
Abstract
This study investigated the relationship between N5,N10-methylene tetrahydrofolic acid reductase (MTHFR) polymorphisms, smoking, and vascular dementia (VD). Polymerase chain reaction-restriction fragment length polymorphism analysis was used to analyze the frequency of the C/T polymorphism at position 677 of the MTHFR gene in 304 VD patients and 300 control patients with nondementia cerebral infarction. The CC, CT, and TT genotype frequencies of the MTHFR gene were 43.42%, 32.57%, and 24.01%, respectively, in the VD group, and 50.67%, 32.00%, and 17.33%, respectively, in the control group. The T allele frequency was significantly higher in the VD group than in the control group (P < .05). Among patients who smoked, the relative risk of VD in patients with the TT genotype and T allele was higher than in the control group (P < .05). Therefore, the smoking group with the T allele has the highest risk of VD, and synergy appears to exist between the MTHFR gene polymorphisms and smoking in susceptibility to VD.
Keywords
Introduction
Vascular dementia (VD) is a persistent intellectual impairment syndrome that may occur as a result of cerebrovascular disease. The incidence of VD is not only directly related to cerebrovascular disease but also influenced by genetic and environmental factors.1,2 It has been shown that a rise in homocysteine (Hcy) level is an independent risk factor for VD. 3 N5,N10-methylene tetrahydrofolic acid reductase (MTHFR) is a key enzyme in the Hcy metabolic pathway. The mutation C/T at position 677 of the gene may influence the heat resistance of the enzyme, leading to a rise of Hcy in serum. A number of researchers have demonstrated the association between MTHFR gene polymorphisms and cerebrovascular disease.4-6 In a study on gene polymorphism, serum folate, and Hcy in Alzheimer’s disease, Kageyama et al 7 found that the genotype frequency of MTHFR gene TT homozygote in Alzheimer’s disease (21.1%) was higher than in a control group (15%); the serum folate level of patients carrying the TT genotype was much lower than that of the control group (3.5 ng/mg, 35% of control), and the Mini-Mental State Examination (MMSE) score of this group of patients was lower than in any of the other genotypes.
Smoking associated with cerebrovascular disease is a significant cause of death. 8 Smoking can increase blood viscosity, which is an important risk factor in VD, and is often related to environmental factors such as social environment and economy. 9 This study combined analysis of a genetic factor (MTHFR gene polymorphism) and an environmental factor (smoking) to explore their possible synergistic effect on the incidence of VD. The aim of the work was to provide a theoretical basis for the prevention and treatment of VD.
Methods
Study Population
Patients were recruited to the study using the diagnostic criteria of DSM-IV vascular dementia in the Quick Reference to the Diagnostic Criteria by the American Psychiatry Association in 1994: (1) memory impairment; (2) one or more of the following aspects of cognitive dysfunction: (a) aphasia, (b) apraxia, (c) agnea, and (d) executive function disorders; (3) obvious social or occupational hazard caused by any cognitive deficit as defined in (1) and (2); (4) local symptoms and signs in the nervous system of etiological factors related to previous pathological changes, and proof of cerebrovascular disease indicated by laboratory examination; and (5) absence of delirium.
Certain data were required from the patients before acceptance into the study: (1) a clinical dementia evaluation form defining symptoms as light, medium, or severe using the aforementioned diagnostic criteria of VD; (2) a clear disease time-line, including image studies that indicated infarction and bleeding, with dementia appearing within 3 months of infarction and lasting at least 3 months; (3) a score of ≥7 according to the scale for the differentiation of syndromes of vascular dementia (SDSVD), and related symptoms; (4) an MMSE score ≤26; (5) a Hachinski ischemia (HIS) score; and (6) exclusion of dementia of other etiology.
Exclusion criteria were the following: (1) patients with Alzheimer’s disease or other types of dementia; (2) an HIS score <7; (3) patients with severe heart, lung, and kidney dysfunction, severe diabetic patients, and patients with a psychiatric history; and (4) patients not meeting the inclusion criteria shown above, patients for whom the types of symptoms could not be judged, and patients without complete data.
Using the criteria outlined above, 304 inpatients diagnosed with cerebral infarction in the Department of Neurology in our hospital from April 2010 to March 2012 were chosen as the research subjects. They comprised 182 males and 122 females, aged 58 to 75 years, average age of 66.3 ± 6.7 years. The MMSE grading was 9 to 24 (with an average score of 18.7 ± 4.5), in accordance with the American Psychiatric Association’s Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV), and the VD diagnostic criteria formulated by the National Institute of Neurological Disorders and Stroke (NINDS), Switzerland Neuroscience International Research Institute. 10 During the same period, 300 nondementia cerebral infarction inpatients were chosen as the control group, with 179 males and 121 females, aged 57 to 76 years, average age of 67.1 ± 6.9 years The MMSE grading was 27 to 30, with an average score of 28.8 ± 2.6. There was no statistically significant difference between the 2 groups with respect to age or gender (P > .05). All the research subjects were of Han nationality and displayed no hepatic or renal dysfunction, hypothyroidism, malignant tumor, or other diseases.
The experimental VD group and the control group were further categorized into those who smoked (at least 1 cigarette per day for a duration of at least 1 year 11 ) and those who did not smoke. There were 78 smokers and 226 nonsmokers in the VD group and 42 smokers and 258 nonsmokers in the control group.
Sample Collection and DNA Extraction
Five milliliters of fasting peripheral venous blood was drawn in the morning. After anticoagulation by heparin, blood plasma was separated by centrifugation and refrigerated at −20°C until use; the hemocyte was separated and leukocyte genomic DNA was extracted using a small-size blood genome DNA extraction kit (Tiangen Biochemistry Technology Beijing Co, Beijing, China).
The study was approved by the Ethical Committee of Xijing Hospital, Fourth Military Medical University. Informed consent was obtained from the participants.
Detection of MTHFR 677C/T Gene Polymorphism
Polymerase chain reaction-restriction fragment length polymorphism analysis (PCR-RFLP) was used to detect MTHFR gene polymorphism using primers and probes provided by Invitrogen. A forward primer, 5′-TGAAGGAGAAGG-TGTCTGCGGGA-3′, and reverse primer, 5′-AGGACGGTGCGGTGAGAGTG-3′, were used to amplify a 198-bp fragment of the gene. The PCR reaction was carried out in a total volume of 25 µL, including 2 µL DNA, 1 µL Taq DNA polymerase, 0.5 µL of each primer, 0.25 µL dNTP, 1.5 µL Taq buffer with 20 mM Mg2+. PCR amplifying conditions were 5 minutes initial denaturing at 94°C, followed by 35 cycles of 30 seconds at 94°C, 30 seconds at 55°C, and 30 seconds at 72°C, with a further 10-minute extension at 72°C. To detect the restriction fragment length polymorphism (RFLP), 3 µL of each amplified product was subjected to enzyme restriction digest using 0.2 µL Hinf I, 1 µL 10× buffer, 5.7 µL double-distilled H2O, and 0.1 µL bovine serum albumin and incubated in a water bath overnight at 37°C. The digestion products were electrophoresed on a 2% agarose gel at 100 V for 30 minutes and stained with ethidium bromide; results were read on a UV light box.
Statistical Methods
SPSS17.0 software was used for statistical processing, and the allele frequency and genotype distribution in all groups were calculated. The goodness-of-fit χ2 was adopted to detect whether the genotype distribution frequency was consistent with the Hardy–Weinberg equilibrium. The comparison between intergroup genotype and allele frequency was detected by χ2, and results were considered to be statistically significant when P < .05.
Results
Amplification of MTHFR and Detection of 677C/T Genotype
The size of the PCR amplification product fragment was 198 bp. A change from C/T at position 677 of the MTHFR gene produced a Hinf I endonuclease cleavage site, creating 3 possible genotypes The CC wild type produced 1 fragment of 198 bp; CT heterozygosity produced 3 fragments of 198 bp, 175 bp, and 23 bp; TT isozygosity produced 2 fragments of 175 bp and 23 bp (Figure 1).
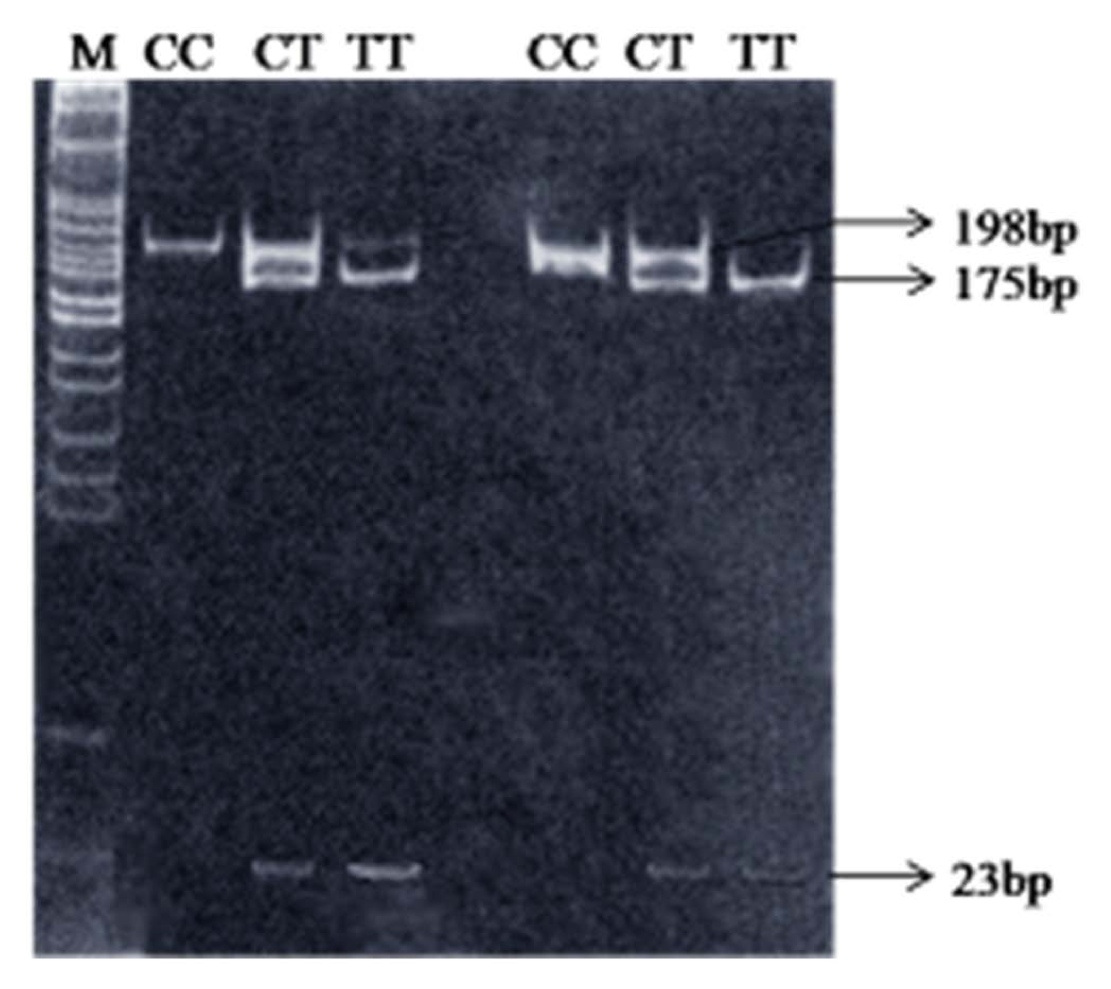
PCR-RFLP result of MTHFR 677C/T.
Comparison of the Frequency Distribution of MTHFR 677C/T Genotypes Between the 2 Groups
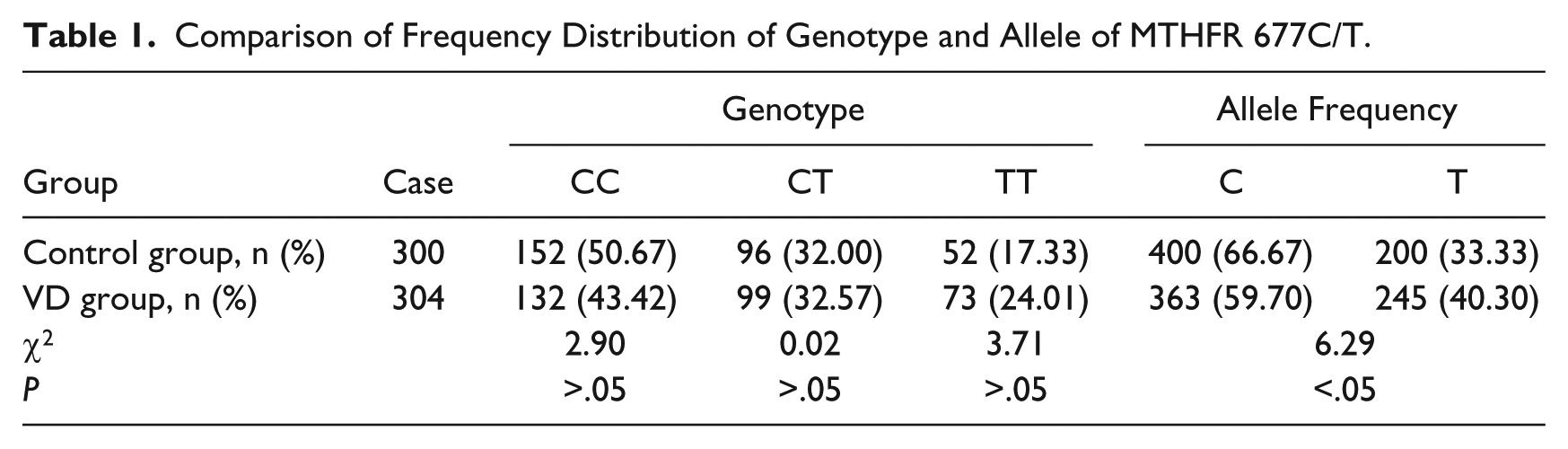
The numbers of CC, CT, and TT genotypes of MTHFR in the VD group were 132 (43.42%), 99 (32.57%), and 73 (24.01%), respectively, while the corresponding numbers in the control group were 152 (50.67%), 96 (32.00%), and 52 (17.33%), respectively. The gene distribution in both groups was in accordance with Hardy–Weinberg equilibrium. Overall, there was no statistically significant difference in the genotype distribution between the 2 groups (P > .05). However, for the T allele frequency alone there was a significantly higher number in the VD group than in the control group (P < .05), which could indicate that the T allele frequency may be related to VD incidence (Table 1). Logistical regression analysis found that the relative risk of suffering from VD for individuals with the CT or TT genotype had no statistical significance (P = .068; Table 2).
Comparison of Frequency Distribution of Genotype and Allele of MTHFR 677C/T.
Correlation of MTHFR 677C/T Genotype and the Relative Risk of VD.
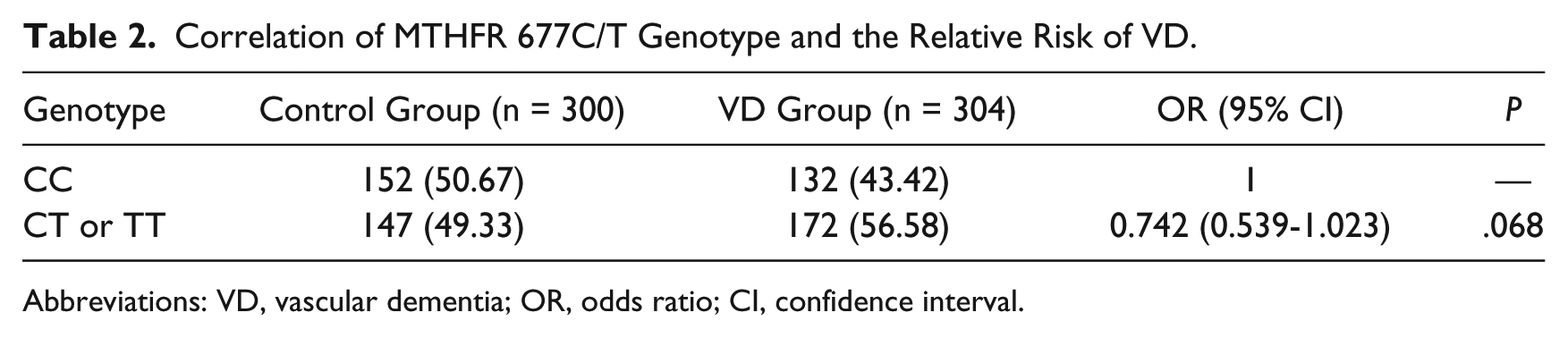
Abbreviations: VD, vascular dementia; OR, odds ratio; CI, confidence interval.
Synergistic Effect of MTHFR Gene Polymorphism and Smoking in VD Incidence
Individuals who smoked and carried the T allele and TT genotype were found at a relatively higher frequency in the VD group than in the control group (P < .05). There was no significant difference (P > .05) in the comparison of genotypes and allele frequencies in the 2 nonsmoking groups. Logistical regression analysis found that the relative risk of suffering from VD for individuals with TT genotype and T allele increased 4.528 times (P = .010), as shown in Tables 3 and 4.
Distribution of Genotype and Allele Frequency of the MTHFR Gene in Smoking and Nonsmoking Groups.
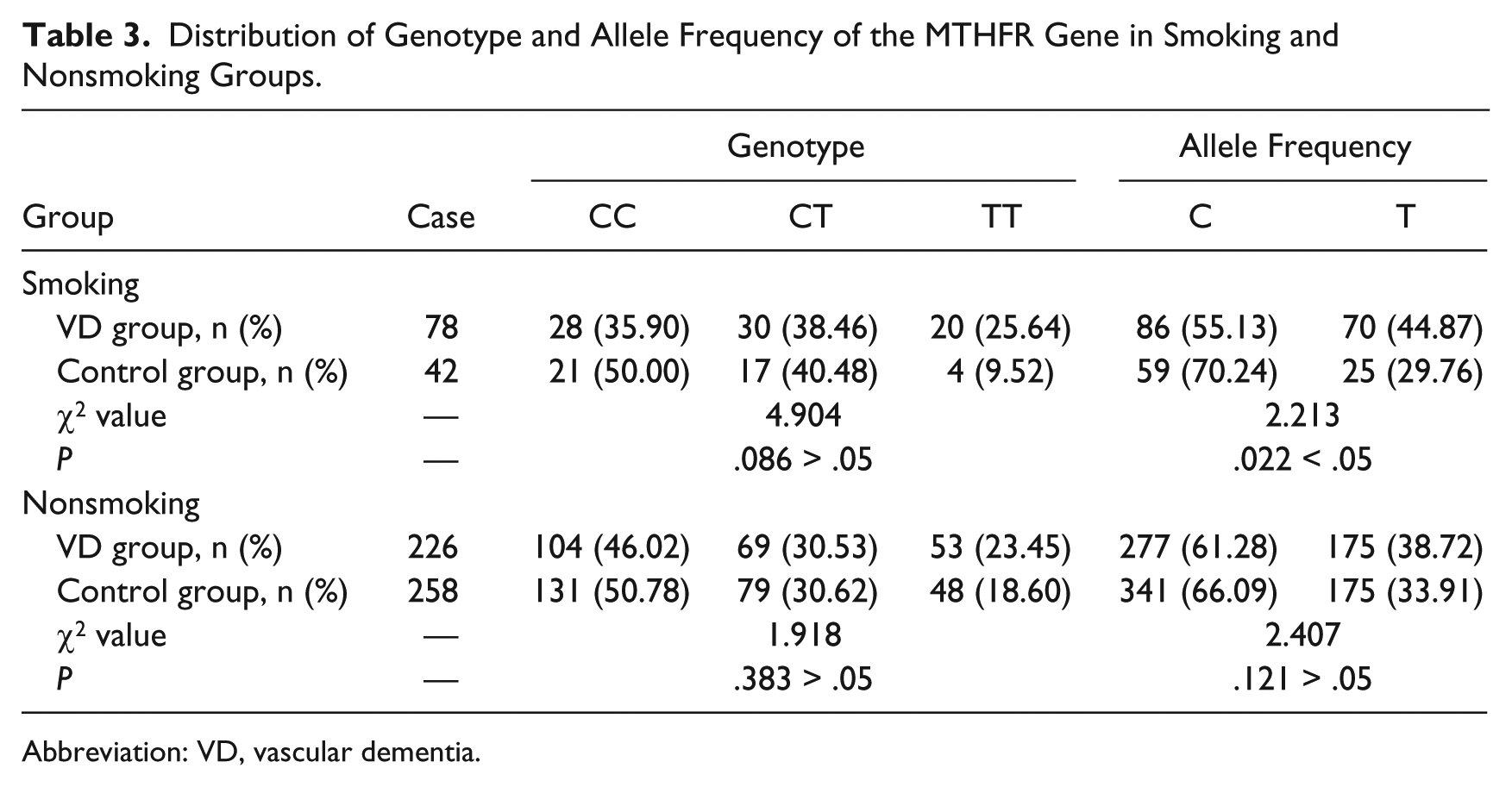
Abbreviation: VD, vascular dementia.
Correlation Between Smoking, TT Genotype, and the Relative Risk of VD.
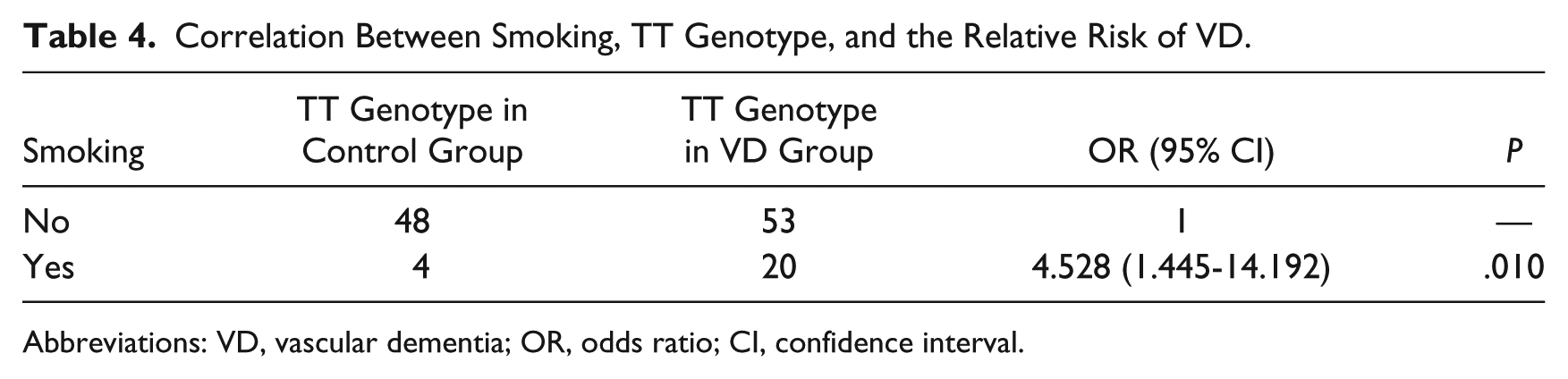
Abbreviations: VD, vascular dementia; OR, odds ratio; CI, confidence interval.
Discussion
VD, the second most common dementia after Alzheimer’s disease, is a clinical syndrome of intellectual and cognitive dysfunction caused by cerebrovascular disease.12,13 Compared with other types of dementia, VD has a better prognosis and can be prevented to a certain extent. It is very important to discuss the risk factors, since targeted prevention has important clinical significance. At present, the study of risk factors for VD is still in its initial stages. However, it can be confirmed that the causes of VD are multifactorial, including not only the vascular factors but also genetic and environmental factors.
In recent years, studies related to candidate genes considered to be associated with VD have mostly focused on the genes related to the production and processing of blood plasma Hcy. Hyperhomocysteinemia (HHCY) is one of the known dependent risk factors of VD. 14 The MTHFR gene is a key enzyme in the Hcy metabolic pathway, N5,N10-methylentetrahydrofolate, and can be reduced 5-methyltetrahydrofolic acid 15 so as to maintain the normal Hcy level in the human body. Replacement of the basic group C by the basic group T in the MTHFR gene at locus 677 causes the encoding amino to be changed from alanine to valine. This mutation produces a fall in MTHFR activity, leading to a rise in Hcy and a consequent rise in VD incidence risk.5,16,17 In this study, the numbers of CC, CT, and TT genotypes of MTHFR in the VD group were 132 (43.42%), 99 (32.57%), and 73 (24.01%), respectively, while the corresponding numbers in the control group were 152 (50.67%), 96 (32.00%), and 52 (17.33%), respectively. There was no statistical significance in the genotype distribution in the 2 groups (P > .05). However, the T allele frequency in the VD group was obviously higher than that in the control group (P < .05), which indicated that the increased T allele frequency might be related to VD incidence.
Smoking as an independent risk factor can increase the VD incidence rate, a fact already verified by many epidemiological studies.18,19 The intake of tar, nicotine, and other toxic substances from tobacco into the human body can stimulate the autonomic nerves, cause vasospasm, elevate blood pressure, raise blood cholesterol, and accelerate a form of atherosclerosis. 20 Furthermore, smoking produces carbon monoxide, changing the oxygen dissociation curve, leading to brain anoxia-ischemia, further causing dysfunction of the brain stem and inducing dementia. Some studies suggest that smoking and other external factors induce VD through genetic factors. 21 In a study on the relationship between secondhand smoke inhalation, vascular diseases, and dementia incidence, Barnes et al 22 found that secondhand smoking inhalation and vascular disease may have a synergistic effect in the dementia development. Passive smoking or inhalation of secondhand smoke has also been shown to have long-term and direct side effects on the cardiovascular system, including increase in platelet viscosity, endothelial dysfunction, and heart rate variability decline. In addition, endothelial dysfunction might be related to the decrease in clearance rate of β-amyloid protein, which is thought to be related to Alzheimer’s disease. 22 This study showed that compared with the control group, the smoking group carrying the TT genotype and T allele had a relatively higher risk of VD (P < .05). There was no significant difference (P > .05) in the comparison of genotypes and alleles between the 2 nonsmoking groups. This leads us to conclude that the rise of VD risk via smoking may be associated with the T allele gene mutation and that the MTHFR gene polymorphism and smoking are working synergistically in increasing the VD incidence.
Footnotes
Authors’ Note
Pengpeng Jin and Shuangxing Hou are co–first authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Fund Project for “Shaanxi Key Technologies R&D Program,” No. 2011K12-33.