
Abstract
We sought to examine correlations between international backpackers’ alcohol consumption and sexual behaviors and determine the prevalence of Chlamydia trachomatis and Neisseria gonorrhoea in this population. A cross-sectional study design consisting of a convenience sample (N = 168) of non-treatment-seeking international backpackers visiting Brisbane, Australia was recruited. Participants were asked to self-complete a questionnaire on sexual behavior and to undertake a urine-based polymerase chain reaction test for C trachomatis and N gonorrhoea. Since arriving in Australia, 73.2% reported having had sex, with a median number of 2 different sex partners (range = 0-21). Most participants had consumed alcohol (53.7%) and used condoms (46.3%) the last time they had sex. In our sample, there was a 4.3% prevalence of C trachomatis and a 0% prevalence of N gonorrhoea. This study identified a variable pattern of risk among backpackers, with those spending longer periods in the country more likely to have sex with Australians.
Introduction
The international travelling environment provides the opportunity for the mixing of broad sexual networks and increased sexual activity.1,2 Within this context, the increased likelihood for acquisition of a sexually transmissible infection (STI), including HIV has been established.2-9 In a study of backpacker attendees at the Sydney Sexual Health Centre, 10 backpackers were significantly more likely than other clients to report a history of human papillomavirus (HPV; 14% vs 12%, P = .008), Chlamydia (13% vs 8%, P < .001), and pelvic inflammatory disease (0.8% vs 0.3%, P < .001). They were also more likely to present with Chlamydia (8% vs 5%, P < .001), and equally likely to present with HPV (16%). Although a number of studies on short-term young adult holiday makers have been conducted,3,7-9 we know little about long-term young international travelers, “backpackers,” who have not sought STI treatment.
“Backpackers” are a specific genre of younger travelers. They are travelers, defined by Tourism Australia, who spend at least one night in hostel accommodation during their travels. 11 Visitors from Europe comprised 57% of the total international backpacker market in Australia during 2008 with the United Kingdom (20%) and Germany (10%) contributing the greatest proportion. 12 Since 2000, real annual growth in the market has been from New Zealand (8%), Asia (5%), and North America (4%). Those aged between 20 and 29 years represented 67% of all international visitors. 12 The gender composition of international backpackers has equalized over the past 20 years. 13 Though 7 of the top 10 nations as a source of short-term arrivals in Australia are Asian, 14 their share of the backpacker market is still small and is predominantly represented by Japan and Korea.
Generally, backpackers are considered to travel from developed to developing nations, and therefore overwhelmingly are drawn from “Western nations.” 15 Wishing to travel on minimal budgets and often avoid “mainstream” tourist markets compels them to seek out lower cost, less developed destinations, 16 though long-term backpackers will tend to divide their travel time between casual employment in Western nations (Europe, North America, and Australia) for the purposes of financing travel to developing countries. 17 The gender mix for those backpackers traveling in developing countries tends to show a greater proportion of males (approximately 60%). 15
The backpacker experience has been described as a transition or rite of passage, 18 which in the absence of ones’ own social and cultural constraints of country, community, and family, facilitates situational disinhibition 19 and sensation-seeking behaviors. 20 Not surprisingly, backpackers have a reputation for hazardous alcohol consumption21,22 and frequent sex, 23 potentially with a greater likelihood of unprotected sex and multiple sexual partners when compared with short-stay holiday makers. 24 A cross-sectional study of British backpackers recruited from Sydney and Cairns hostel accommodation found that 40.3% drunk more than 5 times a week compared with 20.7% at home. 21
Hazardous alcohol consumption can impede an individuals’ ability to negotiate safe sex 25 and participants can become laissez-faire about safe sex. 26 In a cross-sectional study of backpackers recruited in sexual health clinics, 53.9% reported “always” using condoms 10 whereas in a community sample in the same area, 40% reported using condoms “always.” 27 A higher prevalence of Chlamydia has been reported among backpackers,10,20 recruited from health service and treatment-seeking populations compared with the general population, but of the few studies reported among a non-treatment-seeking population, Chlamydia infection has been comparable to the overall Australian prevalence. 27
The purpose of this study was to
examine correlations between international backpackers’ alcohol consumption and sexual behaviors and
establish the prevalence of Chlamydia trachomatis and Neisseria gonorrhoea in a non-treatment-seeking convenient community based sample of international backpackers in Brisbane.
Method
This was a cross-sectional study of a convenience sample of non-treatment-seeking international backpackers. The inclusion criteria were defined by the criteria for a “backpacker” as previously defined by Tourism Queensland and being able to understand English. Ethics clearance was obtained from the Metro North Health Service District, Queensland Health, Human Research Ethics Committee. Protocol Number: HREC/09/QPCH/144.
Recruitment
The study location was Brisbane, Australia. Recruitment occurred over a 1-week period in February 2010 using posters, word of mouth, and touting outside the recruitment location. The study itself was conducted at a community health venue located in close proximity to many backpacker targeted businesses, including accommodation and pubs/hotels. It is estimated that approximately 500 to 700 backpackers reside in the immediate area at any time.
Procedures
Participants were asked to self-complete a short questionnaire in English and to undertake a urine based polymerase chain reaction test (Roche Amplicor) for the detection of C trachomatis and N gonorrhoea. Testing was in accordance with manufacturer’s instructions. These tests were included because of the convenience of urine-based testing. On survey completion, participants were provided with “prevention packs” (including condoms, information on standard alcohol drinks, a standard drinks glass, etc). Project team members experienced in sexual health were available for participants to speak with. Participants were reimbursed $AUD20 for their time.
Measures
The questionnaire contained knowledge, attitudinal, and behavioral questions on sexual behavior and on alcohol consumption. These questions were derived from the National Survey of Australian Secondary Students, HIV/AIDS and Sexual Health 28 and the Alcohol Expectancy Questionnaire. 29 Prior to the study, focus tests were held with small groups of international backpackers to determine the feasibility of the methods, particularly acceptability of STI testing, and interpretation of the questionnaire with an international population.
Data Analysis
Data were analyzed using SPSS Version 18. 30 Social and demographic characteristics, sexual health, and alcohol consumption patterns are reported. Correlations were conducted by examining Spearman’s ρ correlation coefficient between variables of interest (arrival companions, number of drinks consumed in a session, drinking frequency, number of different sex partners, number of Australian sex partners, and condom use frequency). Then correlations again using Spearman’s ρ correlation coefficient was conducted with subsets of variables (age, gender, country of origin, ASEAN travel, number of days in Australia, drinking companions, had sex in Australia, alcohol prior to sex, last sex used condoms, last sex regular or casual, taken antibiotics past 3 months, and any STI symptom).
Results
Demographic and Travel Characteristics
A total of 168 backpackers were recruited and completed the questionnaire, with 160 consenting to provide a urine sample. Participants’ median age was 23 years (range = 18-61 years) and 57.1% were male. Most participants (66.6%) arrived in Australia without a partner (38.9% alone, 37.7% as part of a group) and the remainder with their boyfriend/girlfriend (23.2%). Participants were mainly from Britain/Ireland (44.5%), followed by Europe (36.3%). Only 26.2% of participants had traveled directly to Australia from their country of origin, with 32.1% having traveled through Asia, namely Thailand (27.6%), Singapore (18.6%), Cambodia and Laos (17.4%), and Malaysia (15.6%). Participants had been in Australia for a median of 90 days (range = 1-730 days; table not shown).
Alcohol Consumption
Nearly three quarters (72.6%) of participants drank alcohol above the Australian Standard Drinking Guidelines of four drinks in any one session. 31 The mean number of drinks consumed by all participants in any one session was 6.21. Alcohol was consumed on an average of 3.1 days per week (range = 0-7). Nearly 6 in 10 (57.7%) participants reported consuming more alcohol in Australia than at home, although 20.3% reported drinking less compared with home. Alcohol consumption most commonly occurred with the same person or group (59.9%; table not shown).
Sexual Activity
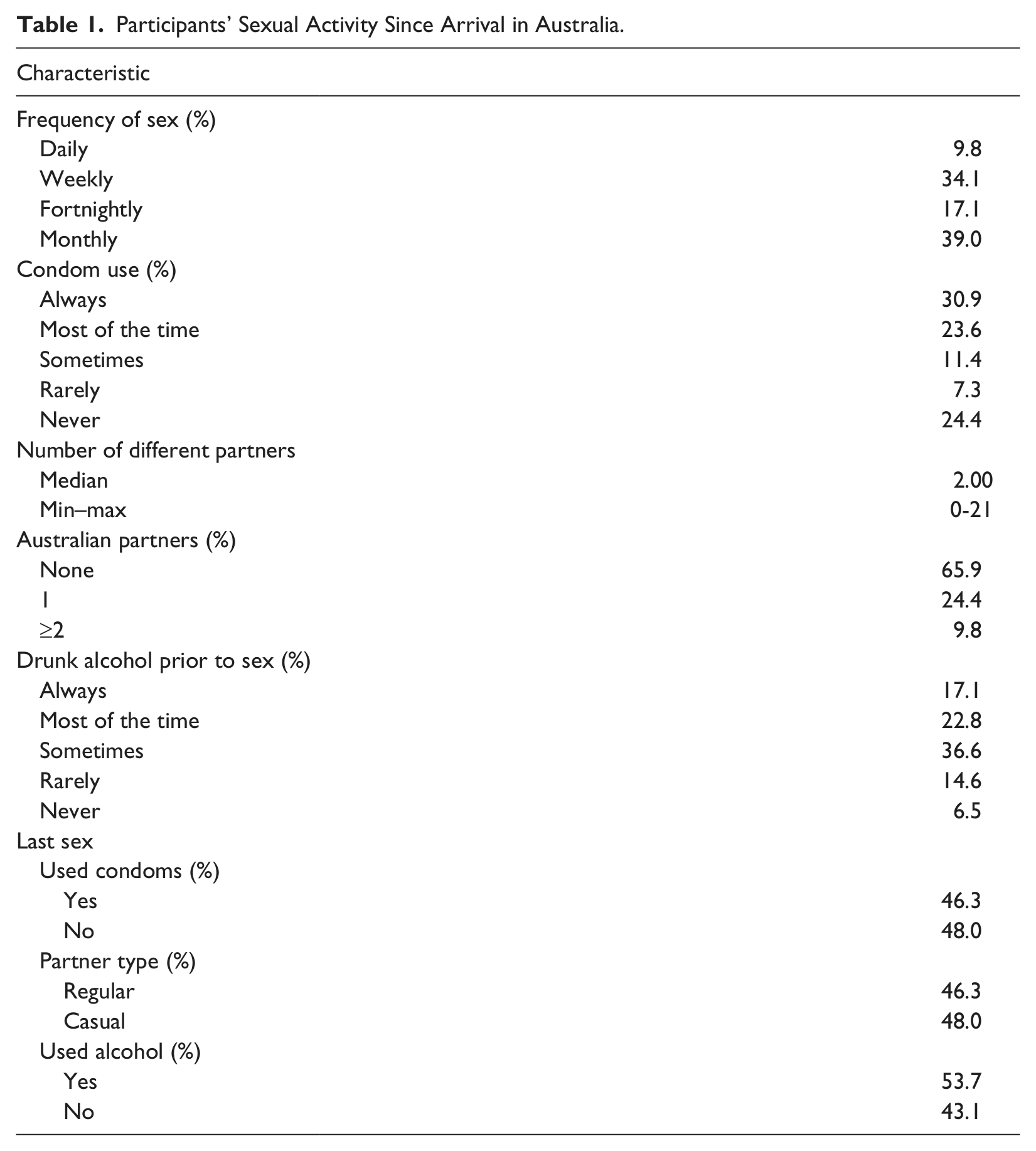
One in 5 participants (20.6%) reported they were having more sex than at home, whereas 30% reported less sex. This paralleled risk perceptions with 21.4% of respondents reporting they felt at greater sexual risk and 37.8% feeling at less or no sexual risk. Nearly three quarters (73.2% N = 123) of participants reported having sex since their Australian arrival, generally monthly (39.0%) or weekly (34.1%). The median number of different sex partners reported was 2 (range = 0-21). In all, 34.2% reported sex with Australian partners. Of those reporting being sexually active in Australia, 54.5% reported using condoms “always” or “most of the time.” The last time these participants had sex, 53.7% had used alcohol, 46.3% had used condoms, and 48.0% reported that they had a casual partner (Table 1).
Participants’ Sexual Activity Since Arrival in Australia.
Prevalence of Chlamydia and Gonorrhoea
Seven out of 160 (4.3%) participants were reactive for C trachomatis and none for N gonorrhoea. The participants diagnosed with Chlamydia were all contacted and given treatment in a sexual health clinic, as well as health information and contact tracing discussions. Participants who tested reactive for C trachomatis were evenly distributed across gender, countries of transit, and arrival status. The majority of those with Chlamydia reported that they used condoms “always” or “mostly,” and had used condoms the last time they had sex. The only significant difference (borderline) between those reactive for Chlamydia and those who were not, was the mean number of different sex partners (4.57 vs 2.12, t = −2.007, df = 156, P = .046; table not shown).
Health Care Usage
In the previous 12 months, 16.1% of all participants reported having experienced symptoms suggestive of an STI. In the past 6 months, 10.2% had been tested for an STI and 5.4% had been tested for HIV. However, 41% had never been tested for an STI. In the previous 4 weeks, 24% had sought medical advice from a pharmacist, 7.8% from a sexual health service and 12% from a doctor. In the previous month, 8.9% had taken antibiotics and 13.3% in the past 3 months.
Correlations
We used Spearman’s ρ correlation coefficient to investigate the relationship between arrival companions, number of drinks consumed in a session, drinking frequency, number of different sex partners, number of Australian sex partners, and condom use frequency. There was a small, but significant correlation between alcohol consumption (r = .293, P < .01), drinking frequency (r = −.242, P < .01), and number of different sexual partners. There were also strong, significant, positive correlations between the number of different sexual partners and Australian sex partners (r = .520, P < .01), and condom use (r = −.548, P < .01; Table 2).
Spearman’s ρ Correlation Coefficient Between Alcohol Consumption and Sexual Behavior.
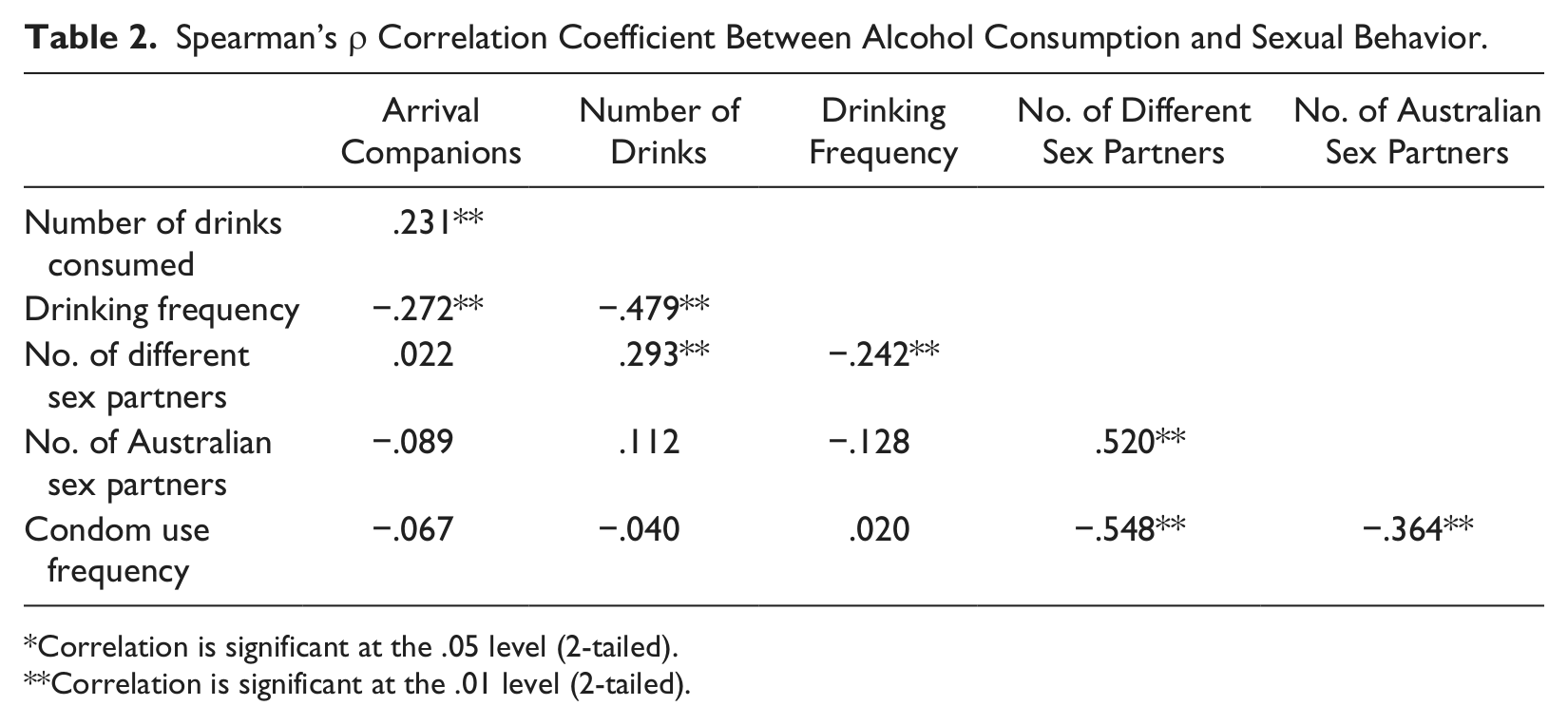
Correlation is significant at the .05 level (2-tailed).
Correlation is significant at the .01 level (2-tailed).
There was a positive correlation between participants who had sex in Australia and their perceived risk compared with their risk at home, with participants having more sex, perceiving themselves to be at greater risk (r = .176, P = .052; table not shown).
We also used Spearman’s ρ correlation coefficient to look at the relationship between variable subsets, arrival companions, number of drinks consumed in a session, drinking frequency, number of different sex partners, number of Australian sex partners, and condom use frequency, with a range of adjustment variables. When considering the 2 recognized sexual risk behaviors—multiple sexual partners and condom usage—a number of strong, significant correlates were identified. Multiple sexual partners correlated strongly with an increased likelihood of having sex in Australia (r = −.630, P < .01), consuming alcohol prior to sex (r = −.623, P < .01), and reporting their most recent sexual partner as casual (r = .469, P < .01). Increased condom usage was positively correlated with having had sex in Australia (r = .591, P < .01), consuming alcohol prior to sex (r = .566, P < .01), and having used condoms at the most recent sexual act (r = .692, P < .01; Table 3).
Spearman’s ρ Correlation Coefficient Between Variable Subsets (Arrival Companions, Number of Drinks Consumed in a Session, Drinking Frequency, Number of Different Sex Partners, Number of Australian Sex Partners, and Condom Use Frequency) With a Range of Adjustment Variables.
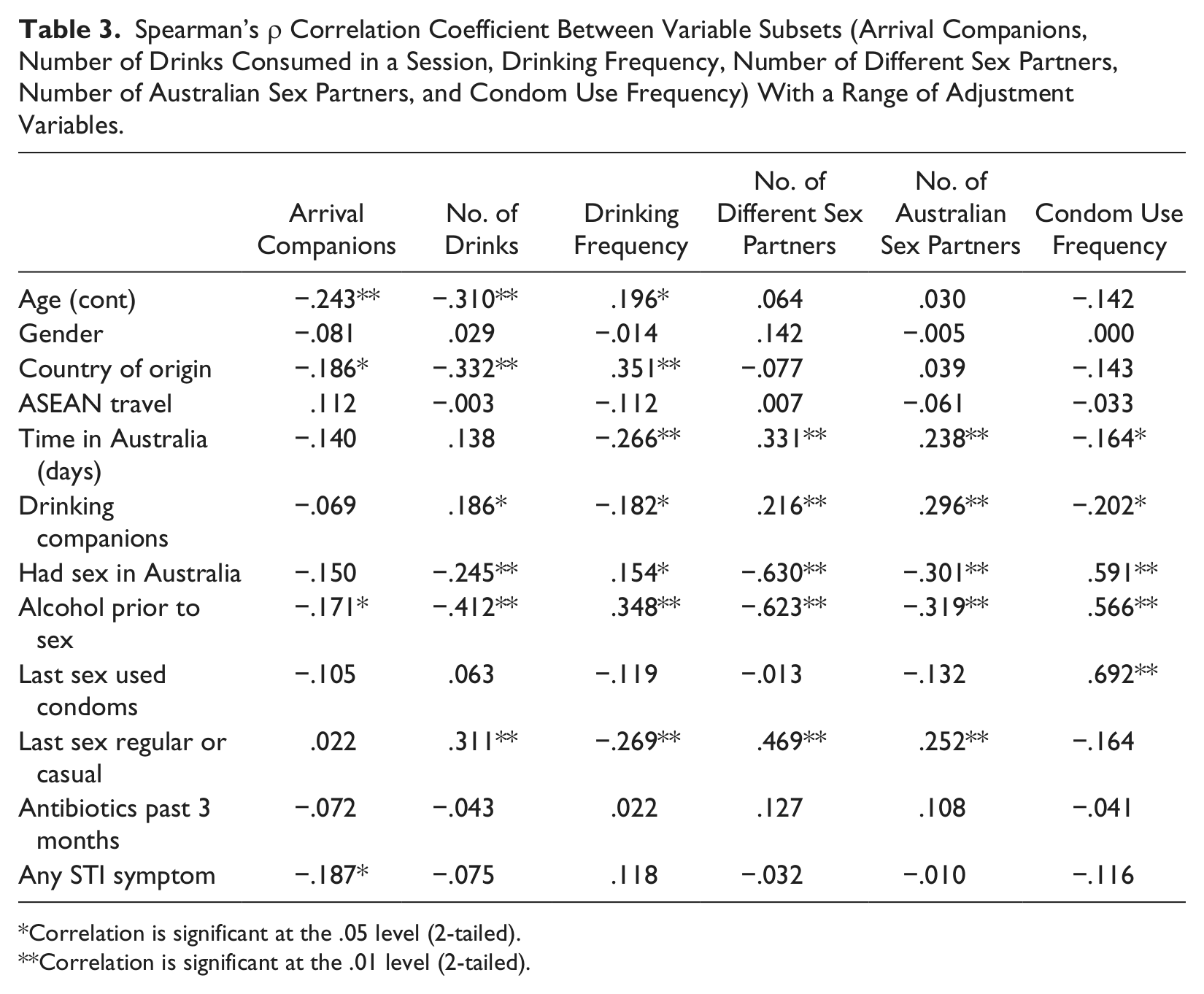
Correlation is significant at the .05 level (2-tailed).
Correlation is significant at the .01 level (2-tailed).
We further investigated participants who reported any STI symptom in the past 12 months and when they last had an STI test. Of those with any STI symptoms (N = 27), 8 had been tested in the past 12 months, 10 had been tested in the past 12 months or more, and 9 had never been tested. The cross-tab comparison between those with any STI symptoms and when tested was not significant (χ2 = 1.385, df = 2, P = .500; table not shown).
Discussion
This study investigated a group of non-treatment-seeking international backpackers’ sexual risk behaviors associated with alcohol consumption. A previous study in 2009 of a community sample of backpackers recruited in Sydney reported a Chlamydia prevalence of 3.5%. 27 Our study identified a 4.3% prevalence of C trachomatis in a Brisbane-based community sample of international backpackers, all of whom were asymptomatic and not seeking treatment or health services. A number of studies have reported Chlamydia infection prevalence in Australia at approximately 4.6%, 32 with a much higher prevalence for some indigenous communities. However, these studies mostly comprise health service and treatment-seeking populations.32,33 Several studies have reported higher prevalence of Chlamydia among travelers, including backpackers,7,20 but these studies were also of health service and treatment-seeking populations. One other community sample of backpackers tested in Queensland reported a Chlamydia prevalence of 7.7%. 34 Approximately 10% of our sample had consumed antibiotics in the previous 1 to 3 months. Although we did not collect information about why or what antibiotics were taken, it is possible that the prevalence in our sample may have been higher, but has been masked by the curative effect of antibiotics.
We found that just more than half the sample consumed alcohol prior to having sex. The number of drinks consumed on a given day positively correlated with the number of sexual partners, greater amounts of sex while on vacation, and a greater perception of sexual risk. This is consistent with other studies that alcohol consumption and sexual risk taking often co-occur.25,35-37
A few correlations with demographic characteristics were apparent in our study. Younger participants were more likely to arrive in Australia as part of a group, to consume more drinks, and to use condoms more often. There was no correlation with gender except for a small effect on number of sexual partners (females reporting less partners). Length of time in Australia was positively correlated with increased frequency of drinking, increased number of sexual partners, including Australian sex partners, and a weak association with the use of condoms. This would suggest that those backpackers extending their stay in Australia as part of a working holiday may pose a more serious public health concern given their greater tendency to have more sexual partners, including Australian partners.
Only a minority of our sample reported sex with Australian partners, confirming the previous Sydney study. 27 Those who reported sex with Australian partners were more likely to have used alcohol the last time they had sex, a greater frequency of condom use, significantly longer times since arrival in Australia, and more different sexual partners (3.9 compared with 1.96). Therefore, the reduced risk of higher condom use needs to be viewed in the context of greater numbers of sexual partners. Consequently, any assessment of the overall epidemiological risk posed by international backpackers should account for the small proportion of backpackers who have Australian partners.
Nonetheless, the role of backpackers as potential bridges for infection is significant given that the majority of travelers pass through Southeast Asia (Thailand, Cambodia, Laos, and Malaysia) where higher prevalence of STIs exist. 38 There are also further concerns for the potential sexual transmission of drug resistant pathogens that are currently a concern overseas, for instance, ceftriaxone-resistant gonorrhoea emergence in Japan and Korea, which are 2 significant tourist markets for Australia. 39 When one considers the asymptomatic nature of many STIs and the window period prior to their possible detection, the epidemiological significance of backpackers passing through high-prevalence countries is significant. However, balanced against this risk is our study’s findings in the past 6 months, 10.2% had been tested for an STI, 5.4% had been tested for HIV, 7.8% had accessed a sexual health service in the previous 4 weeks, and 8.9% and 13.3% had taken antibiotics in the past 1 and 3 months, respectively.
Our study is limited by its relatively small sample size, reliance on English speakers, and the possibility of biased sampling. It relied on a convenience sample, recruited through advertising and the offer of financial reimbursement. Given that the nature of the study was advertised, there is the potential for recruiting interested persons that may show bias toward behaviors under study. Alternately, it is possible that in reporting behaviors during the survey, respondents may have modified their answers, though its anonymity and self-completion may have reduced this. The study did rely on personal recall and perception of the respondent’s level of risk and activity. These are subject to the limitations of any self-analysis. It is therefore difficult to determine the representativeness of this sample in reflecting the overall behavior and infection prevalence of backpackers.
Another limitation is that our study only focused on detecting urethral C trachomatis and N gonorrhoea infection. Our method of sampling and administering interviews constrained us to the collection of urine specimens only and we did not have the capacity to collect swab or blood specimens for either other sites (pharyngeal, rectal) or other infections (HIV, syphilis, herpes simplex virus, HPV). Consequently the prevalence of C trachomatis and N gonorrhoea may have been higher if one were to include other anatomical sites. Additionally, persons with other infections were missed, and therefore the magnitude of risk may be underestimated. However, 16.1% of survey participants did report symptoms in the previous 12 months that were suggestive of an STI (discharge, dysuria, lesion, or lump). Although it cannot be determined whether their recollections are accurate, or whether these symptoms indicate a true STI, the level of self-reported genitourinary symptoms does suggest a higher rate of infection than indicated by our data.
Our survey only asked questions of alcohol consumption and did not include other substances. Although other recreational drugs are used concurrently with alcohol and travel, 40 limitations of time restricted our study to alcohol only given its predominance as the drug of choice for this population. Future studies will need to account for this wider substance use.
The prevalence of C trachomatis in our convenience sample of non-health-seeking individuals identifies this population as a potential core transmitter group. With identified higher drinking and sexual patterns, as well as a moderately higher C trachomatis prevalence among our sample, interventions need to be developed and targeted at backpackers addressing the link between excessive alcohol consumption and sexual risk. However, this small study seems to suggest a more varied picture of the backpacker population and not one to be targeted as a homogenous group of equal risk. This study does reveal that the majority of backpackers confine their sexual activity to other travelers. However, backpackers who arrive alone are more likely to have Australian sexual partners the longer that they stay in Australia. This indicates that public health efforts should be strengthened in the screening and education of those international backpackers who spend longer periods in a host country, given their greater likelihood for having sex with local community members.
Footnotes
Acknowledgements
We are grateful to all participants in the study. Thanks to Professor Michael Dunne, Queensland University of Technology for reviewing the draft manuscript. The views expressed in the article are those of the authors and not necessarily those of Queensland Health, the Ethnic Communities Council of Queensland, or the AER Foundation Ltd.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article:
This study was funded by the AER Foundation Ltd.