
Abstract
Intensifying detection of tuberculosis (TB) symptomatic patients is a priority for Cambodia’s National Tuberculosis Program, in a country where two-thirds of the population has latent TB infection. In 2005, the National Tuberculosis Program initiated a public-private mix (PPM) collaborative program with external and local stakeholders to identify and refer persons with TB symptoms from private sector pharmacies to public sector clinics for diagnosis and treatment. This qualitative study conducted in-depth interviews with organizational stakeholders to assess their perceptions of PPM program collaboration and its sustainability in the long term. Results showed that stakeholders perceived that collaboration and efficient management had contributed to positive program performance. However, stakeholders expressed anxiety over program sustainability should external resources be reduced. Recent developments in pharmacy undergraduate education and recognition of pharmacy providers’ contribution to public health interventions may challenge PPM stakeholders to shift the paradigm from dependence on external agencies to confidence in local expertise and infrastructure.
Introduction
Cambodia, 1 of 4 countries in the World Health Organization Western Pacific Region with high tuberculosis (TB) burden, has succeeded in reducing TB prevalence by 45% over the past decade. 1 However, two-thirds of its population of 14 million has latent TB infection, and the incidence rate (424/100 000) remains high compared with the regional rate of 92/100 000. 1 The case detection rate (CDR) of 64% has increased marginally over years 2008-2010 but remains low compared with the regional CDR of 81%. 1 Recent modeling has suggested that a CDR of more than 70% may not be sufficient to maintain a downward trend in TB incidence rates over the long term without complementary interventions. 2 Cambodia, therefore, is focused on intensifying case detection through engagement with private sector providers, including, but not limited to, registered private sector pharmacies.
Cambodia’s National Center for Tuberculosis and Leprosy Control (CENAT) implements a DOTS (directly observed treatment, short course) program nationwide through public sector primary health care centers. DOTS is an internationally recognized, evidence-based strategy for the diagnosis and directly observed treatment of TB patients. The DOTS program in Cambodia maintains a treatment success rate of 94% 1 and provides free-of-charge services to all citizens. However, more than 70% of Cambodia’s population visits private health care providers, including pharmacies, as their first point of contact with the health care system. 3 Facilitating patient access to public sector DOTS services, via referral from private sector pharmacies, provided the rationale for CENAT’s decision to collaborate with private pharmacies in a public-private mix (PPM-DOTS) partnership. Evidence from studies undertaken in high-burden countries indicate that private sector pharmacies are ready, willing, and able to participate in public health programs, including TB programs, and have the potential to deliver evidence-based quality care while contributing to program targets.4 -7 The recent decade has seen several PPM interventions formally engaging private sector pharmacies in TB control.8 -10
In 2005, CENAT initiated a PPM-DOTS Referral Program, in collaboration with local and external partners, to increase detection of TB symptomatic patients through pharmacy-initiated referral. By 2012, 1200 registered pharmacies nationwide provided referral services, including more than 350 of 600 private pharmacies in the capital city, Phnom Penh. 11 It is reported that approximately 19% of TB symptomatic patients referred through referral program providers, including pharmacies, are diagnosed with TB (Khim TB, National Center for Tuberculosis and Lung Disease, Phnom Penh, personal communication, January 23, 2013). This partnership model exemplifies the potential of pharmacy-based contributions to public health goals in communicable diseases.
The aim of this qualitative study was to investigate perceptions of PPM-DOTS stakeholder organizations in relation to program participation and sustainability.
Methods
Study Design
A qualitative study comprising in-depth interviews with representatives of program stakeholder organizations was conducted in Phnom Penh, Cambodia. The National Ethics Committee for Health Research, Cambodia, and the Human Research Ethics Committee, University of Sydney, approved study protocols prior to the study proceeding in January 2011.
Study Setting
The PPM-DOTS Referral Program was implemented by CENAT in collaboration with Municipal and Provincial Health Departments, global nonprofit organizations (PATH 2005-2011; Family Health International 2011-2012) and the Pharmacists Association of Cambodia—the organization representing the interests of the pharmacy profession. Additional technical assistance to the program was provided through the World Health Organization’s Cambodia office. The referral program, which commenced as a 5-year project, is a collaboration of 7 organizations, each with between 1 and 3 representatives contributing funding and/or expertise to the management, implementation, and coordination of the program. The pharmacy-based providers of referral services complied with regulations, subsequently made law, prohibiting the sale of anti-TB medications in the private sector. This strategy is designed to contain the rise of multidrug-resistant TB in Cambodia. Pharmacy owners and/or staff, many with minimal pharmacy-related education, were trained to assess, counsel, and refer patients with TB-like symptoms. Pharmacies received no fee for service from the program or patients.
Study Participants and Processes
Interviewees were representatives of collaborating program organizations and were purposively selected based on their strategic, decision-making, and implementation roles within the program. Interviews were conducted in Phnom Penh, at times and venues suggested by representatives, across January 2011 and January 2012. Representatives received a Participant Information Sheet, in Khmer, prepared by a commercial translation company prior to providing signed consent and commencing the interview. Participant interviews were audiotaped, with signed interviewee consent. A semistructured interview guide was informed by the author CAB’s reading of the literature relating to PPM interventions in high-burden countries and discussion with the Stop TB Partnership representative in Phnom Penh. Interviewees were allowed open-ended comment on set topics relating to their roles in the program and its sustainability in the long term. Author CAB conducted 9 interviews in English. Three interviews were conducted in Khmer by a Ministry of Health official. Translation of audiotapes from Khmer to English, with verification by a second interpreter, was undertaken by a commercial translation company. All tapes were transcribed by author CAB. Stored audiotapes and transcripts were deidentified.
Data Analysis
Authors CAB and BS independently analyzed data using the Framework Approach.12,13 This approach comprised an open-minded reading of all transcripts in which emergent themes from the set topic data were subsequently indexed, charted, mapped, and interpreted by incorporating differences and commonalities. This systematic approach permits independent analysis.
Results
In all, 12 representatives were interviewed. Table 1 shows deidentified interviewee affiliations based on the interviewee’s full-time employment. Several interviewees worked part-time and/or voluntarily in other program organizations. All organizations were strongly supportive of the program and reported that the program had made good progress since inception, making positive contributions to case detection. Representatives stated that further improvements could be made. Two major themes emerged from the data: “roles and relationships” and “shifting the paradigm.”
Interviewee Affiliations and Organizational Roles in the PPM Referral Program.
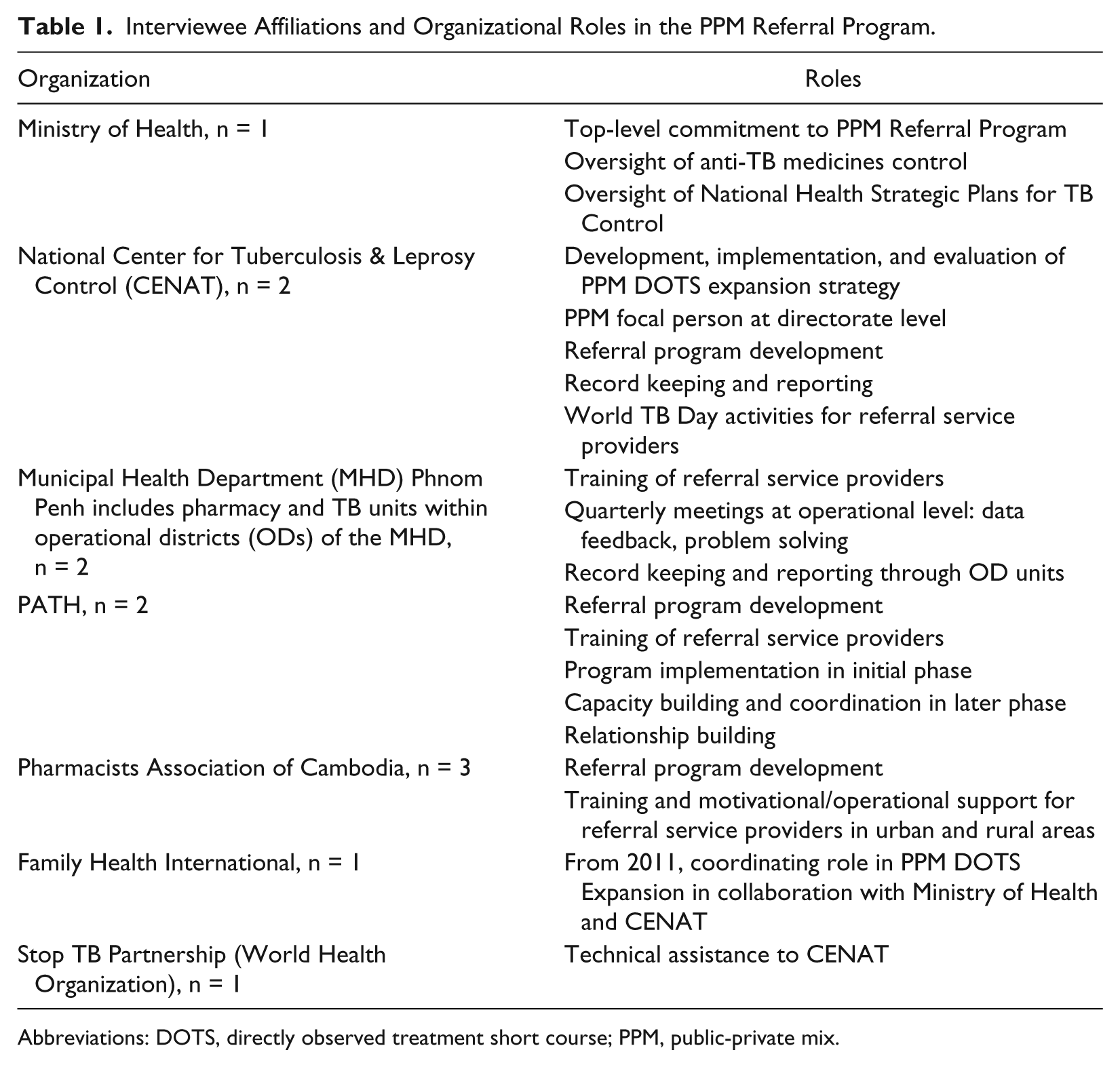
Abbreviations: DOTS, directly observed treatment short course; PPM, public-private mix.
Roles and Relationships
Representatives described clearly defined and allocated roles undertaken by their organizations, as shown in Table 1, and expressed confidence in the PPM-DOTS Referral Program. Representatives believed that strong management structures, including quarterly stakeholder meetings at the operational level to access technical advice, had provided opportunities for shared problem solving and data feedback. Several interviewees referred to successful collaboration as a particular strength of the program:
We meet together, public and private sector, raise the problem and solve together. (R8)
In addition to reported strong collaborative relationships and strong government commitment to the program, interviewees attributed progress to the accessibility and patronage of the large network of legal private sector pharmacies in Cambodia:
In Cambodia people mostly go to pharmacies, so that’s the reason . . . we rightly focus on pharmacies in the beginning. (R5)
Some representatives believed that their employment in both public and private sectors had contributed to a history of good working relationships between government and private sector pharmacies. They perceived this was advantageous for program implementation:
Pharmacy, cabinet [practitioner dispensary] and laboratory, we are agreed to enter the one system [to refer to] the public facility. (R6)
However, others recognized that allocating work time to both sectors was challenging and could affect program operation. This was perceived as a particular challenge for the program.
It affects the working time of the government and sometimes it’s difficult to arrange the time-frame for implementing PPM activities. (R7)
Several stakeholders spoke of Cambodia’s learning-by-doing philosophy—its readiness to regularly review and adapt policy. Interviewees cited the 2011 introduction of text messaging between pharmacies and clinics to monitor referrals and the amendment of referral criteria to detect TB symptomatic persons earlier in the progression of their illness.
Several interviewees commented on the crucial role of the leading global stakeholder, PATH, in program implementation, knowledge transfer, and capacity building with local nongovernment organizations. Minimizing the loss of accrued program benefits following PATH’s anticipated withdrawal at the end of the project period was seen as urgent by external stakeholders in the program.
Several representatives recognized that PPM interventions provided strategic opportunities for external partner agencies to gain experience in PPM management, subsequently transferable to other settings. Similarly, they recognized that local partners gained program management skills, relevant not only to TB control but also to other public health issues. Several representatives cited earlier PPM programs in reproductive, maternal, and child health implemented through private sector pharmacies and the potential for similar consumer-focused programs in malaria control.
Shifting the Paradigm
Despite efficient, collaborative management, all representatives expressed anxiety over program sustainability. Local organizations recognized that through collaborative relationships with global agencies and their direct involvement with program implementation, positive results had been achieved, but doubts were expressed about maintaining and consolidating program performance beyond the project period. Representatives from local stakeholder organizations believed strongly that any reduced funding and management input from global agencies would signal the collapse of the program. However, whereas external stakeholders focused on shifting the paradigm from one of dependence on external funding and support to a more locally driven environment, local organizations were not optimistic:
We are completely dependent on external funding for any activity, even for running our own organisation. (R7)
Expanding the program to involve more local partners, including informal (unregulated) health care providers, was seen as essential by external partners. However, it was suggested by local stakeholders that involvement of informal providers in the PPM program could raise regulatory concerns for government and program donors. External organizations recognized that engaging with informal health care providers could increase access to TB care for many Cambodians. However, they reported that because government policy did not legally recognize informal providers, the decision to work collaboratively with such providers was a complex issue for externally funded agencies.
Should we work with them [informal providers] when they don’t legally exist? If you don’t work with them, you’re losing a lot of opportunities. (R3)
Some representatives believed that increasing participation of local nonprofit organizations in the program could impose strains on existing human and financial resources. One representative stated that volunteer staff had provided training and advocacy workshops in Phnom Penh with minimal recompense, and extending program training and advocacy activities to more organizations, particularly in provincial areas, where greater costs were incurred, was extremely difficult.
Concern was also expressed over pending government legislation to regulate foreign and domestic nonprofit and civil society organizations, with uncertain implications for those agencies and consequently the sustainability of the program.
Discussion
This study is one of few studies looking at pharmacy-based interventions in TB—a disease requiring strategic public health initiatives for containment.8-10 It focused on stakeholder perceptions of a PPM-DOTS intervention as a strategic collaboration rather than as an evaluation of program outcomes.
The Cambodian Ministry of Health was an early adopter of PPM-DOTS strategies, incorporating engagement with the private sector into its National Health Strategic Plans for TB Control 2001-2005 and 2006-2011.14,15 Several respondents referred to a spirit of learning by doing among stakeholders in both public and private sectors, uniting them in their commitment to the postconflict rebuilding of Cambodia’s health care infrastructure. The National TB Program, a major player in the renewal of the health system, has significant experience in building relationships and working collaboratively. 16 These qualities may have contributed to successful stakeholder collaboration in the referral program and have been shown to be factors integral to successful PPM-DOTS implementation elsewhere. 17
Similarly, stakeholders praised the role of pharmacy referral service providers and their major contribution to successful program implementation. In a study of provider perceptions of the referral program, the shared goal of restoring access to health care for all Cambodians was highlighted by providers as a major motivating factor in their commitment to the program. 18 The experience of shared goals and collaborative relationships in Cambodia have been strengths of the program—strengths not always realized in PPM-DOTS interventions in other national contexts.19,20
Despite strong foundations established during the 5-year duration of the referral program, stakeholders spoke with considerable anxiety regarding program sustainability, including local capacity building. Building capacity within the public sector is a major challenge for government and external funding agencies in Cambodia, where low-paid public sector staff commit to working concurrently in the private sector to supplement incomes. 21 Challenges related to developing and strengthening existing resources in Cambodia were highlighted in a study focusing on referral systems for injury patients. 22 Study authors suggested that strengthening the system via its component parts may be a way forward. Strategies for strengthening the TB referral system may benefit from this approach. As pharmacy has played a successful role in public health initiatives in Cambodia, it may be timely for the profession to develop a vision for defining wider professional roles. Given that the undergraduate curriculum 2012-2013 includes clinical sciences, pharmacy practice, and social and behavioral sciences, graduates will be well prepared to contribute to national public health programs. 23 Studies elsewhere have recognized that expanding the role of pharmacists to include both public and private sector involvement has the potential to contribute significantly to public health initiatives, particularly in newly developing health systems. 24 PPM Referral Program stakeholders in Cambodia are now well placed to capitalize on the knowledge and expertise gained during the program to reduce dependence on external agencies. A network of experienced private and public sector referral providers now exists for this purpose. Experience with PPM-DOTS interventions elsewhere has shown that overstay by external agencies may be counterproductive, leading to increased dependence and lack of confidence among local program partners. 19 However, although external aid to Cambodia continues to be delivered through project-based collaborations with a multiplicity of global and local stakeholders, mainstreaming project knowledge and expertise may continue to be a challenge for CENAT and PPM partners. 25
Expanding the PPM model to include informal (unregistered) health care providers was considered essential by global stakeholder organizations but regarded as questionable by some local partners. Concerns were raised about prejudicing successful acquisition of external funding by inclusion of unregistered providers in government-promoted projects and programs. In the context of government efforts to improve regulation of health care providers, involving informal providers in the PPM model may deter inclusion of other registered providers in the program, as found in other studies. 21 Expanding the program to include informal providers may be a strategy whose time is yet to come. 26
Stakeholder anxiety over program sustainability was further compounded by uncertainty over pending government regulation of foreign and domestic nonprofit and civil society organizations. However, draft legislation submitted to nonprofit agencies for comment late 2012 is undergoing further redrafting. 27
There are limitations in this study that should be considered in the context of external validity. Travel and data collection activities were constrained to the capital city, Phnom Penh, because of lack of funding. Consequently, it was not possible to interview program stakeholders located in provinces outside the metropolitan area. TB patients are prime stakeholders in any health care intervention. At the time of this study, TB patients remained unrepresented at the organizational level. Findings from future studies on patient perceptions of PPM-DOTS referral services may complement existing studies on this intervention.
Conclusion
Stakeholders perceived that the PPM-DOTS Referral Program was improving TB CDRs in Cambodia through strong management and the commitment of all stakeholder organizations to the program and its goals. Consolidating and sustaining the impact of private sector pharmacies in meeting public health goals may now challenge PPM-DOTS stakeholders to shift the paradigm from one of dependence on external agencies to one of increasing confidence and investment in local expertise and infrastructure.
Footnotes
Acknowledgements
The authors wish to thank the directors and staff at the following organizations for their cooperation: National Center for Tuberculosis and Leprosy Control (CENAT), Ministry of Health, Cambodia; Municipal Health Department, Phnom Penh; PATH; Family Health International; the Pharmacists Association of Cambodia; and Stop TB Partnership Cambodia Office. We also acknowledge the support of the National Ethics Committee for Health Research, Cambodia, and the Ethics Committee, Research Office, University of Sydney, Australia.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Author CAB received a travel grant from the University of Sydney to undertake this study.