
Abstract
More than one fourth of children of HIV-infected mothers living in Kolkata city are not completely immunized by 12 months of age. This qualitative study aims to explore the barriers to immunization of these children as perceived by their caregivers and the local health care service providers. In-depth interviews were conducted after obtaining written informed consent. Audio recording and hand-recorded notes were used with permission. The transcripts were coded and analyzed using grounded theory. Deteriorating socioeconomic status, tightening of time schedule of caregivers due to illness in the family, stigma, discrimination, and lack of awareness about immunization prove to be major barriers for immunization of the HIV-exposed children. Interplay of these factors coupled with harassment and negative attitudes of service providers toward HIV-affected/HIV-infected people also impede immunization. The intervention efforts need to address these social barriers and adverse life events to improve immunization coverage.
Introduction
Collective denial along with stigma and discrimination makes life difficult not only for the people living with HIV (PLHIV) but also for their family members. Their children, regardless of their HIV status, face social exclusion. The needs of these HIV-infected and HIV-exposed children are not different from other children. Unfortunately, these children are deprived of most of their basic needs for survival due to their parents’ illness. 1 The scenario is the same not only across India but throughout the subcontinent. 2
Universal immunization of children is the most cost-effective and affordable way of promoting child survival. Universal immunization of the HIV-exposed children is of immense importance in the milieu of their deprivations. The World Health Organization and UNICEF have strongly recommended universal immunization among the children of PLHIV guided by the national immunization schedule of the country. 3 Vaccines under the universal immunization program in India are provided absolutely free of cost through the public health system. The goal is to ensure 100% coverage of all eligible children with 1 dose of Bacillus-Calmette-Guérin (BCG), 3 doses of diphtheria-pertussis-tetanus (DPT) and oral polio vaccine (OPV), and 1 dose of the measles vaccine.
HIV-positive status in parents is still a risk for incomplete immunization in the developing world. 4 Information regarding immunization coverage among HIV-exposed children in India is still very limited. The Kolkata metropolitan area in eastern India has been categorized as a high HIV prevalence area through the national sentinel surveillance system. 5 It has been estimated that only 73% of the children with HIV-positive parents in Kolkata are completely immunized at 12 months of age. 6
The universal immunization coverage among the HIV-exposed children in Kolkata is expected to have been 100% as their HIV-infected parents are under the umbrella of the ongoing care and support of the National AIDS Control Program Phase III (NACP III). Moreover, their peer network keeps them in constant contact with volunteers and health care service providers, bringing them into direct and relatively frequent contact with the existing health care programs. 7 Therefore, in this study, we explored the perceived barriers to immunization among the children born to HIV-infected mothers living in the metropolitan areas of Kolkata city and studied the views of health care service providers on issues pertaining to vaccination as a part of the national programs.
Methods
This qualitative study was undertaken among the caregivers of the children born to HIV-infected mothers and health care service providers from the metropolitan areas of Kolkata city. Qualitative methodology was used to explore the experiences, attitudes, values, interactions, and behavior of the respondents in their natural context. 8 A total of 32 in-depth interviews were conducted among the caregivers and the health care service providers of the HIV-exposed children that adequately answered our research question.9,10 Two separate interview guides were prepared for the caregivers and the service providers based on review of the existing literature and the researchers’ experience in the area.6,8-13 The interview guide for the caregivers explored the decision-making process, the perceived barriers to immunization in their children, obstacles from the family, obstacles from the health system, and the enabling factors to access the services. The interview guide for the service providers explored the perceived level of immunization among HIV-exposed children, the barriers to their immunization, obstacles from the family, obstacles from the health system, advice on vaccination, and the factors enabling them to follow the advice. All interviews were conducted during a 2-month period from July 15 to September 14, 2009.
Data Collection
In-depth interviews were conducted after obtaining written informed consent. Audio recording and hand-recorded notes were used with permission. All the interviews were conducted at the drop-in centers. Each interview session lasted between 30 and 40 minutes and was fully transcribed. The caregivers included 22 people who were selected using the list of members of Bengal Network for PLHIV (BNP+), a community-based organization that is representative of the PLHIV of the area. Twenty of the 22 selected caregivers agreed to participate in the study and were called to the drop-in center to be interviewed. The respondents included 17 HIV-infected mothers, 2 grandmothers, and 1 father acting as caregivers for the children born to HIV-positive mothers. The median age of the participants was 27 years, ranging between 22 and 54 years. The highest level of education of the participants was up to primary school, and all were daily wage earners. All the participants were taking care of at least 1 child between 1 and 5 years of age. They together looked after 34 children of whom 14 were female and only 4 were fully immunized. A child was considered to be completely immunized at age 12 months if he/she received 1 dose of BCG, 3 doses of DPT and OPV at an interval of 1 month, and 1 dose of measles by the age of 9 to 12 months. The 2 selected caregivers who did not agree to participate in the study were mothers who could not give time for the interview as they were daily wage earners working at great distance from the drop-in center.
The service providers included 4 female counselors, 2 program managers, and an outreach worker, all with post graduate/masters qualifications in their respective fields. In addition, 5 public and 2 private hospital doctors working in the NACP III in Kolkata metropolitan area were purposively selected for interviews as key informants. Prior appointments were made both over phone and by invitation letter.
Ethical Considerations
Permission to conduct the study in the mentioned areas was obtained from the West Bengal State AIDS Prevention and Control Society. The study was approved by the Technical Advisory Committee and the Institute Ethics Committee of the Sree Chitra Tirunal Institute for Medical Sciences and Technology, Thiruvananthapuram, India. The nature and the objectives of the study were provided, and written informed consent was formally obtained from each respondent who agreed to participate. The participants were assured in writing of complete confidentiality, and the data collected contained no identifiers. All participation was voluntary.
Data Analysis
Transcripts were read and discussed by members of the team, who marked the key passages according to analytical themes. Researchers used the principles of grounded theory for analyses. 12 The analysis was carried out in 2 stages. First, all the interviews were read to identify and list the codes from a selection of interviews. These were then independently coded by another researcher and the differences, if any, were reconciled to develop a final list of codes that were to be used for all the in-depth interviews in each category. The listed codes were subsequently collapsed into thematic groups, and the linkages between these groups were identified by reading and rereading the interviews to identify the possible linkages. Finally, the interviews were reread to finalize the results and correct them to bring it in consonance with all the interviews included in the analysis.
Results
Poor socioeconomic status, lack of time, lack of awareness, stigma and discrimination, and negative attitude of health care service providers are perceived to be the main barriers against immunization of the children born to HIV-positive mothers.
Economic and Time Constraints
The poor socioeconomic status of the caregivers is perceived to be the most important barrier against complete immunization of their children.
So far, our experiences have suggested that people infected with HIV are from a very low socioeconomic background. Ninety percent of these people are so very poor. (Key Informant 1, Allied health care provider) Most of the people come from a poor economic status. Access to health care in general is bad. (Key Informant 8, Pediatrician)
Even though the vaccines are available at public health centers absolutely free of cost, the caregivers cannot take their children for vaccination because they do not have money for the transportation.
I do not have money. . . . I am poor. Going to the vaccination center means spending some money by the way of transport. So, I am not in a mood to take my child there. (Respondent 9, Father)
The HIV-related illness affecting parents of these children bring their financial conditions into a vicious cycle. First, taking a day off from work results in loss of wages. Second, requests to take time off from work are frequently met with refusal from the work supervisor.
Going there would mean spending a considerable sum of money and loss of the day’s wage. . . . I work as a house maid. There was nobody capable of taking my child to the hospital for vaccination as I was busy with my job. . . . I have to take a day off when I go to collect ART. . . . My supervisor does not permit me to take any day offs. . . . I have defaulted many times. (Respondent 3, Mother)
Furthermore, illness in the family reduces the primary caregivers’ resources for catering to the needs of the children and prevents prioritization of timely vaccination of the HIV-exposed child. When the main earning member becomes ill, the family suffers the most and becomes dependent on others.
I am the grandmother. My son is healthy but cannot work as his hand was amputated. My husband is ill, suffering from prostate cancer. He cannot work. . . . My daughter-in-law is an AIDS patient. I am the sole earning member. I work as a maid. (Respondent 5, Grandmother) My husband was not healthy prior to marriage. He used to suffer from frequent bouts of loose stools. . . . After marriage he was very weak. He was very irregular at work. So we faced severe financial hardships for which we had to depend on our in-laws. . . . We do not have the means. We are solely dependent on our in-laws. (Respondent 7, Mother)
The HIV-related or unrelated illness in the family also ties up the primary caregiver’s time and little time is actually left for the child.
For 2-3 months I was extremely busy with my husband before his death and did not have the time to think about my child. . . . I was also ill myself. . . . I had a blood transfusion and ART was started. I was so ill that I could not even wash my clothes. So I could not take my child for vaccinations. (Respondent 1, Mother) The parents who are HIV positive are busy with themselves once they are aware of their HIV status. When husband is positive, his wife becomes so preoccupied, that she finds little time for the child. She forgets to check her child’s immunization card for follow-up. (Key Informant 3, Allied health care provider)
Lack of Awareness
The poor educational status of the caregivers results in a low level of awareness regarding their health needs and the importance of vaccination, leading to incomplete immunization of their children.
I feel those who are socially and economically marginalized suffer from some sort of ignorance regarding access to health care irrespective of their HIV status. They do not come regularly for health care. (Key Informant 6, Allied health care provider)
Some are not aware of childhood immunization at all.
My husband does not stay with me. My mother looked after me during the period of my illness. She had never taken any vaccines in her life and she does not know anything about it. So, she did not keep track on the vaccination of my child. . . . Even we never had any vaccinations and we have grown up to this age. (Respondent 18, Mother)
Others are inquisitive whether vaccinations could prevent HIV infection in their children.
Many people do not know, many people are not aware and some people are not able to access it. . . . . The parents do not know when and how the dose has to be completed. They are not aware of the possible problems arising out of incomplete immunization. (Key Informant 7, Allied health care provider)
Sometimes lack of consensus among the family due to objections from in-laws as a result of local myths, religious beliefs, and peer pressure prevent the parents from vaccinating their children.
My father-in-law conducts prayers at the local mosque. He has prohibited me from vaccinating my child. . . . My husband and I wanted that our child should receive the vaccines. We have vaccinated him secretly on one or two occasions. I had deceived my father-in-law by saying that I am going to my parent’s house. But at the time of measles vaccination and the booster injections, my husband was sick. So my father-in-law had the upper hand and prevented us from taking the vaccination. (Respondent 11, Mother)
Stigma and Discrimination
Stigma and discrimination at the neighborhood or workplace experienced by the family members have serious consequences, including suicide or loss of job opportunities that further aggravate their socioeconomic and time constraints.
My husband was not accepted in the community and he has committed suicide. I am alone but I am determined to save my child from illness. . . . My brother-in-law is not allowed to have lunch with other colleagues. (Respondent 6, Mother)
The HIV-positive mothers face hostile attitudes even at their in-laws house on disclosure of their HIV status.
I have been turned away from my in-laws house due to my HIV infection and now I am living with my parents. (Respondent 14, Mother)
Awareness of their HIV status leaves them, particularly those with little education, in a state of despair and helpless with daily health care needs of the HIV-exposed child. This acts as a demotivating factor for immunization as well.
A sense of despair prevails among the parents that their children’s life span would be shortened. There is no point of giving vaccines to the children. (Key Informant 9, Pediatrician) They suffer from discrimination, loss of emotional support. (Key Informant 4, Allied health care provider)
Attitudes of Service Providers
As a consequence of discrimination, the HIV-positive parents are exposed to hostile attitudes at the local health facility on disclosure of their HIV status. Furthermore, parents of nonexposed children appear to be afraid of these HIV-exposed children and reproved the service providers if they are not served first.
I am afraid they will abuse me seeing my card and knowing my status. I am very much afraid. (Respondent 8, Mother) Whenever we go there, we face a lot of problems. I am very much afraid. I do not want to take my son there anymore. (Respondent 15, Mother) They face discrimination from the health care providers. Some of them may not be aware of even how the transmission of HIV occurs. They are apprehensive that he/she may be affected by mere touching a HIV-positive individual. So in this situation it is expected that immunization is likely to be affected. (Key Informant 5, Allied health care provider) I can tell you about one instance, it is from a rural area. . . . A child was refused immunization by the health worker following objection from the local people. This was at a public health center. . . . I can say the problem is more in private sector. They charge exorbitant for barrier nursing and terminal disinfection. So this is a big problem. (Key Informant 10, Pediatrician)
They are rebuked severely if they miss the day of the immunization or if they ask any questions. The service providers are found to be apprehensive of touching a HIV patient despite knowing that there is no risk of communicating the disease through touch alone. Fear of abuse haunts the mind of the caregivers.
The health workers’ behavior was not good since the beginning and we missed dates. The other children were vaccinated on Wednesdays but my child was vaccinated on Thursdays. The curtains were drawn across all sides. They wore double gloves and deliberately gave pain to my child. . . . They behaved very rudely with us and finally refused to give the vaccines to my child. (Respondent 2, Mother)
In the face of frequent lack of vaccine supply at the health center, the vaccinators did not appear to make it a priority to vaccinate HIV-exposed children at the earliest opportunity, but rather always force them to wait until the end of the sessions when the vaccines stock gets exhausted.
I remember taking my child to the hospital for vaccination. When her turn came we were told that all the vaccines were exhausted and asked to come on another day, and I had to return without giving her the vaccines. This happened twice. Later I had taken her to the hospital again but they refused her the injection since she was having ulcers in the mouth. Even the people standing in the queue shouted at us since we are positive people. . . . I did not have the courage to take her again. (Respondent 19, Mother)
The field-level health workers refuse to visit HIV-positive homes to notify them and make sure vaccinations are performed as per the national guidelines.
Nobody came from the hospital to vaccinate my child although they had come to vaccinate my neighbor’s child a couple of years ago. (Respondent 16, Mother)
The thematic linkages of the concepts that influenced immunization of the children born to HIV-positive mothers are given in Figure 1.
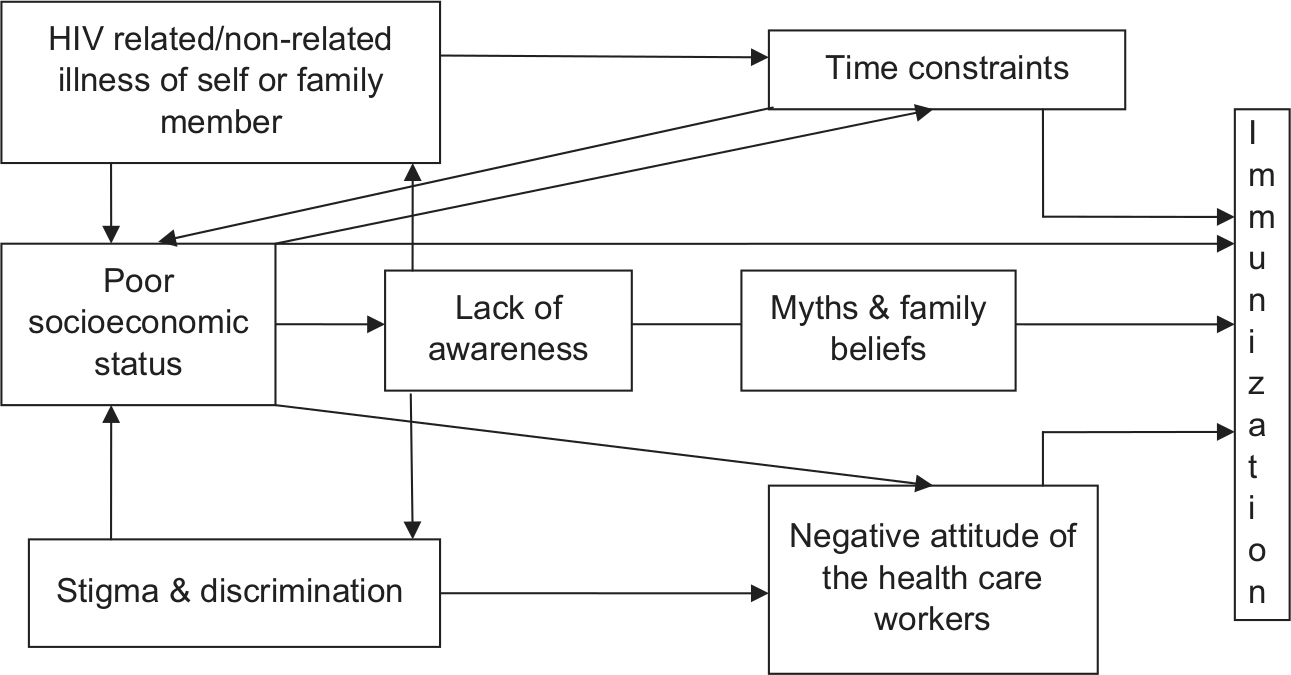
Thematic linking of the concepts that influenced immunization of the children born to HIV-positive mothers.
Discussion
The outcome of this study not only echoes some of the barriers to routine immunization common to all children in Kolkata but also reveals the barriers prevailing by the virtue of their HIV status in their natural context. 8 Socioeconomic status emerges as an important determinant from this qualitative study, which affects all the factors associated with immunization differentially. The HIV-associated illnesses of the parents worsens the economic conditions of the family, turning their plight into a vicious cycle by increasing the cost of care while at the same time reducing income through missed work days and loss of wages. Stigma and discrimination against those with HIV or exposed to HIV leads to uniquely hostile attitudes both at home and at work. Stigma and discrimination may lead to loss or frequent change of job and thereby degrading their socioeconomic status and reinforcing the stigmatized conditions. HIV-positive status thus further aggravates their poverty. As victims of such structural violence, these individuals are predisposed to complications of HIV infection as well as a restricted ability to access care, support, and treatment services including vaccination of their children.2,13 Studies from India and other countries have shown poor socioeconomic status of the caregivers or parents to be a strong marker for incomplete or nonimmunization of their children.14-17 HIV-affected families have poor access to education and incomplete knowledge on health care. Studies have confirmed that the mothers’ education status is an important predictor of immunization of her children.17-19 HIV-infected mothers in this study average a primary school level of education and relatively poor health literacy. Concept of vaccines that is largely unknown to parents or other family members prevents complete immunization.20-22 When the decision-making process regarding the child’s vaccination includes other members of the family, lack of knowledge about vaccination among parents or elders becomes an important issue for incomplete or nonimmunization. Objection from elderly in the family due to religious reasons or superstitious beliefs acts as barrier for immunization. 20 Various myths and the psychosocial barriers among the Muslims including the PLHIV belonging to the Muslim community in India prevents them from getting their children vaccinated.15,20 Domestic problems due to a PLHIV in the family often preoccupy the principal caregiver and thereby hinders the child’s immunization. Illness of the child’s father or the mother due to their opportunistic infections and HIV status not only aggravates their poverty but further tightens the work schedule of the caregiver. The problem is amplified especially where the caregiver is the sole earner for the family. This leads to scarcity of time and opportunity to take the child for vaccination. Poor levels of education coupled with low socioeconomic status, despair, and hopelessness due to their HIV status thus aggravate the “immunization fatigue”.17,23 Stigmatization, discrimination, and harassment of the HIV-infected and HIV-affected people by the health service providers in the country also proves to be a major hindrance for the HIV-exposed children. 22 Inconvenient timings of the immunization sessions at the health center also act as hindrances for immunization of these children. 24 Lack of knowledge about the mechanism of HIV transmission among service providers leads to irrational fear of HIV transmission and poor care. 16 The perceived negative and judgmental attitude and lack of trustworthiness of the service providers affect immunization adversely.16,17,25
Limitations
The respondent caregivers were selected from the list of members of BNP+, but we were unable to access those outside the social network. All the participants had attained their highest level of education only up to primary school and all belonged to the poor socioeconomic category as they were daily wage earners. Some focus group discussions among the caregivers as well as the health care service providers could have substantiated the results even more.
Conclusion
Findings from this study present valuable information that may be applied to the public health care delivery system to improve the vaccination coverage of HIV-exposed children, thereby strengthening routine immunization. The study depicts how the different barriers prevailing in the community influence the decision making regarding the immunization of the HIV-exposed children. The intervention efforts need to address these social barriers and adverse life events in addition to the ongoing care support and treatment. The peer network of the PLHIV needs to be utilized for communication of the needs for universal immunization in the form of simple messages. The overall community awareness about the ways of HIV transmission to allay the stigma and discrimination toward the PLHIV should be the focus of the ongoing behavior change communications. The immunization of the HIV-exposed children depends on strong motivation of all stakeholders to overcome the barriers being identified.
Footnotes
Acknowledgements
We are thankful to the West Bengal State AIDS Prevention and Control Society for providing the permission to carry out the study in the selected areas. We are grateful to Dr Mala Ramanathan, PhD, for her technical comments and suggestions. We sincerely appreciate the help and logistic support provided by the Bengal Network of Positive People and acknowledge the full cooperation and assistance given for the conduct of this study. We are also grateful to Dr Naomi Odell Lundstrom, MD, MPH, for proof editing of the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.