
Abstract
This study investigates the factors affecting the timing of antenatal care (ANC) seeking among Bangladeshi women using the 2007 Bangladesh Demographic and Health Survey data. Overall, 52% of the most recently pregnant women sought skilled ANC. The most pronounced reason for not receiving the services was that it was “not needed.” Of the women who sought ANC, 57% entered for ANC at the fourth month or later. The multivariate regression analysis revealed that maternal age, women’s education, residence, wealth index, pregnancy intention status, child’s birth order, and wanting more children were the important determinants of ANC services utilization. Wanting more children and contraception use were no longer independent contributors to late ANC entry. These barriers should also be addressed as part of health interventions through information education and communication programs to early entry to ANC. The need to reduce financial barriers to care is a major implication of this study.
Introduction
Routine antenatal care (ANC) includes medical interventions and advice that a woman receives during pregnancy and is a key entry point for pregnant women to receive a broad range of health promotion and preventive health services, 1 including knowledge about healthy practices during pregnancy, nutritional support, prevention and treatment of anemia, diagnosis, treatment of other diseases, and tetanus toxoid immunization. 2 Late ANC or inadequate attendance at antenatal clinics has been associated with poor pregnancy outcomes, such as low birth weight, prematurity, and increased delivery intervention. 3 However, there is not much literature on the risks and protective factors associated with the timing of ANC for mothers. 4
An estimated 358 000 maternal deaths occurred worldwide in 2008, a 34% decline from the levels in 1990. Despite this decline, developing countries continued to account for 99% of the deaths. 5 Also, a significant proportion of morbidities occur in developing countries. 6 Although ANC might not have the potential to predict and avert obstetric emergencies during pregnancy and childbirth, it exposes women to health education on risk factors and encourages them to deliver with a skilled attendant or in a health facility. 7 Several studies have shown that women who started ANC attendance early and attended frequently were more likely to be assisted during delivery by a skilled attendant compared with those who initiated ANC late and attended only a few visits.8,9 Recent studies have suggested that women who knew about risk factors were more likely to utilize health facilities for delivery than those without this knowledge. 8
Early entry to ANC is important for early detection and treatment of adverse pregnancy-related outcomes. 10 The World Health Organization (WHO) recommends that pregnant women without uncomplicated pregnancies in developing countries should receive at least 4 ANC visits, with the first visit starting before the fourth month of gestation, whereas in developed countries such as the United Kingdom and the United States, ANC is recommended within the first 3 months of pregnancy.11-14 ANC is generally considered to have a positive effect on the health of both the mother and baby. Guidelines in ANC are diverse and not entirely evidence based. 15 Although there is no consensus about the optimal number of antenatal visits, it is proved that inadequate ANC is related to a worse pregnancy outcome.16,17 Thus, it is important for health policy makers to understand what factors have an influence on the timing of ANC visits.
Bangladesh is committed to the fifth Millennium Development Goal (MDG-5) target of reducing its maternal mortality ratio by three-quarters between 1990 and 2015. Since the early1990s, Bangladesh adopted a strategy of improving access to facilities equipped and staffed to provide emergency obstetric care (EmOC). Utilization of ANC increased substantially from 24% in 1991 to 60% in 2004, with a relatively greater increase in rural than urban areas. Professional attendance (medical, midwifery, trained health workers, etc) at delivery increased by 50% (from 9% to 14%, more rapidly in rural than urban areas), and caesarean sections trebled (from 2% to 6%), but these indicators remained low even by developing country standards. 18 ANC and professional attendance at birth were more common among urban, rich and educated women. Disparities become more pronounced at the extremes of the socioeconomic spectrum. Wider provision of EmOC has clearly increased access to obstetric surgery, although much of the increase occurred in the private sector, and only the wealthier women benefit from these interventions. 18 Despite commendable progress in improving uptake of ANC and in equipping health facilities to provide EmOC, the very low utilization of these facilities, especially by poor women, is a major impediment to meeting MDG-5 in Bangladesh. 18
Bangladesh has achieved important health gains over the recent decades, particularly in reducing maternal mortality and infant and child mortality. Despite this, little is known regarding maternal health care services utilization and, in particular, the timing of ANC services use among women of Bangladesh—a developing and agricultural country where the vast majority live in rural areas. Moreover, there may be enormous gaps with regard to utilization of reproductive health care services among women from different socioeconomic strata. This study aims to investigate the factors affecting the receiving of ANC services and, in particular, the timing of ANC among women of Bangladesh using a nationally representative and cross-sectional data set.
The Andersen Health-Seeking Behavior Model
The analysis of health care services utilization is frequently based on the behavioral model developed by Andersen. 19 This model assumes that health-seeking behavior is the result of interaction between characteristics of individuals, the population, and the surrounding environment. 10 The model consists of several main components, such as predisposing components, enabling, needs, personal health behavior, outcomes, and environment. The predisposing component refers to the characteristics of the person and includes demographic, social position, and attitudinal variables. The enabling component consists of conditions that make health care use available to the person. The third component—illness level—is most directly related to health care use and comprises perceived illness and diagnosed illness. In the context of earlier studies, illness level can be translated to pregnancy history and the current course of the pregnancy. 15
Methods
Data for this study have been taken from the 2007 Bangladesh Demographic and Health Survey (BDHS). The 2007 BDHS is a nationally representative survey, which gathered information from 10 996 ever-married women from rural and urban areas. The survey followed a multistage cluster sampling procedure. It obtained detailed information on fertility levels, marriage, fertility preferences, awareness and use of family planning methods, breastfeeding practices, nutritional status of women and young children, childhood mortality, maternal and child health, and knowledge and attitudes regarding HIV/AIDS and other sexually transmitted infections. A total of 6058 births were recorded in the survey from rural and urban areas that occurred during the past 5 years preceding the survey date. Information regarding ANC was collected from the most recent pregnancy of 4905 women and forms the basis of this study. The 2007 BDHS was conducted under the authority of the National Institute for Population Research and Training (NIPORT) of the Ministry of Health and Family Welfare. It was implemented by Mitra and Associates, a Bangladeshi research firm located in Dhaka. Technical assistance was provided by Macro International Inc, through the MEASURE DHS program. Financial support for the survey was provided by the US Agency for International Development (USAID/Bangladesh).The details of the survey are given elsewhere. 20
Outcome Variables
In this study, we considered the most recent births delivered by the women in the past 5 years preceding the survey date. The outcome variables of this study are 2: (1) ANC seeking; and (2) the timing of receiving ANC services. An ANC visit was defined as a contact with medically trained health personnel to follow up pregnancy. All women were asked, “When you were pregnant with (name of last child), did you see anyone for a medical checkup?” Following this, another question was asked: “How many months pregnant were you when you first received ANC for this pregnancy?” The duration of pregnancy was given in continuous form by months. The first outcome variable was dichotomous, and the responses were recorded as either “yes” or “no.” The second outcome variable was classified into: “early entry to ANC,”, “late entry to ANC,” and “did not receive any ANC service.” “Early entry to ANC” was defined as entering ANC before the fourth month of pregnancy, whereas “late entry” was defined as entering ANC at the fourth month or later. This cutoff point was considered following the direction provided by the World Health Organization. 14
Exposure Variables
The ANC visits were analyzed in association with predisposing, enabling, environmental, and illness characteristics as related to the pregnancy. Maternal age and women’s education were the predisposing factors examined. The enabling factor included in this study is the wealth quintile of the households. The wealth index used in this study was developed and tested in a large number of countries to measure inequalities in household income, use of health services, and health outcome. 20 It is an indicator of the level of wealth that is consistent with expenditure and income measures. The wealth index is constructed from data on household assets, including ownership of durable goods (such as televisions and bicycles) and dwelling characteristics (such as source of drinking water, sanitation facilities, and construction materials). To create the wealth index, each asset was assigned a weight (factor score) generated through principal component analysis, and the resulting asset scores were standardized in relation to a normal distribution with a mean of 0 and standard deviation of 1. Each household was then assigned a score for each asset, and the scores were summed for each household; individuals were ranked according to the total score of the household in which they resided. The sample was then divided into quintiles from 1 (lowest) to 5 (highest). The details of the measurement of wealth quintiles have been given elsewhere. 20 The environmental factors included for analyses are region and place of residence, and pregnancy-related determinants are pregnancy intention status and parity.
Sample Size and Statistical Analyses
We used children’s files for this study from the 2007 BDHS raw data set. The births that occurred during the 5 years preceding the survey were recorded in this file. Information such as birth history, birth order, ANC, delivery care, delivery assistance, and postnatal care has been gathered from the respective mothers of the children. To analyze the factors affecting the utilization of ANC service, we included all respondents (4905 women) from whom information regarding ANC services for the most recent birth was collected. This would help improve our understanding of which factors influence the use and nonuse of ANC services. Besides, to capture the impact of the factors on the late receiving of ANC services, we excluded those women who did not receive any ANC service from multivariate analyses. With this background, the sample size for analyzing the late receiving of ANC service stood at 2536 women.
Simple cross-tabulation and bivariate and multivariate statistical analyses were performed in this study. Simple cross-tabulation was undertaken to describe percentage distribution of the sample women. Bivariate techniques—namely, χ2 tests were used to examine the association between the outcome and exposure variables. Multivariate binary logistic regression analyses were conducted to assess the effect of socioeconomic factors on receiving any ANC service and late entry to ANC. Both the outcome variables were made dichotomous. For the first outcome variable, the women who did not receive any ANC service were coded as “0” and “1” otherwise. For the second outcome variable, the women who received ANC early were coded as “0,” and those who received ANC late were coded as “1.” For both outcome variables, the model-fitting process involved 4 stages of estimation. The first model, model I included only predisposing factors. Model II included predisposing and environmental factors. Model III was constructed using the predisposing, environmental, and enabling factors. Model IV, the final model, included all contextual factors considered in this study. The results of the logistic regression analysis are shown using odds ratios with 95% confidence intervals. All the statistical analyses were performed in SPSS v17 (SPSS Inc, Chicago, IL).
Ethical Considerations
The study used nationally representative data extracted from the 2007 BDHS. The BDHS was conducted as a part of the global Demographic and Health Surveys (DHS) program. It was designed to provide data to monitor the population and health situation in Bangladesh as a follow-up to the previous BDHS surveys. The survey was conducted under the authority of the National Institute for Population Research and Training (NIPORT) of the Ministry of Health and Family Welfare. The BDHS followed all protocols prescribed by the WHO. Moreover, the data are widely used for public health issues. Thus, it was not necessary to get the ethical approval of the review board of Islamic University, Kushtia, Bangladesh.
Results
Table 1 shows the percentage distribution of women by their background characteristics. Of the women, 27% gave birth during their teens, 32% were 20 to 24 years old, 22% were 25 to 29 years old, and 19% were 35 years or older. Slightly more than a quarter had no formal education, 31% had some primary education, 36% had a secondary level of education, and 7% had higher education. In terms of wealth index, 22% were poorest, 21% were poorer, 19% were of medium status, 20% were richer, and 18% were richest. The largest group of women was from the Dhaka region, followed by Rajshahi, Chittagong, Khulna, Sylhet, and Barisal regions, respectively. More than three-fifths were from rural areas. Of the births reported, 31% were unintended. Exactly two-fifths of the women reported that they wanted more children, and 58% were current contraceptive users. Almost 32% of the births were first-order, 27% were second-order, 17% were third-order, 11% were fourth-order, and 13% were fifth- or higher-order pregnancies. Just 52% had visited at least once for ANC services.
Percentage Distribution of Women by Their Background Characteristics, BDHS 2007.
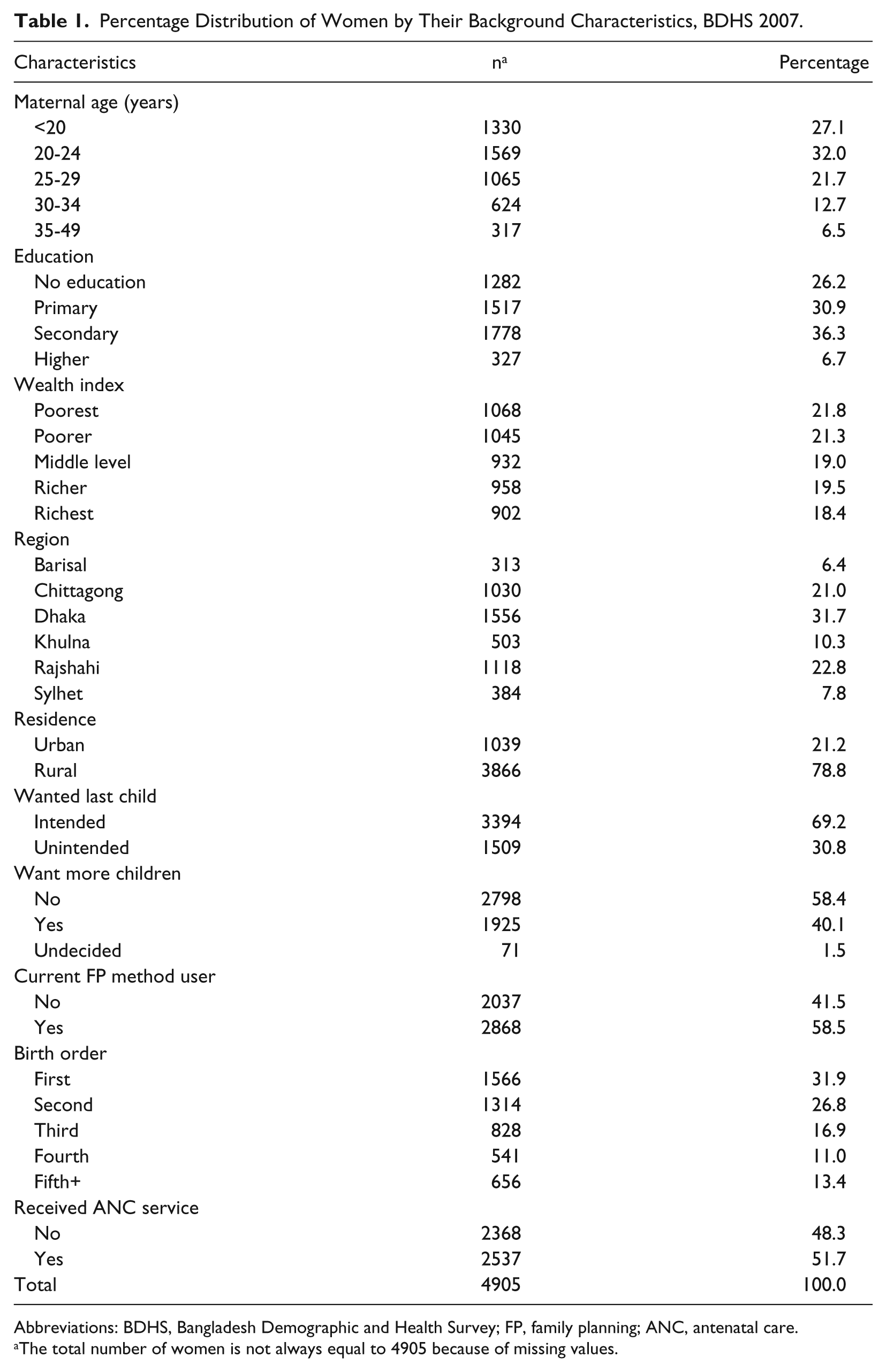
Abbreviations: BDHS, Bangladesh Demographic and Health Survey; FP, family planning; ANC, antenatal care.
The total number of women is not always equal to 4905 because of missing values.
Entry to ANC
Figure 1 shows the percentage distribution of women by the time of first antenatal checkup for their most recent pregnancy. As shown in the figure, 48.3% of the women did not receive any ANC services. Only 2.8% of the women received ANC services in the first month of their pregnancy, 7.5% received ANC services in the second month, 11.8% received ANC services in the third moth, and the rest received ANC services in the fourth month or later.
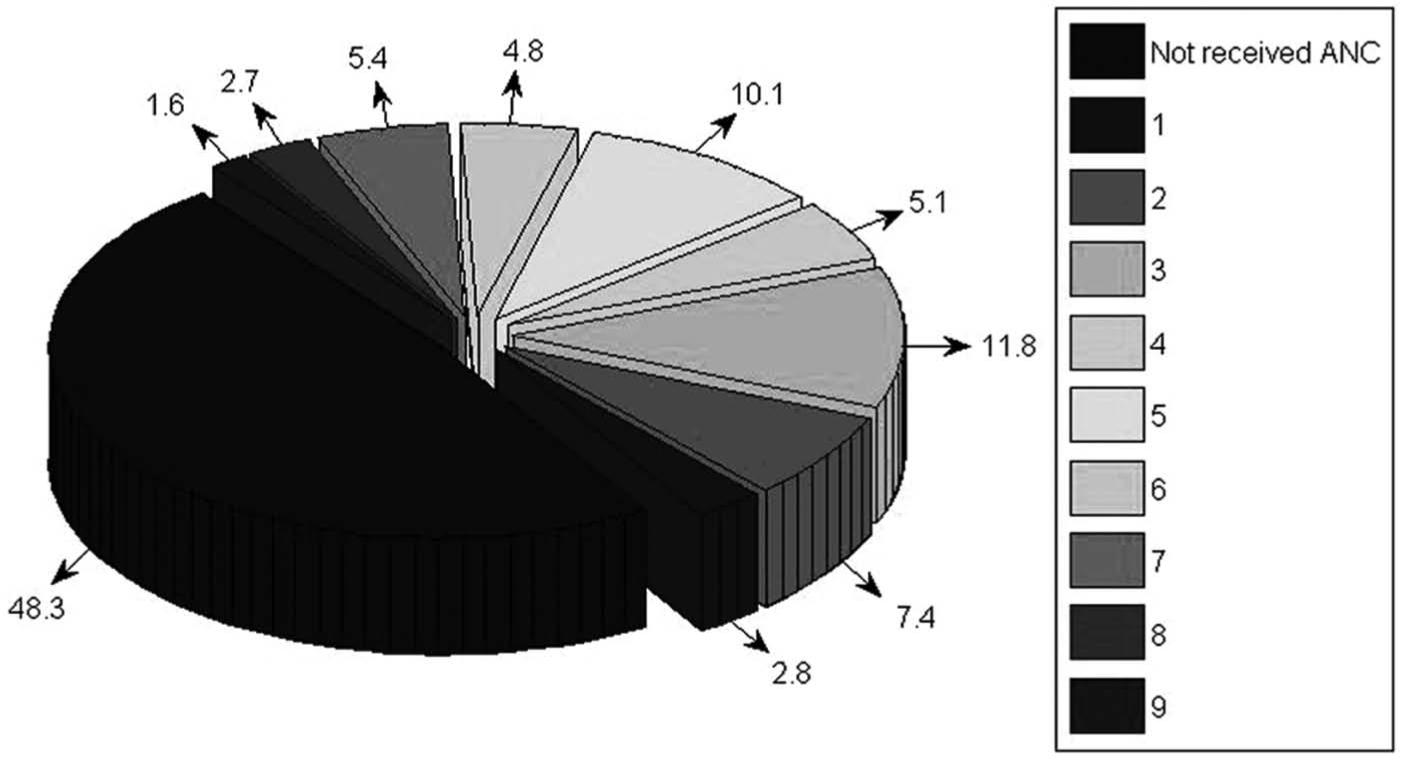
Percentage distribution of women by the time (in months) at first antenatal checkup.
Table 2 shows the early and late entry to ANC visits among women who visited at least once for ANC services, by their background characteristics. As shown in the table, 43% of the women entered early to ANC, and 57% delayed in obtaining ANC services. All the available predisposing, enabling, environmental, and pregnancy-related factors were significantly associated with entry to ANC visits. Late ANC seeking was more prevalent among the young, women with no formal education, the poor, rural residents, women from the Rajshahi region, those with an intended pregnancy, those who desired more children, those who were current contraceptive users, and for third- and higher-order pregnancies.
Prevalence of ANC Seeking Among Women of Bangladesh by Timing and Their Background Characteristics, BDHS 2007.
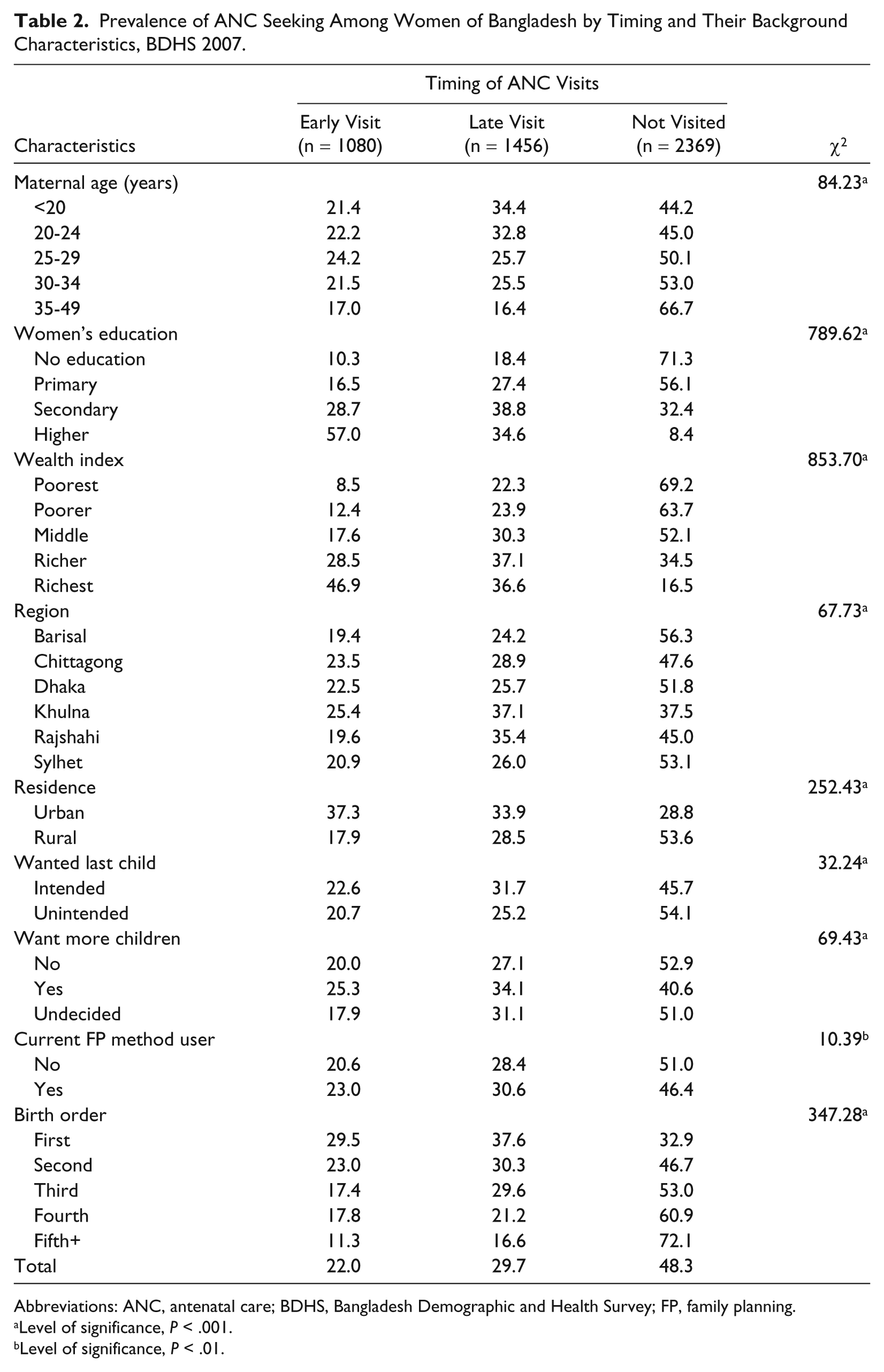
Abbreviations: ANC, antenatal care; BDHS, Bangladesh Demographic and Health Survey; FP, family planning.
Level of significance, P < .001.
Level of significance, P < .01.
Reasons for Not Receiving ANC Services
Table 3 shows the reasons for not receiving ANC for the recent births reported by the women. The women who did not receive ANC services were asked, “Why did you not receive ANC services?” To record the response to this question in the interview schedule, there were 13 closed-ended and coded options, such as too far, inconvenient service hour, unpleasant staff, service too expensive, and so on. From these options, the prompt response provided by the respondents to this particular question was recorded. The most reported reason as mentioned by the women was that “service was not needed” (59.3%), followed by “service was too expensive” (20.4%), “did not know the need of the service” (5.7%), “did not have permission from husband to go for ANC” (4.1%), “the facility place is too far” (3.3%), and “religious reason” (2.6%).
Reasons for Not Receiving ANC Services.
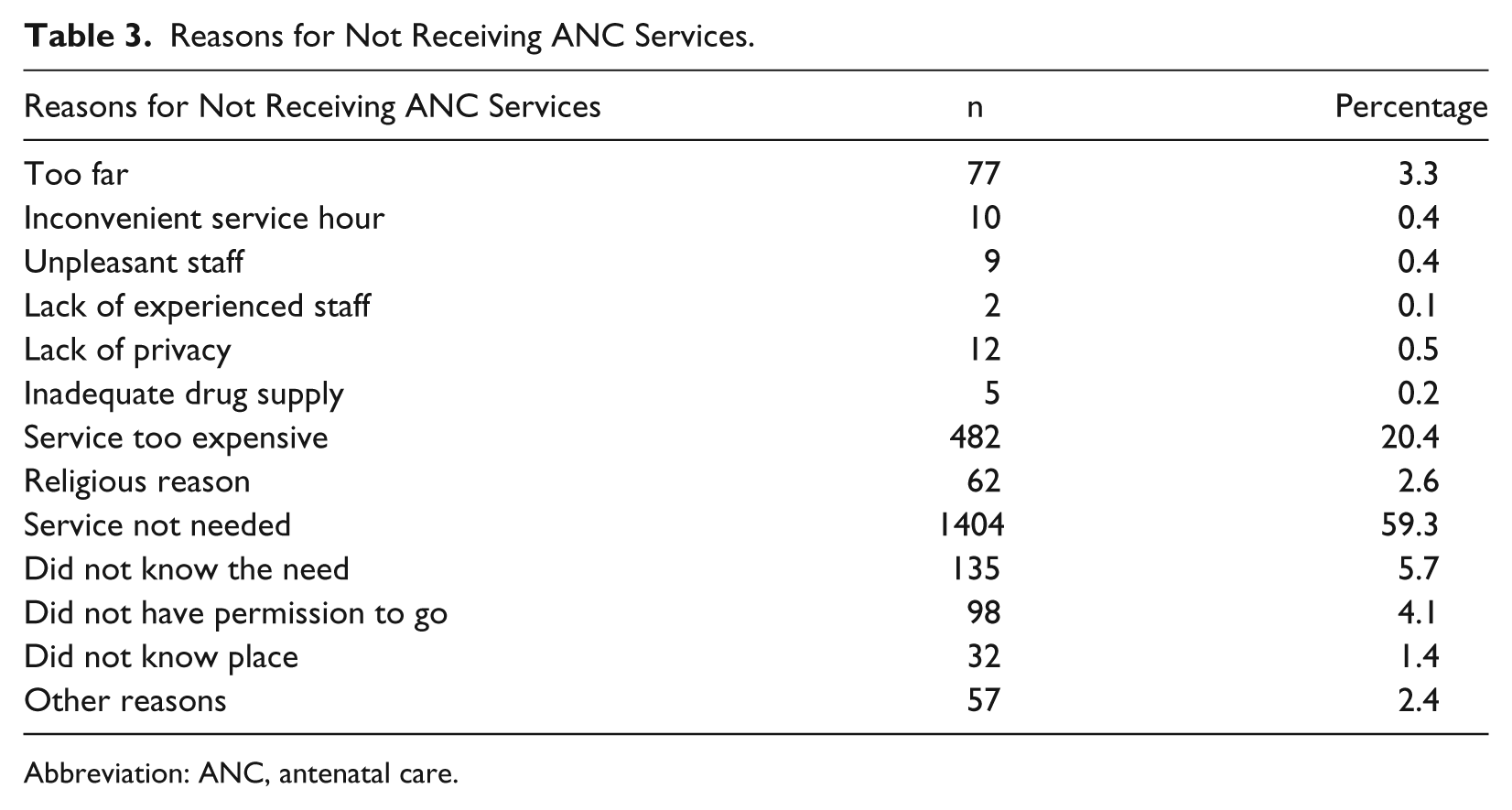
Abbreviation: ANC, antenatal care.
Results of Multivariate Logistic Regression
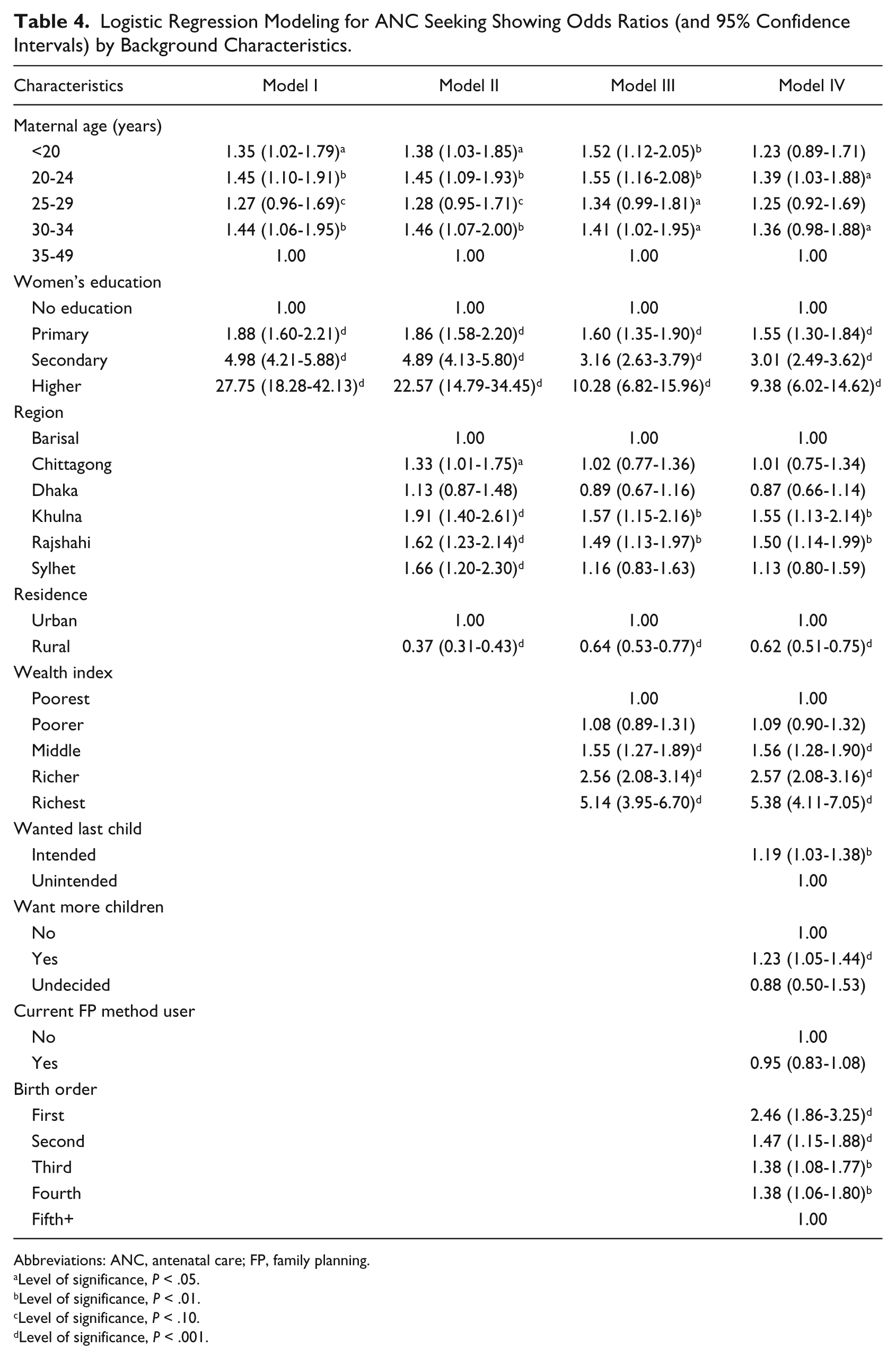
Table 4 demonstrates the results of multivariate logistic regression analyses for ANC seeking among women of Bangladesh. Model I shows that the younger women were significantly more likely to receive ANC services than women aged 35 to 49 years. Women’s education was positively associated with ANC seeking. Model II shows that the effect of age remained unchanged with slight attenuation for women’s education. The women of Chittagong, Khulna, Rajshahi, and Sylhet regions were more likely to receive ANC services than those of Barisal region. As expected, the likelihood of ANC seeking was significantly lower among rural women than their urban sisters.
Logistic Regression Modeling for ANC Seeking Showing Odds Ratios (and 95% Confidence Intervals) by Background Characteristics.
Abbreviations: ANC, antenatal care; FP, family planning.
Level of significance, P < .05.
Level of significance, P < .01.
Level of significance, P < .10.
Level of significance, P < .001.
Model III in Table 4 reveals further attenuation of the effect of women’s education and place of residence on ANC seeking; however, the age effect became sharpened. It also showed regional variation of ANC seeking. The higher the wealth index, the higher the likelihood of ANC seeking. Model IV shows that maternal age, women’s education, region, place of residence, wealth index, pregnancy intention status, wanting more children, and birth order are significant determinants that influence ANC seeking. Being an adolescent age no longer had a significant effect on ANC seeking. Women with intended pregnancies who desired additional children and those with first-order pregnancies were significantly more likely to receive ANC services.
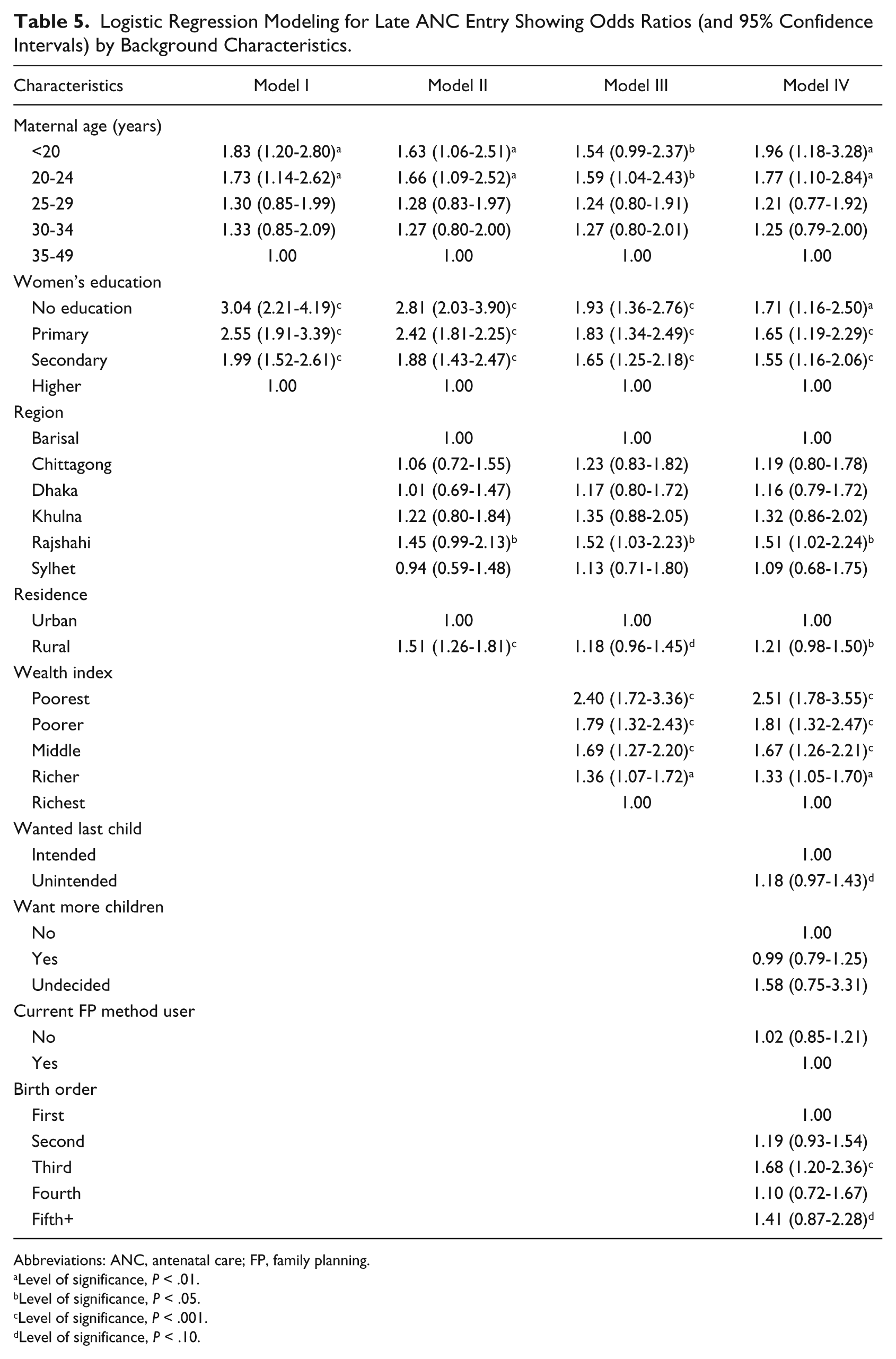
Table 5 shows the results of multivariate logistic regression analyses for late ANC entry. Model I showed that adolescents and young women were more likely to delay ANC seeking than their older counterparts. For instance, adolescents and younger women were significantly more likely to seek ANC services late compared with women aged 35 years or more. Education was significantly related to entry to ANC seeking. The lower women’s education, the more likely women were to seek ANC late. The odds of delay were 3-fold for women with no formal education, more than 2-fold for women with primary education, and 2-fold for women with secondary education compared with women who had higher education.
Logistic Regression Modeling for Late ANC Entry Showing Odds Ratios (and 95% Confidence Intervals) by Background Characteristics.
Abbreviations: ANC, antenatal care; FP, family planning.
Level of significance, P < .01.
Level of significance, P < .05.
Level of significance, P < .001.
Level of significance, P < .10.
Model II showed that the inclusion of environmental factors substantially attenuated the effect of predisposing factors. As compared with women of Barisal division, the women of Rajshahi division delayed significantly more when seeking ANC services. However, there was no significant variation in the likelihood of ANC seeking between the women of Barisal division and those of other administrative regions of the country. Urban women were significantly (P < .001) faster as compared with their rural counterparts in seeking ANC. Model III demonstrates that the inclusion of enabling factors further attenuated the effect of predisposing factors and slightly sharpened the effect of environmental factors. The lower the wealth indexes, the higher the risk of late entry to ANC seeking. For instance, women from the poorest wealth quintile were more than 2 times as likely to enter ANC late as women from the richest quintile.
Model IV shows that all the predisposing, environmental, enabling, and pregnancy-related variables are important determinants of time variation of ANC seeking. The inclusion of pregnancy-related factors increased the effect of maternal age and attenuated the effect of women’s education on ANC seeking, whereas the effect of environmental and enabling factors remained unchanged. Women who reported that their pregnancy was unintended sought ANC significantly later than those who reported their pregnancy to be intended. Women with third and fifth births were much more likely to attend ANC later than recommended compared with those having a first birth.
Discussion and Conclusion
In this study, we examined ANC seeking and the timing of receiving ANC services among women of Bangladesh using cross-sectional and nationally representative BDHS data. The findings showed that 52% of the most recent pregnant women sought skilled ANC from medically trained personnel. Of the women who sought skilled ANC, 57% initiated attendance after the recommended time for first ANC visit, and 43% initiated ANC seeking in due time. When the months were broken down into trimesters, the figure revealed that 22.0% of the women received ANC in their first trimester, 20.0% received ANC services in the second trimester, and 9.7% received ANC in the third trimester of pregnancy. Of the women who did not receive skilled services for ANC, about three-fifths reported that “ANC services were not needed” and one-fifth reported that “the services were too expensive.” This suggests that in Bangladesh, maternal health care services are not yet easily accessible for financial reasons.
Consistent with earlier studies21,22 in developing countries, our findings revealed that although young women were more likely to receive ANC services, adolescents and young pregnant women attended ANC later than their older counterparts. A possible reason for this may be adolescent and young women’s lack of knowledge, power to make decisions, and financial stability as well as concepts of illness. Younger women, especially teenagers, are more likely to have unplanned pregnancies and hence face a scarcity of resources to access ANC services. In contrast, some studies found no significant differences in the timing of entry to ANC seeking among adolescents and adults.7,23 The lack of studies in Bangladesh regarding the late entry to ANC among adolescents and the young as compared with their older counterparts points to the need for further investigation.
Predisposing factors, such as women’s education, have significant effects on both ANC seeking and the timing of ANC seeking. As expected, the lower the education women have, the more likely it is that ANC will be sought late or not at all. Some studies have reported an association between maternal education and receiving ANC services and the timing of ANC initiation. Our findings are in line with the findings of these earlier studies.21,24 Contrary to these studies, there was no evidence of such an effect in some studies. 7 Education is the viable means of gathering knowledge. It is plausible that educated women are better informed and, therefore, more aware of the importance of seeking ANC and other maternal health care services early compared with women with low or no formal education.
Environmental factors such as residence and region were also significantly associated with both the outcome variables. As expected, rural women were less likely to seek ANC services and more likely to enter ANC late compared with their urban counterparts. There was also regional variation in the entry to and receiving of ANC. It is likely that rural women as compared with their urban sisters are not as well educated and poorer, resulting in lower likelihood of entering or late entry to ANC. Variation in the likelihood of ANC in the regions and rural-urban residence are also associated with accessibility, socioeconomic status, and culture and tradition. Many of the sociodemographic and psychosocial characteristics are also associated with late ANC among rural women. Poverty, time management, difficult access, and negative perceptions may be resulting in delay in entry to ANC among rural women and women from some regions of the country.
The enabling factor—the wealth quintile—was found to be significantly positively related to receiving ANC and early entry to ANC. The explanation of this finding is straightforward. Resource scarcity, lack of adequate knowledge regarding the advantage of maternal health care seeking, and lack of autonomy are closely associated with poverty, resulting in lower likelihood of receiving and late entry to ANC services among the poor. Financial barriers posed by high out-of-pocket costs for consultations may be an important determinant of utilization of maternal health services, such as ANC, particularly in areas where poverty is high and for services that are more costly. 25 Thus, financing of health service utilization through insurance or other schemes may reduce these barriers. 26
Our findings showed that unintended pregnancy and multiparity were associated with ANC seeking and also late entry to ANC services utilization. Studies showed that unintended pregnancies are higher among women who were of lower economic status, at an early or late age of reproductive life, not using contraceptives consistently, and attending formal education. 27 Horror, excitement, or pleasure at the discovery of being pregnant for the first time lead to early ANC service utilization. Our findings confirm the findings of previous studies28,29 that show that unintended pregnancies are associated with inadequate ANC, although our finding was attenuated in the multivariate analyses. Although pregnancy intention status was a significant factor in receiving ANC services, it was no longer significantly associated with late entry to ANC.
The study has several limitations. This was a retrospective, cross-sectional data analysis, and there might have been underreporting of age, times and timing of receiving ANC, and other independent exposures. First, in developing countries such as Bangladesh, where vital statistics are not properly maintained, there might have been errors in reports of maternal age. The underreporting may bias the findings of the study. Thus, the findings of this study should be interpreted with caution. The main limitation of this study is that several potentially important factors, such as distance to health facilities, were not included for analyses because of unavailability of information. Despite the limitations, the strength of the study is that it used a population-based and nationally representative large data set.
ANC is vital to achieving good maternal care outcomes in developing countries such as Bangladesh. 30 Financial scarcity and lack of knowledge regarding the importance of service utilization are important barriers to receiving and early entry to ANC. Our findings suggest that interventions that lower financial barriers to receiving and entering ANC are likely to have an impact. Barriers related to education have an independent effect on ANC seeking and late entry to ANC. These barriers should also be addressed as part of health interventions through information, education, and communication programs. Efforts should be made to design interventions that increase early entry to ANC seeking. Promotion of early and frequent ANC utilization through community-based interventions could potentially be scaled up at low cost and adapted to local needs. Research elsewhere reveals that quality of care influences women’s decisions to receive maternal health care services. 7 Thus, at the same time, the quality of ANC services needs to be improved to attract women to use medical care throughout pregnancy, birth, and the postpartum period; outreach services should be offered on a regular basis to bring services closer to women living in very distant settlements. 7
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.