
Abstract
This study aimed to explore the relationship between psychological distress and degree of functional independence among elderly adults following the Great East Japan Earthquake. Participants were 20 282 adults aged 65 and older who lived in the Great East Japan Earthquake evacuation zone specified by the government on March 31, 2011. This study is a part of a detailed survey on mental health and lifestyle, the Fukushima Health Management Survey, which was conducted in 2012. Psychological distress was assessed using the Kessler 6 scale. Functional independence in different daily activities was assessed by asking participants whether they could independently perform activities: eating, dressing, toileting, and shopping. According to the multiple logistic regression analysis, psychological distress was significantly associated with independence in all models: without adjustment (Model 1), adjusting for demographic characteristics (Model 2), and adjusting for demographic characteristics and disaster-related factors (Model 3), with an adjusted odds ratio of 2.32 (95% confidence interval = 1.97-2.73). High psychological distress was associated with low functional independence, after controlling for demographic characteristics and disaster-related factors. Thus, using psychological distress as the dependent variable, we examined the relationship between low functional independence and psychological distress among elderly adults who were evacuated.
Introduction
On March 11, 2011, the Great East Japan Earthquake hit Japan with a magnitude of 9.0 on the Richter scale, and the subsequent tsunami initiated a nuclear accident at the Tokyo Electric Power Company’s Fukushima Daiichi Nuclear Power Plant (NPP). This complex disaster caused a radiation hazard in Fukushima Prefecture, 1 and thus, the government designated an evacuation zone within the area. More than 160 000 residents were forced to evacuate. According to the reports from the NPP accident in Chernobyl in 1986, major health problems experienced by affected residents include psychological distress. 2 The evacuees in Fukushima experienced disaster damage, traumatic stress, and lifestyle change. Consequently, they suffered from psychological distress due to stressors that arose from the evacuation, including perceived risk of radiation effects on health. 3
Appropriate health interventions need to be developed for elderly adults after a disaster. Natural disasters have a greater impact on psychological health among elderly adults than their younger counterparts at the time of disaster.4,5 Furthermore, within the elderly population, functional independence varies from those who live independently and provide care for others, to those who need support typically due to dementia or a bedridden state. To our knowledge, previous research has only focused on the relationship between psychological well-being and its related factors among the general population; thus, the relationship between functional independence and psychological well-being among the elderly population warrants further investigation.
Psychological Distress and Functional Independence
Presently, subclinical depression, or minor depression, is common among community-dwelling elderly adults, although there is a wide range of reported prevalence rates depending on sample characteristics and measurement methods used. 6 Daily functioning is related to mental health among elderly adults,7,8 and in some longitudinal research, depressive status predicts further functional decline among community-dwelling elderly adults.9,10 Functional assessment, which is now incorporated in the Japanese national elderly care program, 11 could be an avenue for assessing further needs related to psychological health among elderly adults. Such assessment is crucial due to the barriers that elderly adults face in seeking psychological help in Japan. 12 Furthermore, in times of disasters, psychological distress commonly increases among elderly adults, partially because of a relative disadvantage in socioeconomic status.13 -15 Moreover, in times of disaster, psychological and functional factors are associated with resilience among elderly adults. 16 Thus, to promote resilience in elderly adults, appropriate public health interventions that address both psychological and functional aspects after a complex disaster are warranted. Since our survey focused on the support for mental health based on the experience in Chernobyl, we examined the degree of functional independence, which could be easily measured, to explain the psychological distress.
The aim of this study was to explore the relationship between psychological distress and degree of functional independence among elderly adults after the Great East Japan Earthquake.
Methods
Study Design
This study is a part of a detailed survey on mental health and lifestyle, the Fukushima Health Management Survey, conducted in 2012, within a year after the accident. We examined the cross-sectional data of elderly adults aged 65 years and older as of March 11, 2011.17,18
Setting
The Fukushima Health Management Survey was implemented to assess the health and lifestyle of those evacuated during the Fukushima Daiichi NPP accident. Details of the protocol and data set used in the present study have been described elsewhere.17-25 The survey was a self-administered questionnaire, and the target population included adults and children (aged 15 years and older) who were registered as residents within the government-designated evacuation zone (n = 210 189). The questionnaires were mailed to the target population beginning January 18, 2012, and they were asked to return them within approximately 2 weeks. The responses that arrived until October 31, 2012, were analyzed and the others were excluded. The evacuation zone designated by the government includes Hirono-machi, Naraha-machi, Tomioka-machi, Kawauchi-mura, Okuma-machi, Futaba-machi, Namie-machi, Katsurao-mura, Iitate-mura, Minamisoma City, Tamura City, and a part of Date City.
Participants
The target population of this study was the elderly-adult cohort, those aged 65 and older as of April 1, 2011 (n = 53 220), and among them 25 890 responded to the Mental Health and Lifestyle Survey between January 30 and October 31, 2012. Although it was a self-administered survey, caregivers were allowed to complete the survey as a proxy for those who were not able to do so themselves, because of existing dementia, or living in nursing homes.
Measurements
Psychological Distress
The outcome variable was psychological distress, measured by the Kessler 6 (K6) scale. 26 This tool uses a 5-point Likert-type scale to assess symptoms of mental illness during the past 30 days. Higher scores indicate worse mental health status (total range = 0-24). The Japanese version of the K6, which was used in this study, has been validated. 27 Based on a previous research, we defined those who scored between 13 and 24 as “psychologically distressed” and those who scored between 0 and 12 as “others.”26,28
Functional Independence
The explanatory variable was functional independence. Respondents reported their ability to perform daily activities, including eating, dressing, toileting, and shopping for daily necessities, with a binary response option: 1 = I can do it by myself; 2 = I cannot do it by myself. Specifically, we asked participants to indicate if they could “eat meals without assistance (does not include meal preparation),” “get dressed without assistance,” “go to the toilet without assistance,” and “go shopping for daily necessities without assistance.” We defined participants with high independence as those who reported, “I can do it by myself” to all 4 items and low independence as those who indicated “I cannot do by myself” to any of the 4 items.
Basic Characteristics and Disaster-Related Factors
To control for confounding variables, we measured general characteristics and disaster-related factors. General characteristics included gender, age, educational attainment, history of mental illness, and change in work. Disaster-related factors include residence place (Fukushima Prefecture or other), current living arrangement (shelter, temporary housing, rented house/apartment, relative’s home, own home, or other), the experience of the tsunami and NPP accident (Yes or No), and bereavement (loss of family or relatives; Yes or No). We defined the experience of the NPP accident as hearing any hydrogen explosion at the nuclear power plant accident to confirm the presence of trauma through a potentially life-threatening experience. Most of the variables were self-reported, and the incorrect response was anticipated because the respondents were elderly adults and we did not exclude people based on their cognitive functioning. In our analyses, we excluded data that were not self-reported (ie, surveys completed by a caregiver) in order to minimize inclusion of elderly adults with cognitive problems and the associated error and biases. This study was approved by the ethics committee of Fukushima Medical University (No. 1316).
Statistical Analysis
We included data from those who completed all 6 items of the K6. With respect to missing data in functional independence, as long as “I cannot do it by myself” was recorded on any item, the participant was categorized into low independence.
To explore the relationship between psychological distress and functional independence, we used a χ2 test to compare proportions of independence (low and high) between those with psychological distress and those without psychological distress. Subsequently, multiple logistic regression was used to examine the relationship between psychological distress and independence, controlling for potential confounding factors. Research has shown that psychological distress is associated with socioeconomic status, including age, gender, and disaster-related factors5,29 -31; thus, these variables were controlled for in the final model. As we assumed the variables were correlated, we introduced the variables stepwise to examine multicollinearity and robustness within the models. Logistic regression analyses were conducted on psychological distress and functional independence to calculate the odds ratio (OR) and 95% confidence interval (95% CI) for 3 models: without adjustment (Model 1), with adjustment for demographic characteristics (Model 2), and with adjustment for demographic characteristics and disaster-related factors (Model 3). Statistical procedures were performed using IBM SPSS Statistics version 21.0 (IBM, Corp, Armonk, NY).
Results
The number of elderly adults who responded to the survey was 25 890 (response rate = 48.6%). Because the outcome was psychological distress, a subjective evaluation, we excluded those who responded by proxy (n = 5608), resulting in 20 282 valid responses (valid response rate = 38.1%). We excluded an additional 3190 from this analysis due to missing values in the outcome variable of the K6, resulting in 17 092 for the analyses. Overall, the average score of K6 (SD) was 6.2 (5.9), and the number of those who were classified as having psychological distress (those who scored 13 or higher on the K6 scale) was 2566 (15.0%).
Table 1 shows the results of the bivariate analyses between psychological distress and the degree of independence, and other possible confounding factors. First, a significant association was found between psychological distress and low independence. Then, associations between psychological distress and the background characteristics were found, including gender, educational attainment, history of mental illness, and change in work. In terms of disaster-related factors, place of residence, living arrangement, experience of tsunami, experience of NPP accident, and bereavement were associated with psychological distress.
Relationships Between Psychological Distress and Degree of Independence, and Other Possible Confounding Factors (N = 17 092).
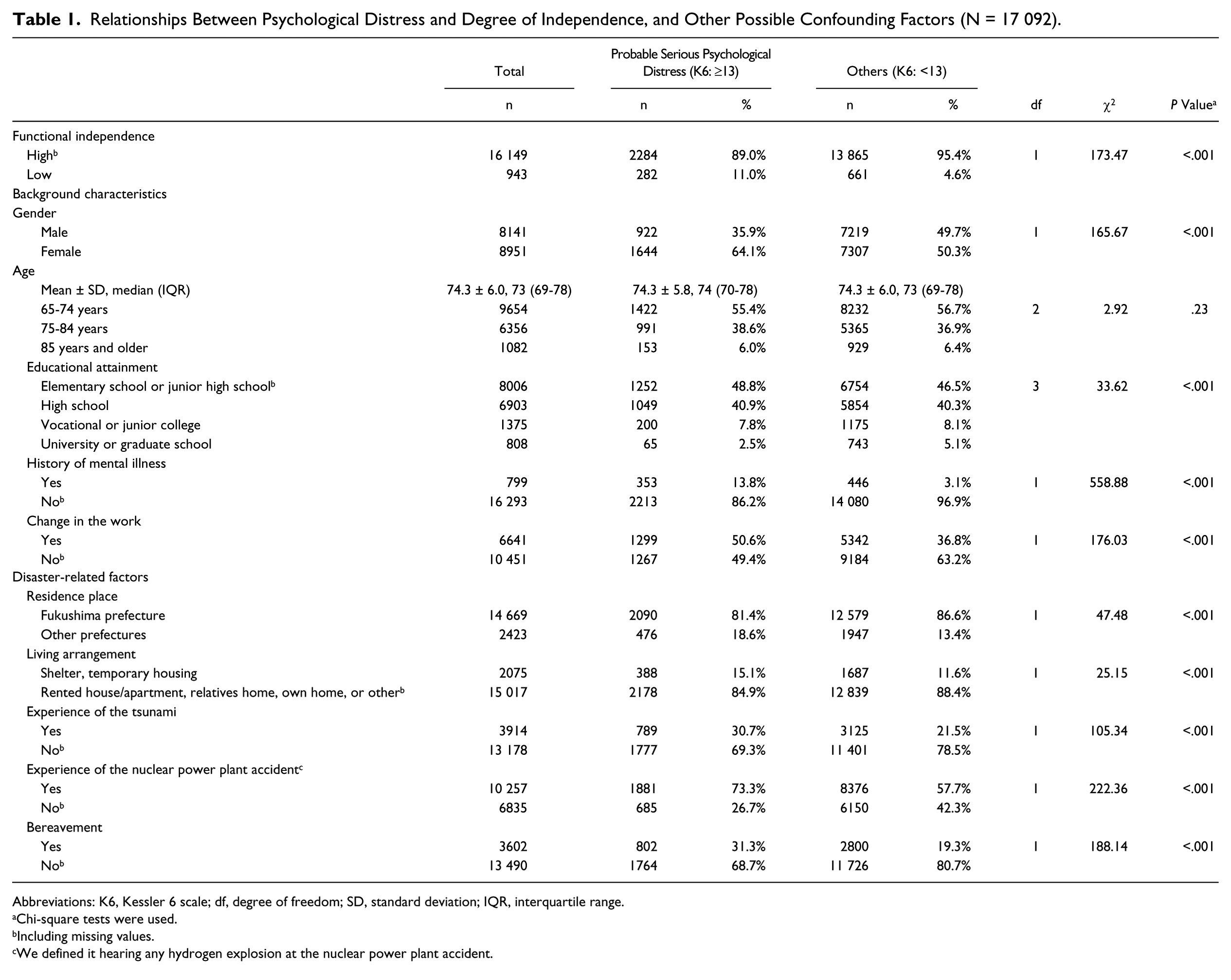
Abbreviations: K6, Kessler 6 scale; df, degree of freedom; SD, standard deviation; IQR, interquartile range.
Chi-square tests were used.
Including missing values.
We defined it hearing any hydrogen explosion at the nuclear power plant accident.
Table 2 presents the associations between psychological distress and functional independence by item. More people were found to have psychological distress among those with low independence than among those with high independence for eating, clothing, toileting, and shopping. Notably, 46.9% of those who had low independence for eating were psychologically distressed.
Relationships Between Psychological Distress and Functional Independence by Item (N = 17 092).
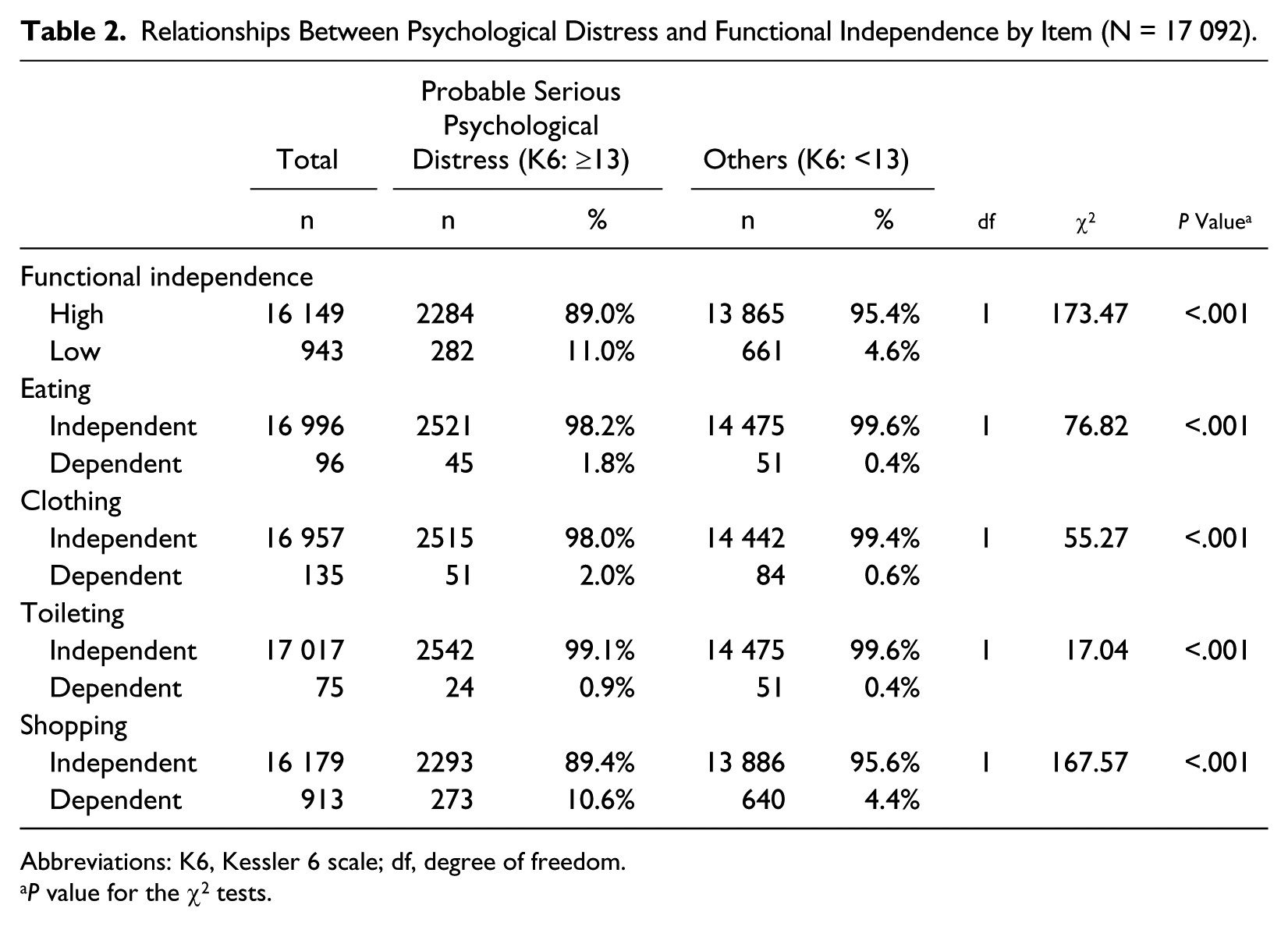
Abbreviations: K6, Kessler 6 scale; df, degree of freedom.
P value for the χ2 tests.
Table 3 shows the results of multiple logistic regression analyses. Low independence increased the likelihood of psychological distress by crude OR of 2.59 (95% CI = 2.24-3.00; Model 1), OR of 2.39 (95% CI = 2.03-2.81) adjusting for background characteristics (Model 2), and OR of 2.32 (95% CI = 1.97 to 2.73) adjusting for background characteristics and disaster-related factors (Model 3).
Relationships Between Degree of Independence and Probable Serious Psychological Distress (K6 ≥ 13) (Multiple Logistic Regression Analysis; N = 17 092).
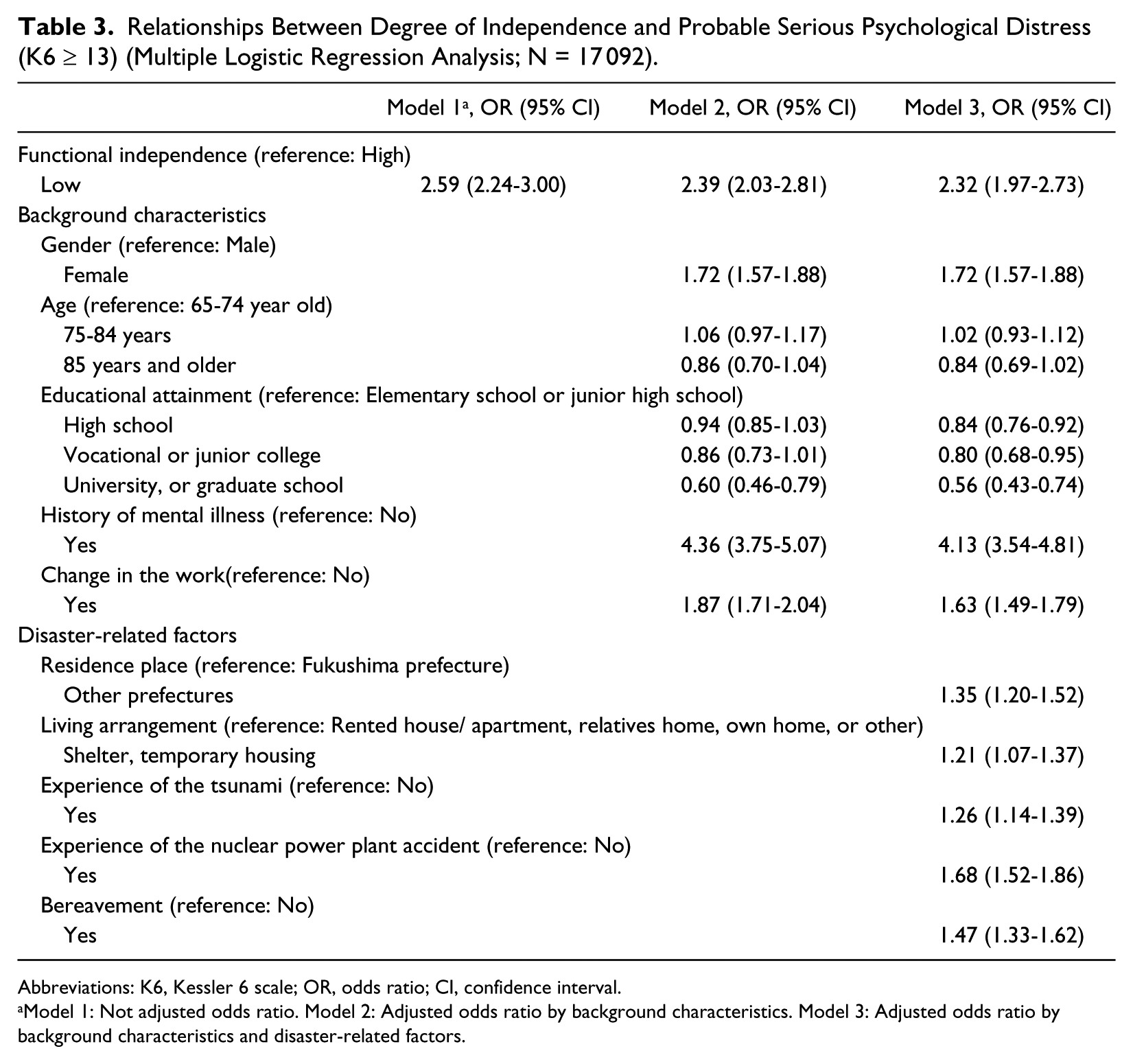
Abbreviations: K6, Kessler 6 scale; OR, odds ratio; CI, confidence interval.
Model 1: Not adjusted odds ratio. Model 2: Adjusted odds ratio by background characteristics. Model 3: Adjusted odds ratio by background characteristics and disaster-related factors.
Discussion
Psychological distress was associated with low functional independence among elderly adults who were evacuated after the Great East Japan Earthquake and Fukushima NPP accident 10 to 19 months after the disaster. This association remained after controlling for background characteristics and disaster-related factors. These findings suggest that priority should be given to low-functioning elderly adults in providing psychological care after a disaster.
In general, it is well known that elderly people, even under normal conditions, are more likely to be in a depressive state than younger people, which often causes a decline in the activities of daily living (ADL) or independent living skills.8 -10 Both cross-sectional and longitudinal studies have revealed the association between low functional independence and psychiatric disorders. A cross-sectional study demonstrated that the prevalence of depression was significantly higher in individuals who were dependent for ADL or instrumental ADL compared with those who were not. 32 A 4-year prospective cohort study demonstrated that increasing levels of depressive symptoms were predictors of a greater decline in physical performance. 33 Iwasa et al examined a longitudinal relationship between a depressive status and functional decline among Japanese community-dwelling older adults, using a 12-year population-based prospective cohort study design. As a result, an independent relationship was found between a depressive status and a longitudinal change in functional capacity among community-dwelling older individuals, suggesting that depression is a reliable predictor of a decline in both basic ADL and higher-level competence in older adults. 13 Therefore, psychological distress could be associated with an increased risk of functional dependence and vice versa.
In reviewing previous disaster studies focusing on the psychological well-being of elderly adults, risk factors for psychological distress were examined using basic characteristics and disaster-related factors.5,29 -31 This study added the knowledge that psychological distress was associated with low functional independence, even after controlling for such known disaster-related risk factors. Elderly adults are reported to be more vulnerable4,5 and take longer to recover than their younger counterparts in times of disaster. 34 The population in this study was a very specific and unique population, that is, the elderly adults who used to reside within the evacuation zone. Generalizing these results to other populations should be done with caution; however, the relationships established between psychological distress and potential confounding factors, that is, demographic characteristics and disaster-related factors, were comparable to previous findings in disaster research, which helps corroborate our study’s validity. In the event of the Fukushima NPP accident, adaptation to new living environments may have increased psychological burden among elderly adults, especially those who are frail. Mortality rates among the institutionalized elderly were exceptionally high during the first 3 months after the NPP accident. 35 Indeed, relocation is associated with poor mental health among elderly who experience several natural disasters.36,37
Furthermore, loneliness predicts functional decline among elderly adults. 38 Although loneliness was not directly measured in this study, living outside of one’s home or outside of Fukushima may have been associated with psychological distress through loneliness. Further study of this association is recommended. Another explanation for our findings points to secondary stress, such as separation from family members, unclear compensation, and exposure to public stigma, experienced after the evacuation, as a large body of research shows that secondary stressors are associated with psychological distress during disasters. 39 While physical and cognitive decline are key sources of low functional independence, secondary stressors may influence elderly evacuees to live less active lives in temporary housing or other housing arrangements that require additional adjustment effort. This may have created a self-perpetuating cycle, whereby the frail elderly became even more inactive. Thus, mental health care for those with low functional independence may also be an effective preventive measure for increased frailty.
Nevertheless, the strength of the present study is that is is the first to examine the relationship between psychological distress and independence after controlling for known risk factors using a large sample of elderly adults who were evacuated after the NPP accident in Fukushima, and its potential limitations warrant consideration. First, it is possible that the reverse relationship exists due to the cross-sectional nature of the study design. For example, psychological distress may have influenced functional impairment, as history of mental illness was strongly associated with psychological distress, suggesting a poor psychological condition prior to the disaster. The analysis of longitudinal data in future research is recommended to explore the causal relationship between independence and psychological distress. Second, functional independence was broadly operationalized and did not distinguish between basic ADL, such as eating, dressing, and toileting, and instrumental ADL, such as shopping. We attempted to analyze the basic and instrumental ADL data separately. Finally, since we analyzed the data obtained from only the elderly people who completed the questionnaire themselves, the participants of our study are likely to be more independent. This should be considered when generalizing the results of the present study.
In conclusion, our findings demonstrate that psychological distress is associated with low functional independence, even after controlling for demographic characteristics and disaster-related factors. Thus, using psychological distress as the dependent variable in the analysis models, we examined the relationship between low functional independence and psychological distress among elderly adults who were evacuated.
Footnotes
Appendix
The Fukushima Health Management Survey Group: Masafumi Abe, Shunichi Yamashita, Kenji Kamiya, Koichi Tanigawa, Seiji Yasumura, Makoto Akashi, Kazunori Kodama, Kotaro Ozasa, Hirooki Yabe, Masaharu Maeda, Kenneth E. Nollet, Ohtsura Niwa, Akira Ohtsuru, Shiro Matsui, Shinichi Niwa, Mitsuaki Hosoya, Tetsuya Ohira, Yasuto Kunii, Shuntaro Itagaki, Tetsuya Shiga, Hajime Iwasa, Yuriko Suzuki, Yoko Nakayama, Senta Fujii, Hiroaki Satoh, Shigeatsu Hashimoto, Kanae Takese, Satomi Nakajima, Maho Momoi, Saori Goto, Hirofumi Mashiko, Misao Ohta, Aya Goto, Mitsuru Hisata, Norito Kawakami, Akiko Yagi, Yu-ichi Oiwaka, Yuka Ueda, Mayumi Harigane, Naoko Horikoshi, Yu-ya Kashiwazaki, and Go Takeda.
Acknowledgements
We thank the chairpersons, other expert committee members, advisors, and staff of the Fukushima Health Management Survey Group.
Authors’ Note
The findings and conclusions of this article are solely the responsibility of the authors and do not represent the official views of Fukushima Prefecture government.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by the National Health Fund for Children and Adults Affected by the Nuclear Incident.