
Abstract
Objective. To develop a better understanding of perceived barriers to and ideas for weight loss and maintenance among Malay homemakers in Singapore. Methods. Interventions for weight management were reviewed, and 5 focus groups were conducted among overweight and obese Malay homemakers (n = 24) to explore barriers to and concepts and ideas pertaining to weight loss and maintenance. Results. Barriers identified included the lack of time, finances, and motivation. Ideas that were most appealing included free health screening, workshops on how best to manage children and family, regular fun group activities, monetary incentives for participation in activities for healthy living, and flexible part-time jobs. Conclusion. The focus groups provided useful insights pointing toward possible interventions that could appeal to Malay homemakers in Singapore. The most appealing approaches were those that were time flexible and had the least financial burden or had a financial benefit.
Keywords
Introduction
The rising prevalence of overweight and obesity 1 and the economic costs associated with obesity 2 are a concern worldwide, especially for high-risk groups. 3 In the Asia-Pacific region, women, compared with men, and Malays, both in Singapore and elsewhere, compared with other ethnic groups, are at a greater risk for overweight and obesity.4,5 A study from Singapore reported that two-thirds of Malay women were overweight (body mass index, BMI ≥ 25 kg/m2), with an even higher prevalence among those of lower socioeconomic status. 6 The prevalence of diabetes and levels of systolic blood pressure as well as total and low-density lipoprotein cholesterol were also found to be higher among Malay women than men. 7 Among Malay women, homemakers may be at a higher risk for overweight and obesity. In the study by Shariff and Khor 8 in selected rural communities in Malaysia, they observed that food insecure women, mainly homemakers with more children, tended to be overweight or obese. Studies from elsewhere also report that female homemakers had less total physical activity than women who were unskilled or professional workers.9,10 Thus, Malay women homemakers are an important demographic group to reach with weight management interventions.
An understanding of the key behaviors associated with obesity—namely, the extent of excessive dietary intake and reduced physical activity—is central for the development and success of any behavioral interventions in a targeted population group. A study found that Malay women of lower socioeconomic status expressed less concern about their weight. 6 The Singapore National Nutrition Survey 2004 documented a high prevalence of unhealthy dietary practices among Malays. 11 However, the survey also documented that nearly 40% of Malays had dieted to lose weight and that half were doing so frequently or continually. 11 On the other hand, the prevalence of regular exercise and inactivity was higher and similar, respectively, among the Malays relative to the Chinese. 12 Organizations such as the Social Enterprise Network Singapore Pte Ltd (SENSE) and Persatuan Pemudi Islam Singapura (PPIS) are also active in the Malay community in Singapore and organize activities such as aerobics classes and cooking courses for Malay women of any age and socioeconomic status to better their health. Thus, although these studies and national surveys suggest that unhealthy practices associated with weight gain or obesity are common among Malays in Singapore, the findings are somewhat inconsistent and do not provide deeper insights into the perceptions Malays have about dietary intake and physical activity. Although 1 study suggested that limited resources, limited time to engage in physical activity, and consumption of cheaper but unhealthy energy-dense foods rich in fat were contributors toward the high obesity prevalence among Malay women, these suggestions were conjectures based on studies from other countries and not based on the primary data. 6
Because very little is known about attitudes and knowledge related to healthy weight behaviors among Malay homemakers, an in-depth qualitative study was deemed necessary before developing any interventions for this population subgroup.
The focus group is a qualitative research technique for eliciting information from specific population subgroups 13 and has been used to explore the barriers to and motivators or cues for healthy eating, physical activity, and weight loss among African Americans14-17 and other minority groups.18,19 Furthermore, focus groups, unlike individual interviews, provide an added dimension—namely, insight into group members’ interactions. 20 This should help design interventions that are more likely to be acceptable, sustainable, and effective in the targeted group.
The objective of this study was to develop a better understanding of perceived barriers to and ideas for weight loss and maintenance among Malay homemakers in Singapore.
Method
The study had ethics approval from SingHealth Institutional Review Board (IRB #90/2006) and was exempted from IRB review by the Duke University Health System Institutional Review Board (Pro00027123).
A team of health care professionals, comprising 2 endocrinologists, an obesity clinical coordinator, an exercise physiologist, and a staff involved in marketing communications for health care services, had several meetings to consolidate possible hypotheses and interventions based on their clinical experience as well as the lifestyle strategies from the Diabetes Prevention Program 21 (phase 1). The Diabetes Prevention Program was chosen because it included a range of strategies aimed at diet, exercise, and behavioral modification to effectively help reduce weight and the risk of developing diabetes. 21 These hypotheses and intervention ideas formed the basis for designing the discussion coverage for the focus groups in phase 2 and facilitate the analytical induction approach to provide an initial logical framework to link lifestyle, motivations, and possible interventions. Figure 1 illustrates the details of each phase of this study.
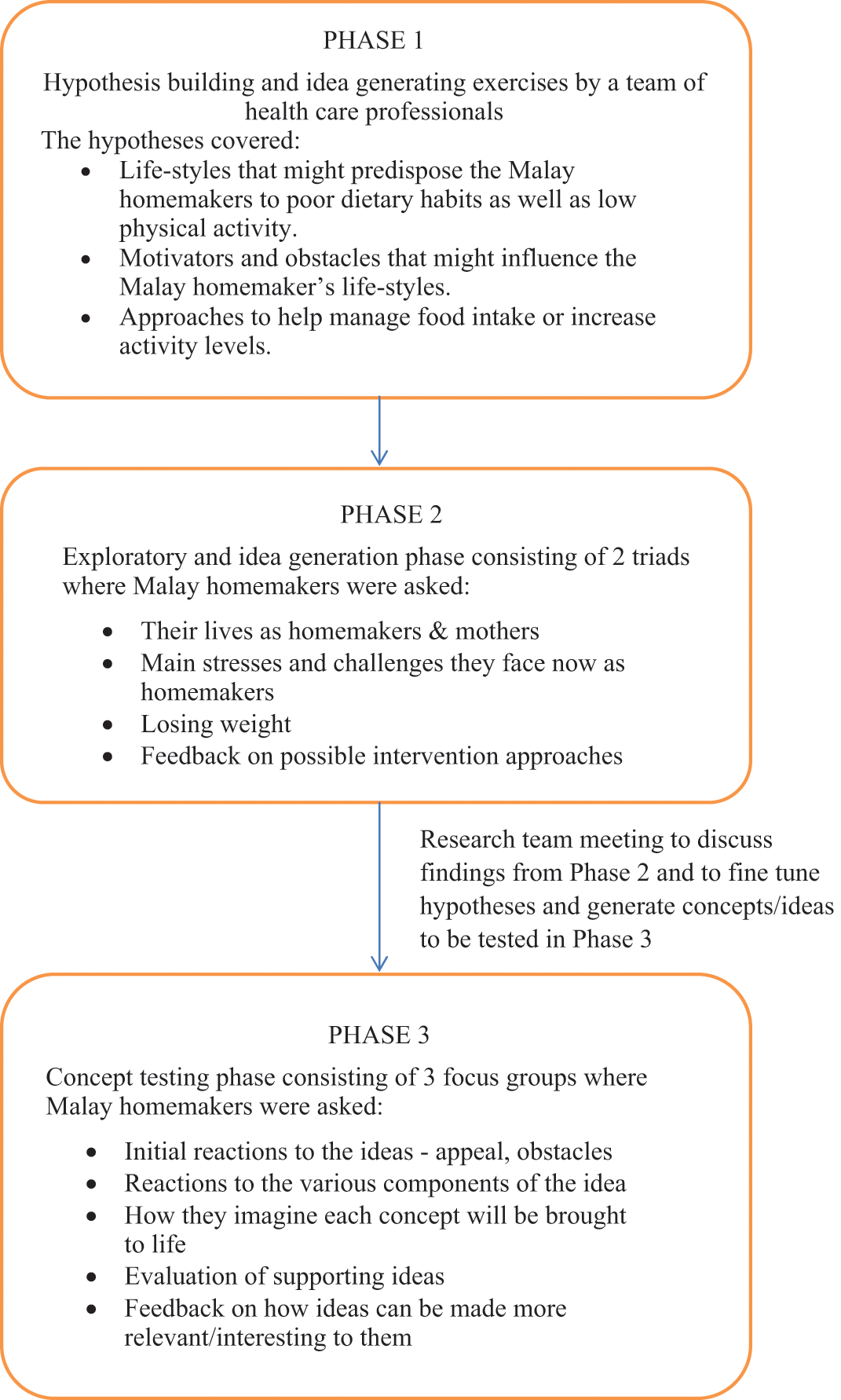
Flow chart illustrating the different phases of the study.
Focus Groups
Five focus groups were conducted between October 2007 and January 2008 by 1 independent facilitator (a psychologist with extensive focus group experience) from Acorn Marketing & Research Consultants (Acorn). All focus groups were conducted over a meal in a casual environment and were observed by the team of health care professionals from behind a 1-way mirror. The sessions were conducted in English and video recorded, and an assistant moderator took notes during the sessions. Each session lasted 1.5 hours and included 3 to 6 participants. The facilitator introduced himself and gave a brief overview of the topic of discussion, objective of the research, and ground rules for the session. Written informed consent was obtained for the recording from each participant. Each participant received a monetary incentive (150 Singapore dollars) for their time. After each focus group session, an hour-long meeting was held that included the facilitator and the health care professionals to discuss the key points from the session.
The first 2 focus groups, known as triads (each had 3 participants), were “exploratory” or “idea generation” focus groups (phase 2), conducted among 6 overweight Malay homemakers in their late 30s who were friends with each other for at least 5 years. Triads are a form of ethnographic research where participants were placed in a familiar social context to facilitate discussion of sensitive topics 22 —in this case, weight issues. Thus, the decision to recruit friends for this phase of the current study was intentional, so that the overweight respondents would be less self-conscious talking about eating and physical activity. 23 The findings from these triad groups were discussed to revise the initial hypotheses, if required, to aid in the development of a list of possible interventions for weight loss and maintenance, which were subsequently tested in the focus groups in phase 3.
Phase 3 consisted of 6 participants in each of the 3 “concept testing” focus groups. The participants in each of the focus group were of similar age, life stage and BMI, but they were not friends, thus providing a wider spectrum of responses. These women were recruited by a network of recruiters from Acorn who approached strangers and business and social contacts to identify individuals who met the recruitment criteria. Potential candidates were further screened via phone interviews to group them into the focus groups to ensure diversity (not all living in the same neighborhoods, nor all having similar numbers of children).
Data Analysis
The entire team, including the researchers from Acorn, were present throughout all focus groups, watching through a 1-way mirror to take notes. All focus group sessions were also audio- and videotaped as well as transcribed verbatim. The focus group interviews were listened to in their entirety to determine common themes, and their connection to the transcripts was established. 24 In the second stage of coding, the analytical induction approach was used to develop a link between lifestyle, motivations, and possible interventions associated with weight management. 25
Results
Participants
The Malay homemakers (n = 24) were 36 to 38 years old, with low- to middle-levels of family income, having 1 to 4 children, a BMI above 27.5 kg/m2, and a family history of diabetes. These homemakers lived in 3- to 5-room high-rise public housing (flats).
Phase 1: Current Evidence
Based on their own experience, the team of health care professionals felt that Malay homemakers often have irregular and imbalanced meals because of lack of personal free time and the prioritization of their family’s needs above their own. We generated 9 possible intervention ideas, thought to be appealing to Malay homemakers, for discussion in the phase 2 focus groups.
Phase 2: Exploratory
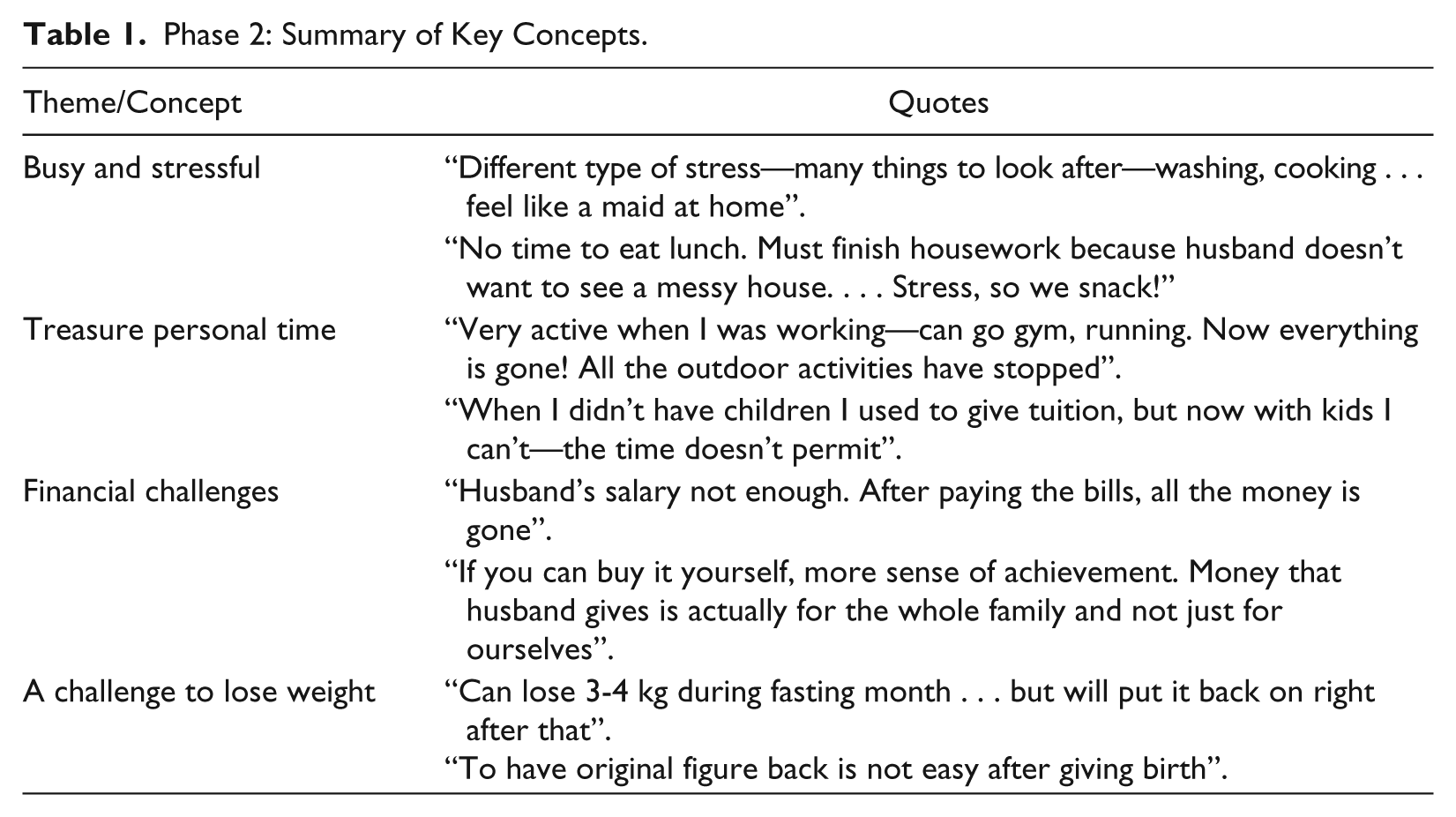
The role of a homemaker was perceived to be physically demanding and hectic. Table 1 summarizes the key concepts from phase 2. The women managed multiple daily projects—their children, cleaning the house, and cooking—which were time consuming and possibly tedious. They wanted to be seen as busy because this meant that they “sacrificed” their time for their family, and this was rewarding and something to be proud of, similar to that of their working peers who often emphasized that their lives were stressful and busy and therefore important.
You have to wake up before the children and get them ready for school, send them to school and back. In between, run errands. Very busy . . . sometimes I buy newspapers but even forget to read them.
Phase 2: Summary of Key Concepts.
However, they also aspired to be less active by trying to find ways to spend less time and effort on house work by using automation and training their children to help out. Thus, it was against their aspirations to do more housework as part of increasing physical activity.
Blender! Used to pound chilli, now I blend everything. Don’t want to spend whole day on housework . . . want some time to myself.
The primary challenge and stress was that of managing family finances. Besides being successful in household management, they aspired to have some personal time to themselves as well as to be financially independent.
If you can buy it yourself, more sense of achievement. Money that husband gives is actually for the whole family and not just for us.
Although being a good cook was seen as important, earning their own money was more important because that would contribute to their family finances and provide them with personal spending power.
When we are working, we can buy what we want, but now we don’t get to.
They often replaced their main meals with snacks because of their busy schedule of housework and care of children. This blurred the line between a meal (considered valid and necessary) and a snack (considered unnecessary). On the issue of dieting, the participants said they were already doing that during the fasting month and attempted to control their food intake—they “survived” through many rounds of social eating. However, they were still aware that they were overweight and expressed displeasure with this fact because they all desired to look as good as the models in weight loss advertisements.
We skip so many meals in the day, but still look like this—square!
Gyms, perceived as premium tier services similar to Botox treatment, were not appealing. They rather preferred physical activity to be part of a social activity. They admitted that they had been more active in the past and presently were keen on social gatherings regardless of whether it included physical activity or not. Their busy schedules allowed them only 2 to 3 hours of free time each day, during which they could be involved in physical activity or work. However, they were not in favor of weight loss centers or “slimming pills” because they knew of friends or relatives who had spent thousands of dollars with little results and put on all the lost weight after ceasing these interventions. They expressed a lack for motivation and self-discipline to sustain lifestyle modification to lose weight.
If we could control we wouldn’t look like this!
They were also more self-conscious about attending a weight loss program even in the hospital setting because of past failures and the stigma of making it being seen as a medical problem. The causes of weight gain were perceived by all the participants to be a result of their role as homemakers, having children, and growing older—all part of life’s journey.
Not perfect, but it’s okay. All our friends are also like this.
In summary, the barriers to healthy lifestyle for weight management were lack of time and money. Possible cues for Malay homemakers to take action were monetary incentives, interventions that were flexible, and activities that were set in their social context and possibly involving their children as a channel to inculcate healthy habits.
Perception of the 9 Ideas From Phase 1
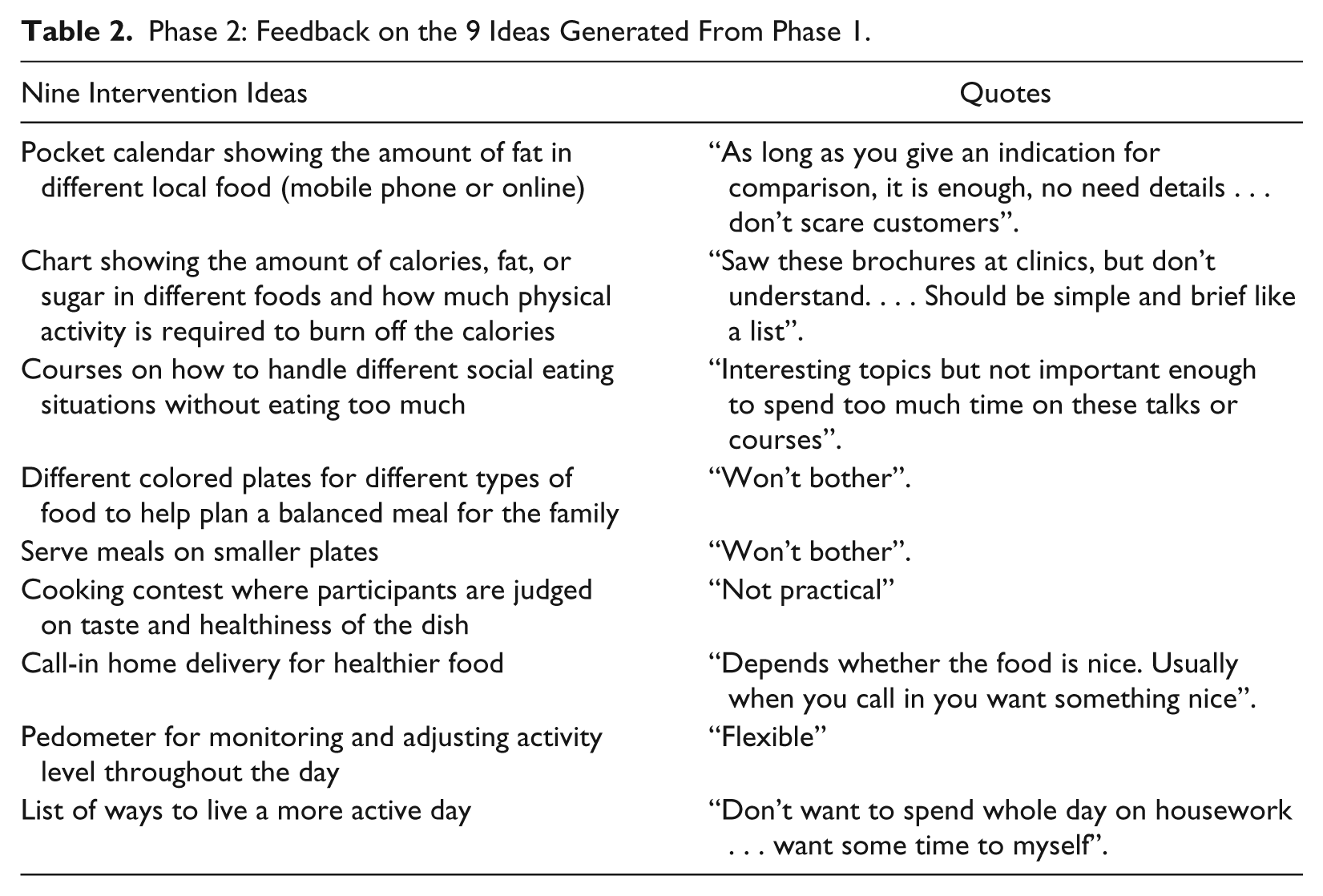
The 9 intervention ideas were written on big cards and presented to the women who chose which interventions appealed or did not appeal to them and provided the reasons why. The Malay homemakers found only 2 of the intervention ideas that were presented to be interesting (Table 2): a pocket calendar depicting the fat content of local dishes (“is informative”) and the use of pedometers to monitor activity level (“flexible”).
Phase 2: Feedback on the 9 Ideas Generated From Phase 1.
Phase 3: Concept Testing—Perspectives on 16 Ideas From Phase 2
The perspectives of the Malay women on life, especially as homemakers, and on the challenges and barriers to weight control were reviewed, and 14 new ideas were generated by the team of health care professionals after evaluating the responses from phase 2. These 14 ideas together with the 2 intervention ideas that the homemakers found interesting, revolved around the provision of monetary incentives to motivate, providing monitoring, having programs that aimed at their children’s health, and having a social context attached to the activities (Figure 2).
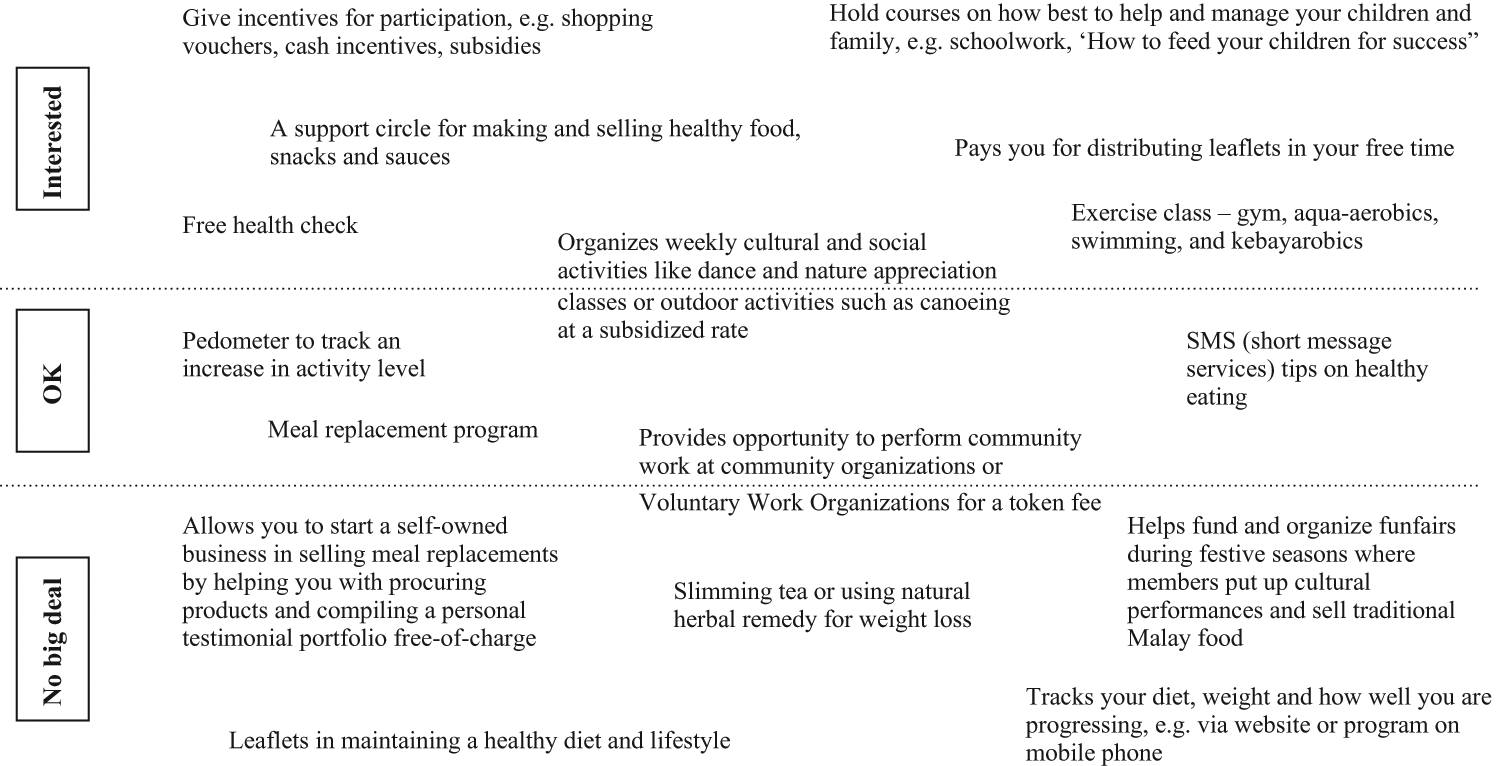
Malay homemakers’ perceptions of the 16 intervention ideas developed in phase 2. These were classified into 3 sections: “Interested,” “Ok” or neutral, and “No big deal” or not interested at all.
The Malay homemakers felt that the meal replacements would be effective but were concerned about sustainability and were only willing to use these once a day.
Expensive . . . also need to eat with family especially dinner.
However, they expressed interest in any activity that did not impose any financial burden or had a financial benefit, such as free health screenings, cash incentives for participation, and part-time job opportunities.
Went for courses, each lasting at least 2 to 3 days . . . but I was still not given a job.
Although they were relatively inactive or sedentary, they did not want to be singled out as needing exercise but preferred physical activity embedded in activities with other explicit purposes, such as cultural or social activities, rather than specifically going to a gym.
Have programs which allow me to choose not to do too little and not to do too much—prefer the middle zone of activities to “stay within the norm”—not to be seen as weak willed or too “extreme”.
The idea of doing things together with minimal level of commitment in a social context was more important than the exact activity.
If not it will come across as community centre—organizes a lot of different activities and you attend the ones which interest you . . . which you never get around to it.
Because time was perceived as very precious, they were receptive to household appliances that could save time in household chores or cooking time; thus, incentives such as shopping vouchers to purchase such appliances were attractive. Having a person to mind the children while they participated in activities was appealing as well:
Can bring kids along? Can’t go if there is no baby sitter.
The rest of the ideas, such as setting up a self-owned business to sell meal replacements, were not particularly appealing because they thought that it would be difficult to sustain in the long term.
Discussion
This is the first qualitative study to identify barriers to change and cues to action for healthy weight among Malay homemakers in Singapore. The main issue with this demographic group was that they perceived overweight as being common among homemakers, and their aim was to maintain their weight. Although organizations such as SENSE do offer physical activity programs for Malay women, the likely barriers toward participation include location, children, timing, and cost. Intervention ideas that appealed to Malay homemakers were those that focused on their role as a mother and a finance manager, those requiring the least commitment, and those with monetary benefits. These included free health screening, workshops on how best to manage children and family, and regular group activities that had a financial benefit. Gym membership was not appealing, likely because of its cost and their perception that it, like Botox treatment, was targeted toward working professionals rather than homemakers.
It would be cost-effective to engage existing Malay organizations to best address the above problem of sustaining an activity by providing resources to mind the children and having partnerships with larger organizations to provide flexible working hours. A study that administered a survey in Malaysia echoed the same sentiments as women who left the workforce after having children were willing to reenter the job markets if work conditions were flexible. 26 A healthy work-life balance would not only benefit the Malay homemakers, but it would also provide a boost to the workforce.
The women said that promotion of good health or weight loss without “medicalizing” or showcasing the seriousness of the problem would appeal to them because they wanted to be treated as normal rather than being stigmatized. Hospital-based weight management programs are unlikely to appeal to them; thus, any program that intends to help them maintain a healthy weight should be held at the community level. They also preferred more frequent monitoring or supervision in the community where they could participate together with their peers because they often lacked motivation and discipline.
The next step is to collaborate with existing organizations and put some of these ideas into action. It is also of interest to assess whether the issues facing Malay women in Malaysia are different from those facing Malay women in Singapore.
One of the limitations of this study was the insufficient funds to run more focus groups. Furthermore, it was challenging to get more women involved because many of them had family commitments, and to have a fixed day and time for them to come together made it all the more challenging.
Conclusion
The main issue identified by the Malay homemakers in these focus groups was not weight loss but healthy weight maintenance. The participants identified their main problems to be lack of self-discipline and motivation and would like regular supervision to stay on track. Monetary incentives and “freebies” were seen as significant motivators. Using their roles as mothers and finance managers might also be a good strategy for educating them about healthy lifestyle. Weight management programs might be effective among the Malay homemakers if they are conducted in groups in the community. Future research is required to implement and assess the effectiveness of interventions among Malay homemakers.
Footnotes
Acknowledgements
We would like to thank the Malay ladies who participated in the focus groups and Michelle Melang who helped proofread the manuscript.
Authors’ Note
We certify that no party having a direct interest in the results of the research supporting this article has or will confer a benefit on us or on any organization with which we are associated.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this study was provided by SingHealth Foundation SHF/FG241P/2005.