. However, little is known about their impacts on relationship of skeletal muscle mass with cardiometabolic abnormalities especially in Asians such as Korean who might be at higher cardiometabolic risk due to a lower muscle mass compared with other races. 6
A higher risk of having MS is associated with higher body mass index (BMI), older age, and lifestyle factors including low physical activity and smoking.7,8 Therefore, assessment of the impact of muscle mass on cardiometabolic abnormalities may need simultaneous consideration of these covariates.
The objective of this study was to examine the impact of appendicular skeletal muscle (ASM) mass on the risk of having the MS and IR after controlled for other covariates including lifestyle factors in normal-weight and obese men and women using a nationally representative sample of Korean adults.
Methods
Study Subjects
The subjects and data were obtained from the fourth and fifth Korea National Health and Nutrition Examination Surveys (KNHANES IV-3 and V-1), a cross-sectional and nationally representative survey with a stratified, multistage, probability sampling design conducted by the Korea Centers for Disease Control and Prevention in 2009 and 2010. The KNHANES consisted of the Health Interview Survey, Health Examination, and Nutrition Survey. The present study used data from anthropometric measurement, blood test, blood pressure, body composition, and various health and lifestyle questions including self-reported health status, smoking, drinking alcohol, physical activity. Details of the KNHANES design, procedures, and participants have been published elsewhere.9-11 In brief, the fourth (2007-2009) and fifth (2010-2012) KNHANES were conducted annually using a rolling sampling design. The target population of the survey was noninstitutionalized civilians older than 1 year in South Korea. Sampling units were defined based on geographic area, gender, and age group using the household registries from the National Census Registry. A total of 12 722 individuals from 3975 households in 200 national districts in 2009 and 10 938 people from 3840 households in 192 national districts in 2010 were randomly sampled. A total of 10 078 (79.2% of the target population) in 2009 and 8473 (77.5% of the target population) in 2010 participated in the Health Interview Survey and the Health Examination, respectively. The Health Interview Survey was conducted by trained interviewers, and the Health Examination was performed in mobile medical clinics.
The present study included 4630 men and 5516 women, aged 19 to 93 years with complete data with anthropometric measurement, body composition, blood test, and health behavior questionnaire. The subjects who had mental and physical disability, cancer, stroke, ischemic heart disease, hepatic disease, renal disease, or thyroid disease, were underweight (BMI < 18.5), or fasted less than 8 hours prior to blood sampling were excluded. All participants in this survey signed an informed consent form.
Measurements
Based on their BMI (kg/m2), subjects were classified as being normal weight (18.5 ≤ BMI < 25) or obese (BMI ≥ 25). ASM mass was measured by dual-energy X-ray absorptiometry (Hologic, Bedford, MA). ASM in kilogram was calculated as the sum of lean soft tissue in both right and left arms and legs and normalized for body weight (ASM/wt (%) = ASM/weight × 100). The ASM/wt values were divided into quartiles as previously described. 3 Appendicular lean soft tissue is known to be well correlated with total body skeletal muscle mass measured by whole body magnetic resonance imaging.12,13
Cardiometabolic abnormalities were determined using MS criteria and insulin resistance. Insulin resistance was determined using the homeostasis model assessment of insulin resistance (HOMA-IR = fasting glucose [mmol/L] × fasting insulin [µU/mL]/22.5) and defined as a HOMA-IR value >75th percentile (2.79 in present study). 14
For a metabolic syndrome definition, the National Cholesterol Education Program (NCEP) Adult Treatment Panel (ATP) III criteria were used 15 : (a) elevated blood pressure defined as systolic or diastolic blood pressure ≥130 and 85 mm Hg or on antihypertensive drug treatment; (b) fasting plasma glucose ≥100 mg/dL or on antidiabetic drug treatment; (c) triglyceride concentration ≥150 mg/dL; (d) high-density lipoprotein (HDL) cholesterol concentration <40 mg/dL in men and <50 mg/dL in women; and (e) central obesity defined by a waist circumference ≥90 cm in men and ≥80 cm in women for Asians. Subjects who had at least 3 of the 5 criteria were classified as having a metabolic syndrome.
Confounding variables such as age, BMI, menopausal status, and lifestyle factors, which were previously reported as risk factors for MS, were considered.7,8 Lifestyle factors included physical activity (physically active [regular moderate-intensity physical activity more than 30 minutes 5 times per week or vigorous physical activity more than 20 minutes 3 times per week] or not), smoking (current smoker, former smoker [≥100 cigarette in lifetime] or nonsmoker), and alcohol drinking (drinker [≥1 drink per month in the past 12 months] or nondrinker). Menopause status and use of hormone replacement therapy were assessed in women.
Statistical Analysis
Significant differences in prevalence of cardiometabolic abnormalities (MS, 5 components of the MS, and IR) among sex-specific quartiles of ASM/wt in normal-weight and obese men and women were determined using χ2 test. Binary logistic regression analyses were used to examine the associations of having MS, 5 components of the MS, and IR with quartiles of ASM/wt in an unadjusted model and in a model including potential covariates. Dependent variable was coded as 1 representing having each component of cardiometabolic abnormalities and 0 representing an absence of outcome. Unadjusted odds ratio (OR) of each outcome for quartiles of ASM/wt (Q4 [≥75th percentile] as a reference: OR = 1) was estimated. If OR is greater than 1, it indicates that, relative to Q4, the odds of the outcome occurring increase. In addition, adjusted ORs of having cardiometabolic abnormalities with 95% confidence interval (CI) for quartiles of ASM/wt were presented with adjustment for age, BMI, alcohol drinking, smoking, physical activity, and HOMA-IR in men and with further adjustment for menopause status and hormone replacement therapy in women. The level of significance was set at P < .05. Data were analyzed using SPSS version 13.0 (2004, IBM SPSS, Chicago, IL).
Results
The overall prevalence of all cardiometabolic abnormalities except central obesity and low HDL was greater in men than in women (all P < .01) with the greater prevalence in obese group than in normal-weight group in both men and women (all P < .001). When the prevalence of cardiometabolic abnormalities was presented by quartiles of ASM/wt (Tables 1 and 2), prevalence of MS, elevated blood pressure (BP), central obesity, hyperglycemia, high triglycerides (TG), low HDL cholesterol, and IR all significantly decreased with increments in quartiles of ASM/wt in normal-weight men and women. In obese men, prevalence of all cardiometabolic abnormalities except low HDL also decreased as quartiles of ASM/wt increased. However, in obese women, only prevalence of MS and central obesity decreased with higher ASM/wt.
Prevalence and Adjusted Odds Ratios of Metabolic Abnormalities According to Quartiles of Appendicular Skeletal Muscle Mass as Percentage of Body Weight in Normal-Weight and Obese Men.
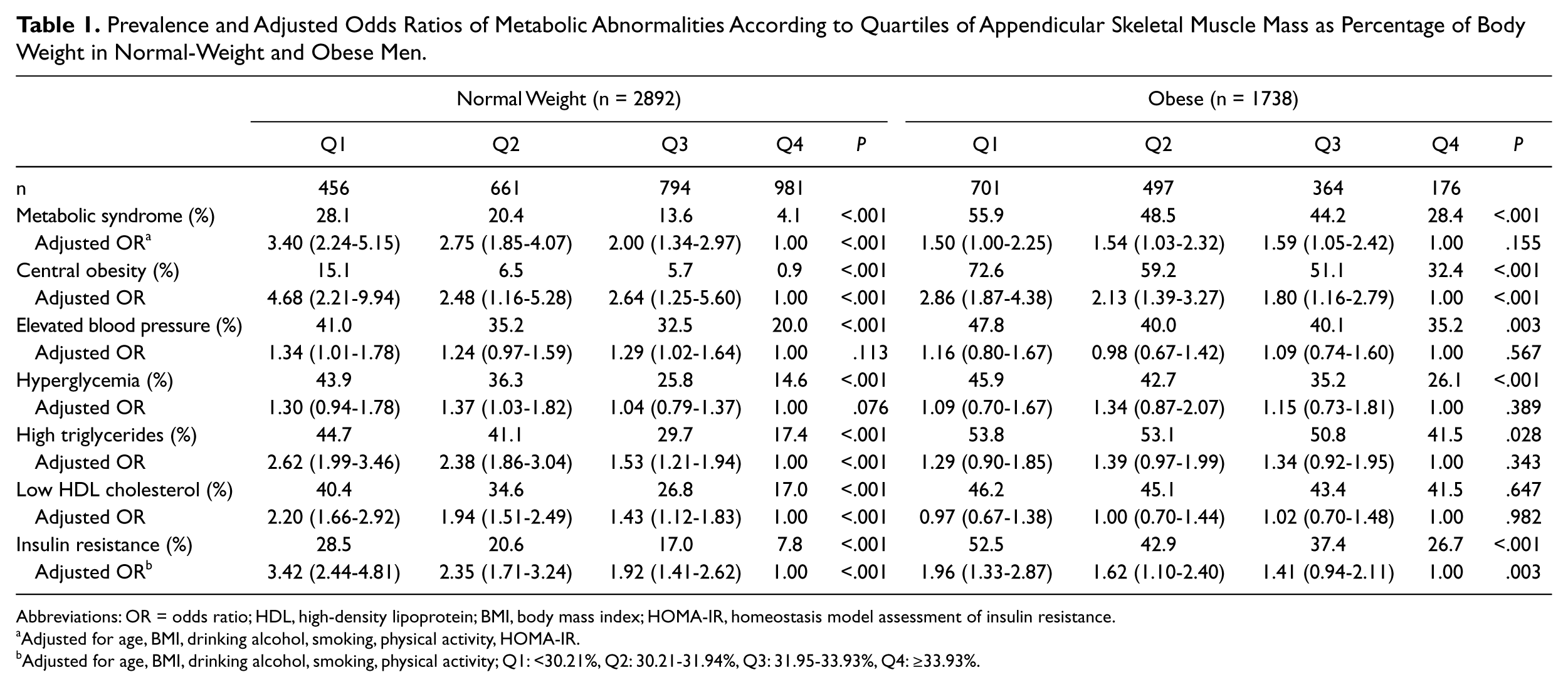
Abbreviations: OR = odds ratio; HDL, high-density lipoprotein; BMI, body mass index; HOMA-IR, homeostasis model assessment of insulin resistance.
Adjusted for age, BMI, drinking alcohol, smoking, physical activity, HOMA-IR.
Adjusted for age, BMI, drinking alcohol, smoking, physical activity; Q1: <30.21%, Q2: 30.21-31.94%, Q3: 31.95-33.93%, Q4: ≥33.93%.
Prevalence and Adjusted Odds Ratios of Metabolic Abnormalities by Quartiles of Appendicular Lean Mass as Percentage of Body Weight in Normal-Weight and Obese Women.
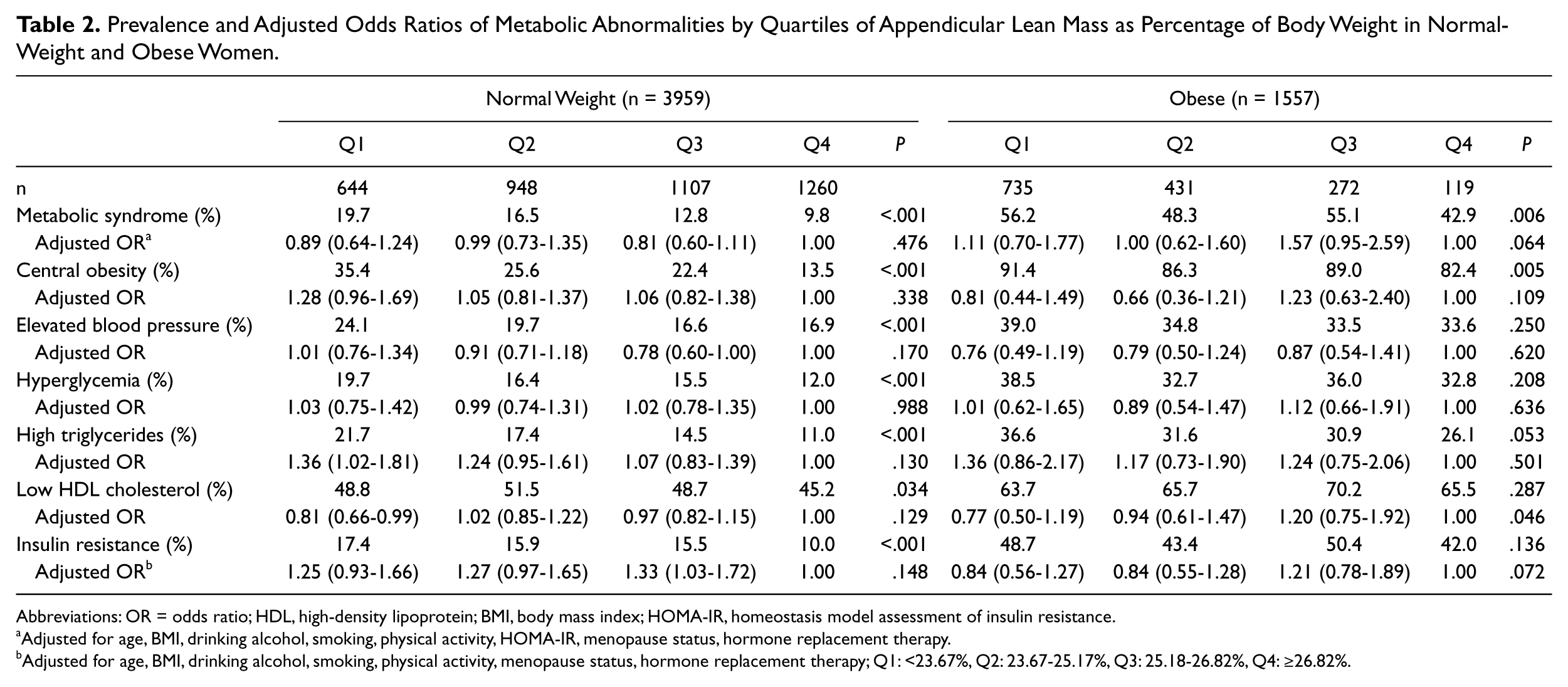
Abbreviations: OR = odds ratio; HDL, high-density lipoprotein; BMI, body mass index; HOMA-IR, homeostasis model assessment of insulin resistance.
Adjusted for age, BMI, drinking alcohol, smoking, physical activity, HOMA-IR, menopause status, hormone replacement therapy.
Adjusted for age, BMI, drinking alcohol, smoking, physical activity, menopause status, hormone replacement therapy; Q1: <23.67%, Q2: 23.67-25.17%, Q3: 25.18-26.82%, Q4: ≥26.82%.
In normal-weight men and women, unadjusted ORs of having cardiometabolic abnormalities significantly increased with lower ASM/wt (all P for trend < .05). After adjusting for covariates, ORs of having MS, central obesity, high TG, low HDL, and IR were still significant in normal-weight men (all P for trend < .001) but all ORs were nonsignificant in normal-weight women (Tables 1 and 2). In normal-weight men, the ORs for having MS, central obesity, high TG, and low HDL in the lowest quartile of ASM/wt (Q1: <30.21%) compared with the highest quartile (Q4: ≥33.93%) were 3.40 (95% CI = 2.24-5.15; P < .001), 4.68 (95% CI = 2.21-9.94; P < .001), 2.62 (95% CI = 1.99-3.46; P < .001), and 2.20 (95% CI = 1.66-2.92; P < .001), respectively, after adjusting for age, BMI, drinking alcohol, smoking, physical activity, HOMA-IR (Table 1). In normal-weight men, the OR for having IR in Q1 was 3.42 (95% CI = 2.44-4.81; P < .001) after adjusting for age, BMI, drinking alcohol, smoking, and physical activity.
In obese men, unadjusted ORs of having cardiometabolic abnormalities except low HDL significantly increased with lower ASM/wt (all P for trend < .05). However, after adjusting for covariates, only central obesity and IR remained significant in obese men. In obese men the ORs (95% CI) in each ASM/wt quartile were 2.86 (1.87-4.38), 2.13 (1.39-3.27), 1.80 (1.16-2.79), and 1.00 (P for trend < .001) for having central obesity after adjusting for age, BMI, drinking alcohol, smoking, physical activity, and HOMA-IR and 1.96 (1.33-2.87), 1.62 (1.10-2.40), 1.41 (0.94-2.11), and 1.00 (P for trend = .003) for being IR after adjusting for age, BMI, drinking alcohol, smoking, and physical activity (Table 1). In obese women, unadjusted ORs of having MS and central obesity were significant (P for trend = .007 and .006, respectively) but the significance disappeared after adjusting for age, BMI, drinking alcohol, smoking, physical activity, HOMA-IR, menopause status, and hormone replacement therapy (Table 2).
Discussion
The primary finding of the present study was that association between skeletal muscle mass and cardiometabolic abnormalities were dependent on gender in normal-weight and obese Korean adults. Findings indicate that lower ASM was the significantly independent factor associated with increased risk of the MS and IR after controlling for covariates including lifestyle factors in normal-weight men but not in normal-weight women. This finding is consistent with results from previous studies showing that muscle mass was inversely related to MS in older Australian men without information on obesity and directly with insulin sensitivity in young healthy normal-weight Indian men with small sample size.1,16
In the present study, lifestyle factors and BMI rather than ASM were significantly associated with risk for IR in normal-weight and obese women. Moreover, older age, postmenopausal status (normal-weight group only), and higher BMI and HOMA-IR rather than lower ASM were significantly associated with risk for MS in women. In obese men, lower ASM was related to higher risk for IR but not to MS after controlled for other covariates (significant covariates for MS in multivariate logistic regression model: older age, being current smoker, higher BMI, and higher HOMA-IR). A previous study reported that total body skeletal muscle mass was not associated with insulin sensitivity in overweight and obese men and women, suggesting that other factors might be more important than muscle mass. 17 This result is consistent with the present finding in women but not in men.
One recent study reported that the total muscle mass (estimated by bioelectrical impedance) expressed as percentage of body weight and divided into quartiles was inversely associated with IR and prevalence of diabetes after adjusting for age, ethnicity, gender, and general and central obesity. 3 These findings suggest that inverse relationship of muscle mass with IR exists regardless of gender, contradictory to present findings. This might be due to measurement differences, which could have resulted from different methods used for estimating muscle mass or ethnic differences. Although the previous study mentioned above controlled for race (non-Hispanic white, non-Hispanic black, Mexican-American, and other), 3 there was little information about Asian ethnicity in the study. Furthermore, ethnic variation among Asian in fat and lean body mass is known to be related with IR. 4 Therefore, it is possible that one of the reasons for lack of the relationship between muscle mass and IR in women could be due to ethnic difference of Korean population.
One possibility of gender differences in the present findings is that gender differences in muscle mass or other muscle pathophysiology could confound an association of muscle mass with MS or IR. Women are known to have less absolute and relative muscle mass than men. 5 Muscle morphology and metabolism such as muscle fiber type, muscle capillary density, or imbalance between glycolytic and oxidative enzyme capacities are known to be associated with IR and muscle glucose metabolism.18-20
Although inverse association between skeletal muscle mass and MS or IR was previously reported,1,3 whether gender and obesity influence association between muscle mass, MS, and IR or not has not been investigated to the best of my knowledge. Therefore, the present study is the first study demonstrating the significance of gender difference in association between skeletal muscle mass and cardiometabolic abnormalities in both normal-weight and obese adults using a nationally representative sample.
One noteworthy study limitation is that the present study used a cross-sectional design, which has the limitation to detect causal relationships. Therefore, causal inferences between ASM and cardiometabolic abnormalities cannot be made. Also, it is worthy of note that the present study used data from health status and behavior surveys based on self-reported questionnaires to exclude subjects with chronic diseases that might physiologically affect muscle mass and categorize lifestyle factors. Nevertheless, it is still possible that there might be misclassification or asymptomatic subjects who were never diagnosed.
In conclusion, the results of the present study indicate that lower muscle mass is an independent risk factor for MS and IR in normal-weight men but not in women. Interestingly, the impact of lower muscle mass on MS disappears after controlled for IR and lifestyle factors in obese men. These findings suggest that the appropriate interventions designed to increase skeletal muscle mass may be required to prevent cardiometabolic abnormalities in normal-weight Korean men.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.