
Abstract
To evaluate proportion and predictors of poor response in infants and appraise booster seroprotection, we surveyed 2047 infants in Shanghai and detected antibody to hepatitis B (HB) surface antigen (anti-HBs). Poor responders were randomized into 2 groups, given booster with 5 µg and 10 µg hepatitis B vaccine (HepB), respectively. Proportion of infants with titer <10 mIU/mL and 10 to 99 mIU/mL was 1.86% and 15.14%, respectively. Multivariate logistic regression suggested infants of male, aged 13 to 18 months, premature, administered with 5 µg HepB or mother positive for HB surface antigen (HBsAg) and HBe antigen (HBeAg) would more likely develop worse response. Difference of geometric mean concentration between the first and full booster was not statistically significant both for 5 µg and for 10 µg HepB groups. The seroprotective rate were higher for infants with 10 µg HepB than those with 5 µg HepB (P > .05). Therefore, it is concluded that booster for poor vaccinees with 10 µg HepB could achieve satisfactory seroprotection.
Introduction
Hepatitis B (HB) is caused by infection with the hepatitis B virus (HBV) and is one of the world’s most prevalent and severe infectious diseases. At present, approximately 350 million people are chronically infected with HBV worldwide. 1 While most of the chronically infected people reside in Asia, Africa, and Latin America, more than 8 million live in Europe and the United States, where the prevalence is up to 8% and higher in defined populations. 2 Prevention of HBV infection has taken a significant step forward since the availability of, first, plasma-derived hepatitis B vaccine (HepB) and, later, yeast-derived vaccine. Since China adopted HepB into the Expanded Programme of Immunization (EPI) in 1992, the prevalence of HBV in children has decreased dramatically. According to results of the national population HB sero-epidemiology surveyed in 2006, the national prevalence rate of hepatitis B surface antigen (HBsAg) in children aged 1 to 4 years was only 0.96%, and compared with 1992, the HBsAg carriers in children decreased by nearly 80 million. 3 Although the protective effect of HepB has been observed worldwide, 5% to 10% of individuals with the standard 3-dose primary immunization schedule at months 0, 1, and 6 failed to mount an adequate titer of antibodies to hepatitis B surface antigen (anti-HBs).4-9 Reasons for the lack of an effective antibody response are multifactorial, including obesity, male gender, immune suppression, as well as genetically related, and offer a challenge for research.10-15 Anti-HBs titer <10 mIU/mL is considered as “nonresponse” to vaccination and these vaccinees have difficulty in avoiding infection with HBV. Besides, having an anti-HBs titer of 10 to 99 mIU/mL is regarded as “low-response” to vaccination, and the cutoff of 100 mIU/mL is recommended by some European health authorities as seroprotection in persons at increased risk of infecting HBV.16,17 An anti-HBs level ≥100 mIU/mL is desirable, and therefore, this higher cutoff level has been used in this study.
Shanghai is an international metropolis in east China with 18 districts, with 6 districts initiating the HepB vaccination for neonates in 1986. Plasma-derived HepB was offered to newborns with HBsAg-positive mothers. In 1989, the scheme was expanded to 12 districts, and all newborns, regardless maternal infection status, were offered vaccination. Meanwhile, neonates with HBsAg and hepatitis Be antigen (HBeAg)–positive mothers in other nonpiloting districts were also in the vaccinating population. From 1992, plasma-derived HepB were administered to all neonates in Shanghai, and recombinant yeast-derived HepB replaced plasma-derived HepB in 1997. Since November 2003, HepB had been brought into the free EPI, which further promoted the vaccination of HepB in Shanghai.
The purpose of present study was to evaluate the proportion and predictors of poor response in infants after 3 dosages of primary immunization with recombinant yeast-derived HepB in Shanghai. Furthermore, the study also assessed the effectiveness of booster immunization using different types and dosages of HepB in nonresponders and low responders.
Materials and Methods
Study Population
In July 2010, 3 districts (JiaDing, Qingpu, and Chongming) in Shanghai were selected as study sites, where a total of 2047 infants aged 7 to 18 months who had lived in a local district for more than 6 months were enrolled. These infants were vaccinated with a 3-dose schedule HepB soon after birth. Either 5 µg HepB made by recombinant DNA techniques in Saccharomyces cerevisiae yeast (HepB-SCY) or 10 µg HepB made by recombinant DNA techniques in Hansenula polymoarpha yeast (HepB-HPY) were administered at 0, 1, and 6 months.
Data and Sample Collection
Data were collected using interviewer-administered questionnaires in August 2010. Interviews were conducted in private rooms, and local interviewers accepting the training in the survey methodology were employed. Questionnaires generally consisted of birth state, HepB vaccinating history, family history of HBV infection; and all questions were close-ended. After questionnaire administration, 2 mL of venous blood specimens were collected for anti-HBs titer testing. Vaccinees with anti-HBs titer <l0 mIU/mL and between 10 and 99 mIU/mL were regarded as “nonresponders” and “low responders,” respectively. Subjects were considered seroprotected when the anti-HBs titer was ≥100 mIU/mL.
Laboratory Analysis
Anti-HBs titer were to be measured in a single licensed laboratory by a chemiluminescence microparticle immuno assay, according to the procedures recommended by the manufacturer (Abbott Labs, Abbott Park, IL). HBsAg was tested when the anti-HBs were lower than l0 mIU/mL.
Booster Immunization
Nonresponding and low responding infants were randomized into 2 groups and given a 3-dose booster immunization with schedule of 0, 1, and 6 months with 5 µg HepB-SCY (Shenzhen Kangtai Biological Products, Guangdong, China) or 10 µg HepB-HPY (Dalian Hissen Bio-pharm, Liaoning, China). Each HepB-SCY and HepB-HPY contained 5 µg/0.50 mL of HBsAg and 10 µg/0.50 mL of HBsAg, respectively. These 2 vaccines are the often used HepB for infants in China currently, and the quantity of HBsAg protein per dose of HepB conforms to the World Health Organization position paper on HepB. 18 Anti-HBs titer was assessed on the follow-up visit at the first and the seventh months.
Ethical Clearance
The objectives and methods of this study were clearly explained to the guardians of infants. Informed written consent from guardians was obtained before collection of data. The ethical approval for the study was obtained from the ethics committee of the researching institution, and the study was conducted in full compliance with the principles of the Declaration of Helsinki.
Statistics
All tests were performed 2-sided at the 5% significance level. The Pearson χ2 test and Fisher’s exact test were performed to analyze the association between response status and subject characters. The backward stepwise (entry and removal probability was .05 and .10, respectively) multivariate logistic regression analysis was conducted to identify the association of chosen variables with vaccine response status, in which dependence was set to a dichotomized variable, and all independent variables were categorized. The natural logarithm-transformed anti-HBs antibody titers for different HepB groups were compared by the independent-samples t test, and the MIXED procedure was performed for analysis of the natural logarithm-transformed anti-HBs antibody titers between post-first and post-full booster. The anti-HBs seroprotection for different HepBs was compared using Pearson’s χ2 test. The CATMOD procedure was performed for analysis of categorical repeated measurements such as the difference of anti-HBs seroprotection between post-first booster and post-full booster. All statistical analyses were performed using Statistics Analysis System 9.2 (SAS 9.2; SAS Institute Inc, Cary, NC).
Results
General Characteristics
A total of 2047 infants were recruited including 1060 males and 987 females. The infants aged 7 to 12 months and those aged 13 to 18 months accounted for 47.19% and 52.81%, respectively. Premature infants (<37 weeks) accounted for 3.08%, and partus maturus infants (≥37 weeks) accounted for 96.92%. As for HepB primary immunization, infants vaccinated with 5 µg HepB-SCY and 10 µg HepB-HPY accounted for 74.79% and 25.21%, respectively. There were 46 (2.25%) infants whose mothers were positive for both HBsAg and HBeAg.
The post-primary vaccination anti-HBs titer ranged from 14982.70 mIU/mL to 0.52 mIU/mL, and with a geometric mean concentration (GMC) of 408.04 mIU/mL (95% confidence interval [CI] = 383.43-432.58). Altogether, 38 (1.86%) infants were classified as nonresponders, 307 (15.14%) were classified as low responders, and 1699 (83.00%) developed protective antibody titer (>100 mIU/mL). Only one 15-month-old, partus maturus infant with normal birth weight who completed primary immunization with 10 µg HepB-HPY had undetectable anti-HBs and was positive for HBsAg. His mother was positive for both HBsAg and HBeAg.
Poor Response After Primary Immunization
The univariate analysis of response after primary immunization is shown in Table 1. The proportion of nonresponse and low response was notably lower in infants aged 7 to 12 months than those of infants aged 13 to 18 months, with statistically significant difference (P < .05). There were no differences in response status between gender and body mass index (BMI, cutoff of 18; P > .05). Prematurity was significantly associated with poor response (P < .05). However, there was no statistically significant difference in birth weight or delivery mode among infants with different response status (P > .05). The proportion of nonresponse and low response in infants who received 5 µg HepB-SCY was significantly higher than those who received 10 µg HepB-HPY (P < .05). Infants whose mothers were positive for both HBsAg and HBeAg developed poorer response (P < .05). Whether the mother had received hepatitis B immunoglobulin (HBIG) during pregnancy had no effect on the response status of infant (P > .05).
Univariate Analysis on Factors Associated With Nonresponse and Low Response to Neonatal HepB Vaccination.
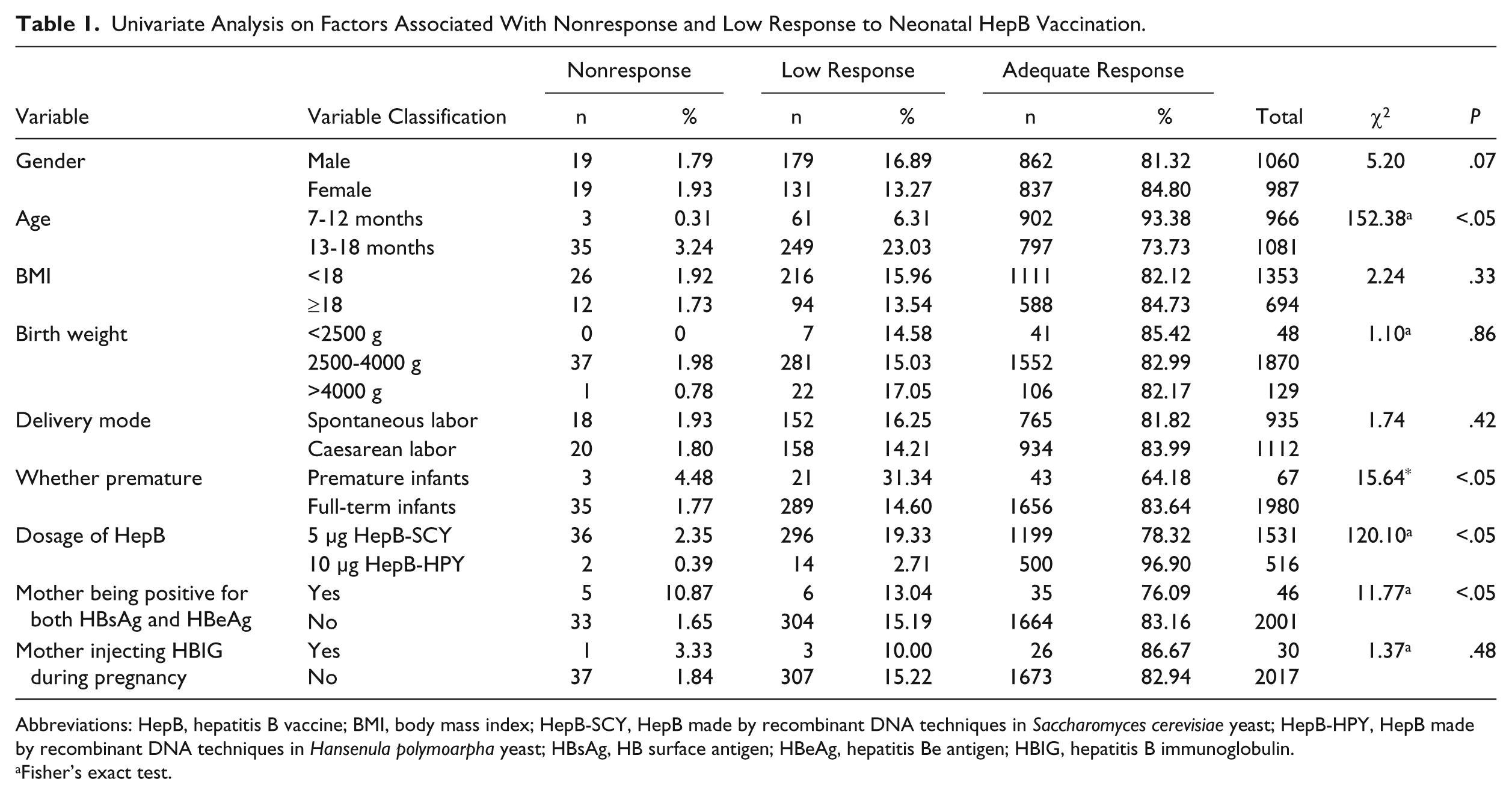
Abbreviations: HepB, hepatitis B vaccine; BMI, body mass index; HepB-SCY, HepB made by recombinant DNA techniques in Saccharomyces cerevisiae yeast; HepB-HPY, HepB made by recombinant DNA techniques in Hansenula polymoarpha yeast; HBsAg, HB surface antigen; HBeAg, hepatitis Be antigen; HBIG, hepatitis B immunoglobulin.
Fisher’s exact test.
The backward stepwise logistic regression model was fitted to analyze the predictors of vaccine response. The dichotomized dependent variables were poor response, which meant anti-HBs titer <l00 mIU/ mL, and fine response, which meant anti-HBs titer ≥l00 mIU/ mL. All variables in univariate analysis were incorporated into model fitting with multinomial variables converted into dummy variables. The predictors of response are shown in Table 2. Five variables, gender, age, prematurity, dosage of HepB, and mother being positive for both HBsAg and HBeAg, were found to be significant predictors of vaccine response. The strongest predictor was the dosage of HepB; infants who were vaccinated with 5 µg HepB-SCY were 4.26 times more likely to develop poor response than those vaccinated by 10 µg HepB-HPY. Age also had strong effect on response, with infants aged 13 to 18 months being 3.08 times more likely to develop worse response than those aged 7 to 12 months. Premature infants and infants whose mothers were positive for both HBsAg and HBeAg were more likely to develop poor response with odds ratio (OR) of 2.73 and 1.94, respectively. Notably, gender was also a predictor of vaccine response. Male infants were 1.39 times more likely to have lower response compared to female infants. In addition, BMI, birth weight, delivery mode, and mother who had received HBIG during pregnancy had no significant influence on the response when adjusted for potential confounding factors.
Logistic Regression Analysis on Predictors of Neonatal Response to HepB Vaccination.
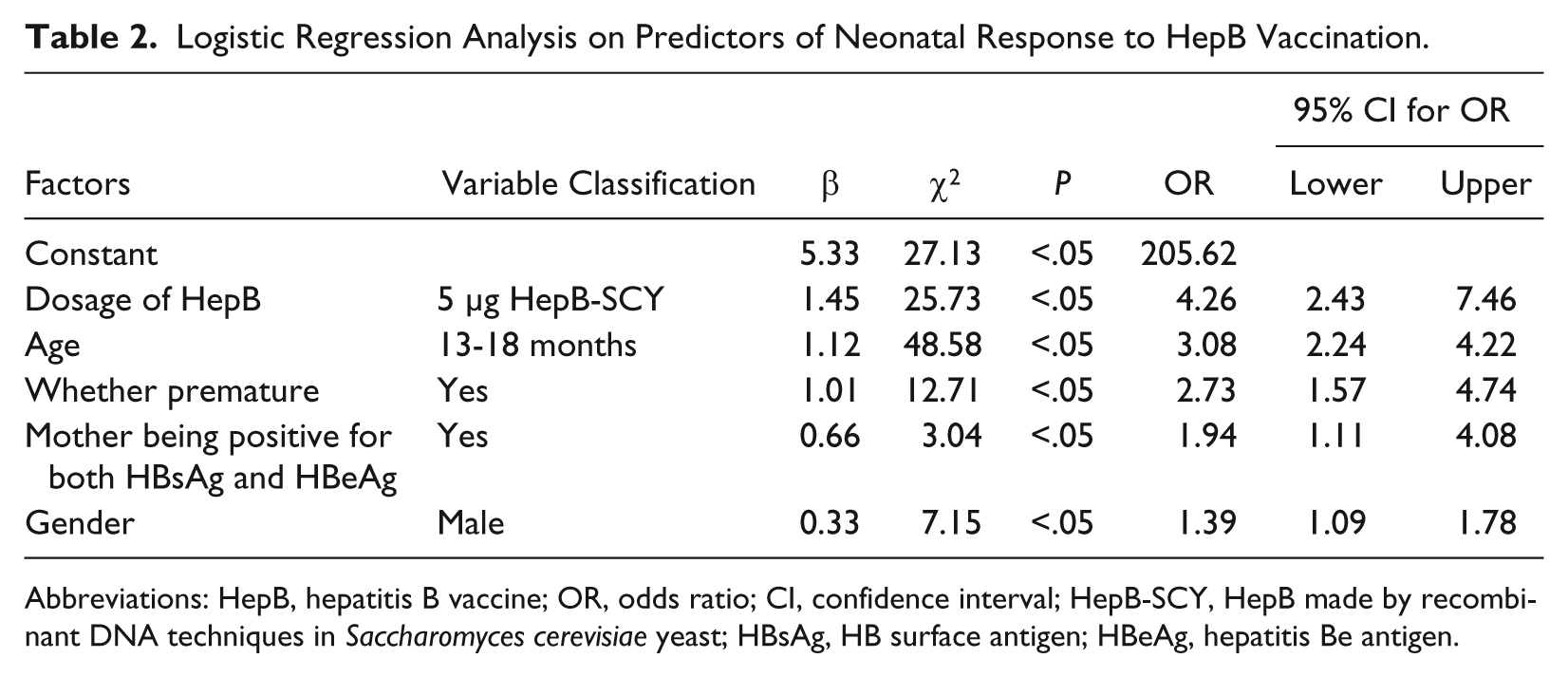
Abbreviations: HepB, hepatitis B vaccine; OR, odds ratio; CI, confidence interval; HepB-SCY, HepB made by recombinant DNA techniques in Saccharomyces cerevisiae yeast; HBsAg, HB surface antigen; HBeAg, hepatitis Be antigen.
Booster Immunization
Of the 344 subjects who did not meet the protective antibody titer (>100 mIU/mL) after primary immunization, 262 (76.16%) were successfully recruited for booster vaccination. At the baseline of booster, essential characteristics including gender, age, and premature status were compared, and no statistically significant difference was found (Pearson χ2 = .01, P = .94; Pearson χ2 = .07, P = .79; Pearson χ2 = .29, P = .59, respectively). Of these, 234 infants (126 males vs 108 females) and 214 infants (119 males vs 95 females) were evaluated for anti-HBs titer at the first and the seventh month post-booster, respectively.
For 112 infants (61 males vs 51 females) who were vaccinated with 5 µg HepB-SCY, the GMC post-first booster was 630.30 mIU/mL (95% CI = 613.47-647.13). The GMC of 106 infants (62 males vs 44 females) who had completed the full 3 boosters was 511.78 mIU/mL (95% CI = 498.72-524.84). The GMC of infants administered with 5 µg HepB-SCY between post-first booster and post-full booster did not have statistically significant difference (t = 2.03, P = .16; Table 3). In the group vaccinated by 10 µg HepB-HPY, the GMC of 108 infants (57 males vs 51 females) who had completed the full 3 boosters was 1359.95 mIU/mL (95% CI = 1344.96-1374.95), higher than the GMC of 122 infants (65 males vs 57 females) after the first booster, which was 1295.17 mIU/mL (95% CI = 1273.65-1316.69), and the difference did not reach statistical significance (t = 1.92, P = .17). The GMC of infants in the 10 µg HepB-HPY group was obviously higher than that of infants in the 5 µg HepB-SCY group, with statistically significant difference both post-first booster (t = −3.65, P < .05) and post-third booster (t = −5.31, P < .05; Table 3).
Anti-HBs Titers of Poor Response Infants After Receiving Booster Immunization.
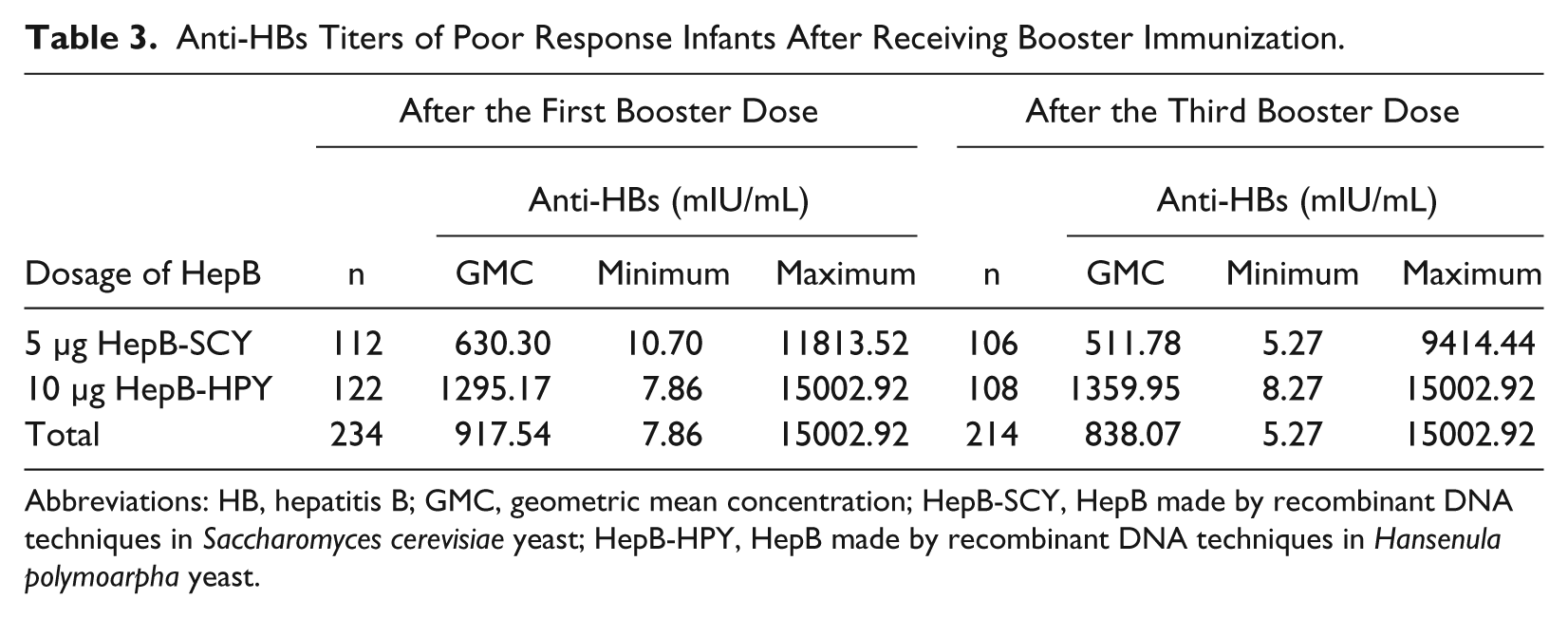
Abbreviations: HB, hepatitis B; GMC, geometric mean concentration; HepB-SCY, HepB made by recombinant DNA techniques in Saccharomyces cerevisiae yeast; HepB-HPY, HepB made by recombinant DNA techniques in Hansenula polymoarpha yeast.
With regard to the seroprotective rate (anti-HBs > 100 mIU/mL) of the group receiving 5 µg HepB-SCY, 91.51% (97/106) became seroprotected after the full course of booster, higher than the seroprotective rate after the first booster, which was 89.29% (100/112), but the difference was not statistically significant (χ2 = 0.50, P = .48). For 10 µg HepB-HPY group infants, 97.22% (105/108) developed anti-HBs seroprotection after the full booster, higher than the seroprotective rate after the first booster, which was 90.99% (111/122), and the difference was also not statistically significant (χ2 = 3.90, P = .09). After the first booster dose, the proportion of seroprotection in the group receiving 10 µg HepB-HPY was higher than that of the 5 µg HepB-SCY group (90.99% vs 89.29%), but the difference was not statistically significant (χ2 = 0.19, P = .66). Using the threshold for high seroprotection of ≥1000 mIU/mL, the result showed a notably higher seroprotected rate for the 10 µg HepB-HPY group (61.48%) as compared with the 5 µg HepB-SCY group (39.29%), and with statistically significant difference observed (χ2 = 11.50, P < .05). After the full 3 doses of booster, 97.22% (105/108) in 10 µg HepB-HPY group and 91.51% (97/106) in the 5 µg HepB-SCY group became seroprotected, and the difference was not statistically significant (Fisher’s χ2 = 3.30, P = .07). It was worth noting that the proportion of anti-HBs titers higher than 1000 mIU/mL for the 10 µg HepB-HPY group (61.11%) was still higher than that of the 5 µg HepB-SCY group (25.47%), and with statistically significant difference observed (χ2 = 27.65, P < .05; see Table 4).
Distribution of Anti-HBs Level of Poor Response Infants After Receiving Booster Vaccination.
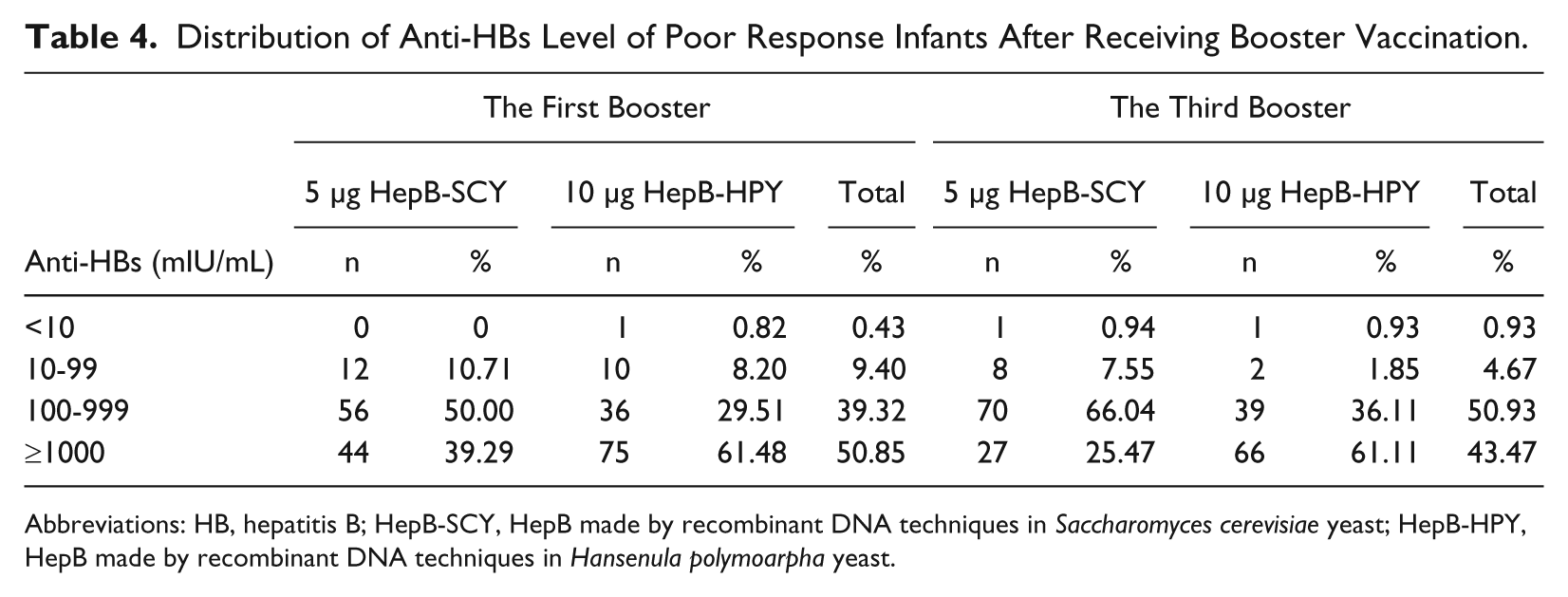
Abbreviations: HB, hepatitis B; HepB-SCY, HepB made by recombinant DNA techniques in Saccharomyces cerevisiae yeast; HepB-HPY, HepB made by recombinant DNA techniques in Hansenula polymoarpha yeast.
Discussion
Since the introduction of active immunoprophylaxis against HBV infection, HepB vaccination for neonates has been proven to be the most effective strategy for prevention and control of HB. However, the phenomenon of nonresponse and low response is still a problem. Infants may not be able to surpass a protective level of anti-HBs following a full course of vaccination. Due to the difficulty of blood collection for infants, study on nonresponse and low response to HepB in infants is comparatively rare.19,20 We observed that 1.86% of infants were nonresponders and 15.14% were low responders. Our results were similar to another study in south China, which reported 1.72% and 15.17%, respectively. 19
The reasons why some infants do not respond adequately to the primary vaccination against HepB are complex. Our study showed that the dosage of HepB, age, gender, prematurity, and mother being positive for both HBsAg and HBeAg were the predictors of poor response. Infants vaccinated with 5 µg HepB-SCY were more likely to develop poor response than those vaccinated with 10 µg HepB-HPY, which indicated dosage of vaccines had an important impact. 21 Poor response in infants aged 7 to 12 months was lower than that of infants aged 13 to 18 months, which suggested younger infants could have better response compared with older ones. Analogous studies also found anti-HBs of infants finishing primary immunization declined relatively fast 1 to 2 years after birth, especially for those whose mothers were HBsAg carriers.22,23 Similar with observations from others, our results showed that the response of premature infants was inferior to full-term infants. 19 Compared to the full-term infants, the specific and nonspecific immune function of premature infant is immature, and its response to HepB is also weaker than that of full-term infants. Moreover, whether the mother is an active carrier also affected the infant’s response to HepB.23,24 Our study indicated that infants whose mothers were positive for both HBsAg and HBeAg were 1.94 times more likely to develop poor response than their controls, so the chance of immunization failure increased correspondingly. It was thought that perinatal or early postnatal HBV transmission was more likely for those infants born to HBsAg-carrier mothers with concurrent HBeAg, which therefore would affect the response to HepB. However, immunized infants born to mothers infected with HBV were 3.50 times less likely to become infected with HBV. 25 Gender was also a predictor of response, male infants were more likely to have inferior response compared to female infants. A study in German also showed that the anti-HBs of males were lower than that of females. 11 Contrary to previous reports,19,26 we did not observe any statistical correlation between birth weight and vaccine response.
In our study, we adopted different types and dosages of HepB for booster immunization for documented nonresponding and low-responding infants. Overall, the difference between the GMC post-first booster and the GMC post-full booster program did not show statistical significance. Grouping results also showed the difference between the GMC after the first booster and the GMC after the full booster was not statistically significant, whether for the 5 µg HepB-SCY group or for the 10 µg HepB-HPY group, which suggested revaccination of 1 dose of 5 µg HepB-SCY or 1 dose of 10 µg HepB-HPY would develop sufficient seroprotection for nonresponse and low-response infants. On the other hand, the GMC of the 10 µg HepB-HPY group was obviously higher than that of the 5 µg HepB-SCY group whether after the first booster or after the full booster (P < .05), which indicated the immunogenicity of 10 µg HepB-HPY was better than that of 5 µg HepB-SCY.
Revaccination for nonresponders and low responders in this study not only acquired sufficient anti-HBs titer but also achieved satisfactory seroconversion. The seroprotection of the 2 HepB groups after the full booster was higher than the seroprotection after the first booster, and without statistically significant difference observed. The findings further demonstrated revaccination of 1 dose of 5 µg HepB-SCY or 1 dose of 10 µg HepB-HPY would achieve ideal seroconversion for nonresponse and low-response infants. It was worth noting that the proportion of anti-HBs titer higher than 1000 mIU/mL of the 10 µg HepB-HPY group was obviously higher than that of the 5 µg HepB-SCY group whether after the first booster or after the full booster (P < .05), which indicated that the capability of high-level seroconversion of 10 µg HepB-HPY was better than that of 5 µg HepB-SCY.
We can therefore conclude that HepB revaccination for poor responding infants can ultimately develop satisfactory anti-HBs seroconversion and GMC according to 0, 1, and 6 months schedule. Whether evaluating from anti-HBs seroconversion or from GMC, 1 dose of booster with 10 µg HepB-HPY or 5 µg HepB-SCY can both produce satisfactory response and probably activate the immunologic memory of these infants. Compared with 5 µg HepB-SCY, 10 µg HepB-HPY can achieve the higher GMC and more superior seroprotection (anti-HBs > 1000 mIU/mL). It could therefore be advisable to administer an extra dose of 10 µg HepB-HPY to documented nonresponse and low-response infants. Despite the booster, immunization can make most of low-response infants produce seroprotection, and the GMC obtained in the short term has no obvious difference with that of good responders; however, the persistence is inconclusive and needs further study.
Footnotes
Acknowledgements
The skillful assistance and administrative support of Dr Cao Weizhong, Dr Pan Yinjun, and Dr Qian Jie (all at the study site in Shanghai), which ensure timely study conduct and high-quality data, is warmly acknowledged. We thank Prof Paul Chan (Chinese University of Hong Kong) for critical review of the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from the National Key Science and Technology Projects in “Eleventh Five-Year Plan” (No. 2008ZX10002-001), the Science and Research Project of Shanghai Municipal Health Bureau (No. 20114072), and the Constructing Program of Shanghai Municipal Public Health Key Discipline (No. 12GWZX0101).