
Abstract
The Fukushima nuclear power plant accident caused widespread radiation contamination. Mothers of young children were at risk of negative emotional and mental health consequences. Using data from 2 independent prefecture-wide surveys of pregnant women, we examined the associations of disaster-related stressors with both maternal self-confidence and depressive symptoms. Two postal surveys were conducted targeting women who registered their pregnancies in Fukushima Prefecture (n = 6686 in 2012 and n = 6423 in 2013). The proportions of mothers with lower self-confidence in child rearing and with depressive symptoms were 53% and 25% in 2012 and 55% and 24% in 2013, respectively. After adjusting for maternal and infant characteristics, evacuation and concern about radiation were significantly associated with depressive symptoms but not lower maternal confidence, although these 2 outcomes were significantly associated. Mothers in Fukushima showed resilience in parenting, whereas their experiences and concerns in the aftermath of nuclear disaster were associated with depressive symptoms.
Background
The Fukushima nuclear power plant accident occurred on the heels of the March 2011 Great East Japan earthquake and tsunami, causing radiation contamination across a broad geographic area. In the face of this major nuclear power plant (NPP) disaster, mothers of young children were identified as one of the groups at greatest risk of negative emotional and mental health consequences. 1 In addition to the forced evacuation of the 20-km area, there was also a large self-evacuation outside the designated evacuation zones. 2 One year after the disaster, the proportion of the Fukushima population <5 years old was 8% lower than before the accident. A 2014 survey of 5000 residents in and 500 evacuees from Fukushima City (capital city outside the designated evacuation zone) found health concerns regarding external and internal radiation exposure was higher among the evacuees. 3 Fear and anxiety about radiation was also reported among other groups involved in the extensive migration caused by the NPP disaster. 4
Fukushima Medical University launched a prefecture-wide cohort survey (the Fukushima Health Management Survey [FHMS]) to estimate the level of external exposure to radiation, investigate mental and physical health of the population, and provide counseling services to distressed residents. 5 We previously found that 1 in 4 mothers who delivered within 1 year after the disaster screened positive for depression. 6 This finding underscores the public health priority in Fukushima of careful mental health reassessments and support for mothers with small children.
The overall aims of postpartum care are to identify health problems of mothers and babies at an early stage and to help mothers to become confident in parenting. 7 Our previous report on new mothers living in Fukushima City found that the proportion of mothers lacking confidence in child rearing increased 10% in the disaster year and was associated with interpersonal problems at home. 8 The current analysis extends these findings by focusing on maternal confidence of mothers across Fukushima Prefecture in subsequent years. Specifically, our aims were to examine whether disaster-related stressors (evacuation and concern about radiation) were associated with maternal confidence and whether maternal confidence moderated the association between disaster-related stressors and depressive symptoms. The analyses were replicated with data from 2012 and 2013 to determine the temporal stability of the findings.
Methods
Setting and Procedure
The Pregnancy and Birth Survey of the FHMS has been conducted every year since the disaster. 9 This mail survey targets different groups of women who registered their pregnancies in a specified period in each year. In Japan, every pregnant woman is required to register her pregnancy and receives a maternal and child health handbook. The aim of this registration system is to provide free access to antenatal care and well-child visits.
Participants and Recruitment
The 2012 survey targeted women who registered their pregnancies from August 1, 2011, to July 31, 2012, and the 2013 survey targeted those registered from August 1, 2012, to July 31, 2013. Lists of women who had registered their pregnancies within the designated period were obtained from all municipalities in the prefecture, based on the above-mentioned national pregnancy registration. Reminders were sent once for the 2012 survey and twice for the 2013 survey (June 28, 2013, for the 2012 survey; May 10 and July 31, 2014, for the 2013 survey). Data collection continued for about 1 year (till November 30, 2013, for the 2012 survey and December 26, 2014, for the 2013 survey).
Of the 14516 identified women in 2012, 7181 (49.5%) returned the questionnaires. The present analysis focused on the 6686 mothers with singleton live births and complete data on depression screen and maternal self-confidence (93.1% of mothers who returned the questionnaire). Of the 15218 identified women in 2013, 7260 (47.7%) returned the questionnaires. The analysis focused on the 6423 women with singleton live births and complete data on depression screen and maternal self-confidence (88.5% of mothers who returned the questionnaire). Among respondents with live births in 2013, 150 had given birth and responded to the 2012 survey.
Data Management and Sources
The database from the FHMS is computerized and managed centrally by the Radiation Medical Science Center of the FHMS. Currently, access to the data is limited to the center-related staff, who also respond to requests for specific analyses. Expanded access is in the planning stages. In the current study, we analyzed data from the second and third surveys in 2012 and 2013 because questions regarding maternal confidence and evacuation were introduced only in the second year.
Data Items
The analysis focused on maternal confidence and depressive symptoms. Maternal confidence was assessed by a single question: “Are there any moments when you don’t feel confident about child rearing?” 8 The response codes were “yes,” “unsure,” and “no”; “yes” or “unsure” were classified as lacking confidence in child rearing. This measure was included as a key indicator in the National Maternal and Child Health Plan evaluation from 2001 to 2014 and was validated and used in our previous studies. 8 To assess depressive symptoms, a standard 2-item screening measure was administered. The items assess depressed mood and anhedonia over the past month 6 : “During the past month, have you often felt down, depressed, or hopeless?” and “During the past month, have you often found little interest or pleasure in doing things?” Mothers who answered “yes” to one or both of these questions were classified as positive on depressive symptoms. We provided telephone counseling by midwives and nurses to mothers who were positive on both symptoms and wrote concerns in a free space.
General risk factors for maternal self-confidence and depressive symptoms included in the analyses were the following: maternal factors (age at pregnancy, number of postpartum days at the time of survey response, psychiatric history, residential region, relocation after becoming pregnant), obstetrical factors (gestational week at birth and complications during pregnancy from a list of 15 complications), and infant characteristics (sex, birth weight, and anomalies). Residential regions were classified into 3 major, commonly used regions: the most populated central region with relatively higher radiation levels, the coastal region closest to the NPP and partially designated as an evacuation zone, and the mountainous region farthest from the NPP. Relocation after pregnancy was based on whether the address provided in the returned questionnaire differed from the mailing address listed at the time the pregnancy was registered.
Fukushima-specific risk factors were evacuation at the time of survey (designated and self-determined) and concern about radiation, defined as bottle feeding their babies because of radiation concerns (vs breast feeding, bottle feeding as a result of lack of breast milk, or bottle feeding for other reasons).
Statistical Analysis
With regard to the analysis of factors associated with maternal confidence and depressive symptoms, we used the Wilcoxon-Mann-Whitney rank-sum test for continuous variables and χ 2 tests for categorical variables (Tables 1-4). We confirmed that factors associated with the 2 outcomes were consistent with the results of our previous studies conducted in Fukushima.6,8,10 We then conducted unadjusted and adjusted logistic regression analyses. Variables that were significantly associated with both the outcome (depressive symptoms) and the independent variables (current evacuation or concern toward radiation) were considered as potential confounders. Relocation after pregnancy, however, was considered as a potential mediator because it could occur more often among mothers in temporary housing and with concern about radiation and, at the same time, could result in social isolation and increased risk of parenting difficulty. 11 The Sobel-Goodman test was used to confirm the presence of a mediation effect. The same procedure was repeated for the 2012 and 2013 data sets, with the following variables entered into multivariable analyses: maternal age and postpartum days at the time of survey into the current evacuation model in 2012, postpartum days at the time of survey, first-time motherhood and obstetrical complications into the radiation concern model in 2012, first-time motherhood into the current evacuation model in 2013, and obstetrical complications into the radiation concern model in 2013.
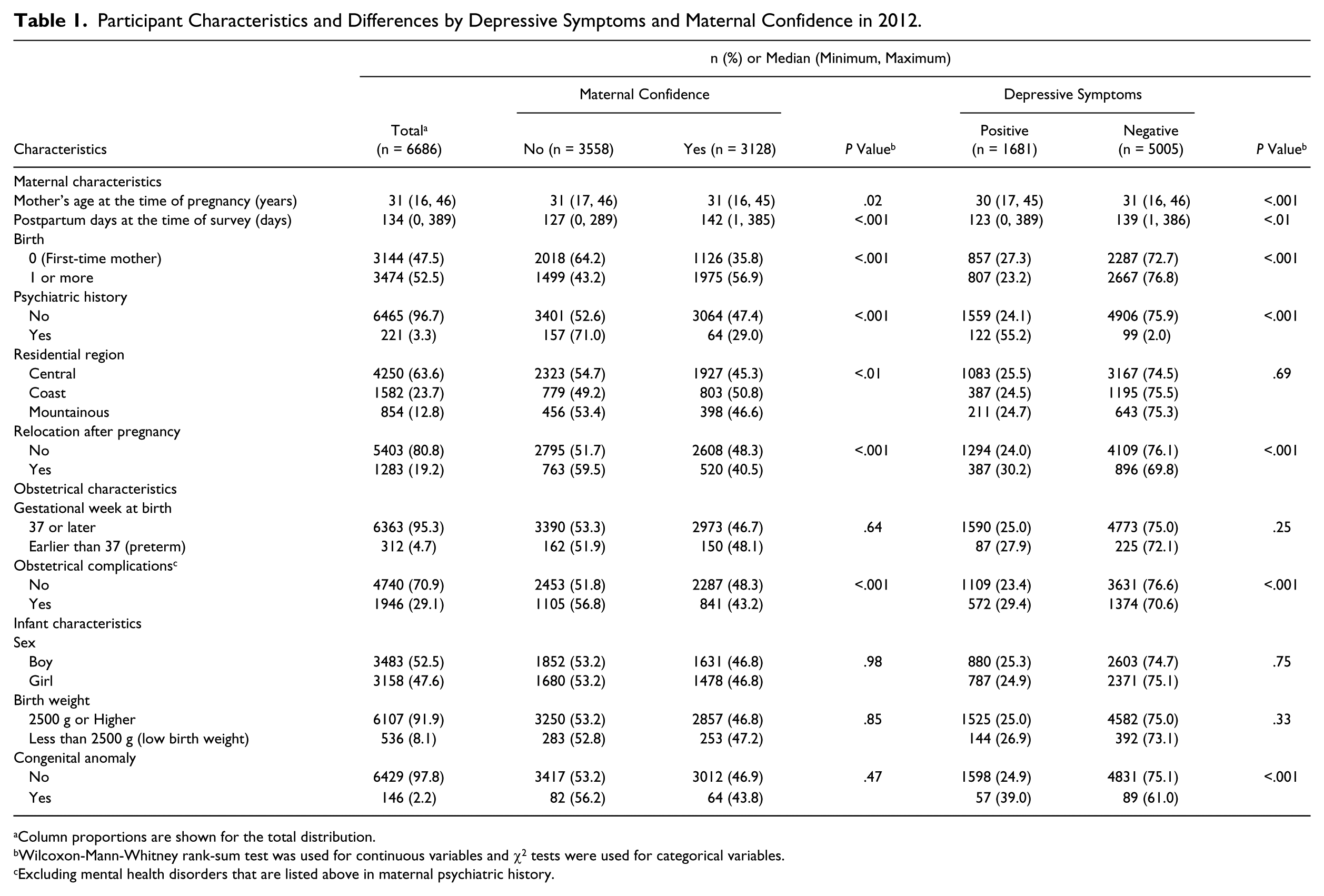
Participant Characteristics and Differences by Depressive Symptoms and Maternal Confidence in 2012.
Column proportions are shown for the total distribution.
Wilcoxon-Mann-Whitney rank-sum test was used for continuous variables and χ2 tests were used for categorical variables.
Excluding mental health disorders that are listed above in maternal psychiatric history.
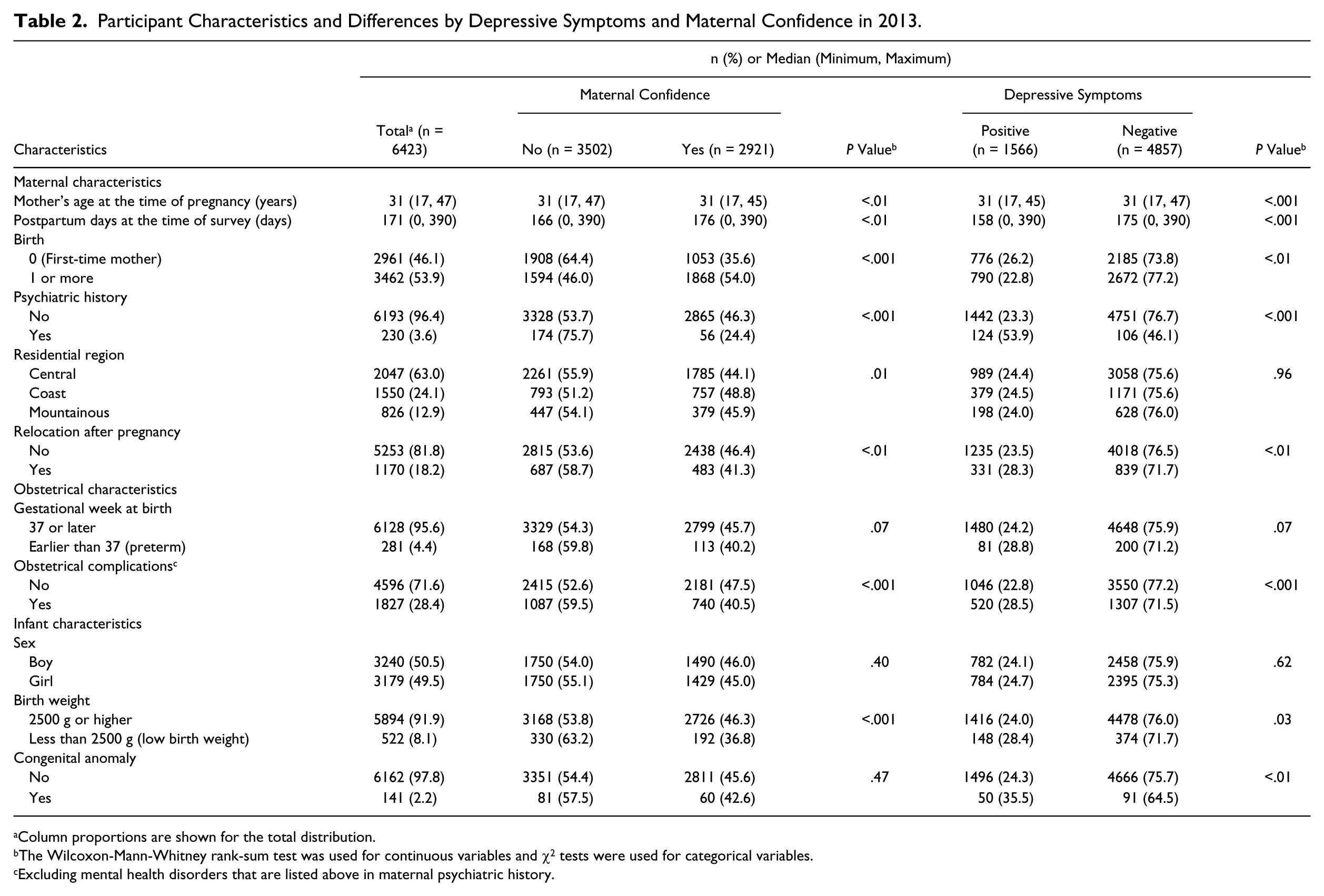
Participant Characteristics and Differences by Depressive Symptoms and Maternal Confidence in 2013.
Column proportions are shown for the total distribution.
The Wilcoxon-Mann-Whitney rank-sum test was used for continuous variables and χ2 tests were used for categorical variables.
Excluding mental health disorders that are listed above in maternal psychiatric history.
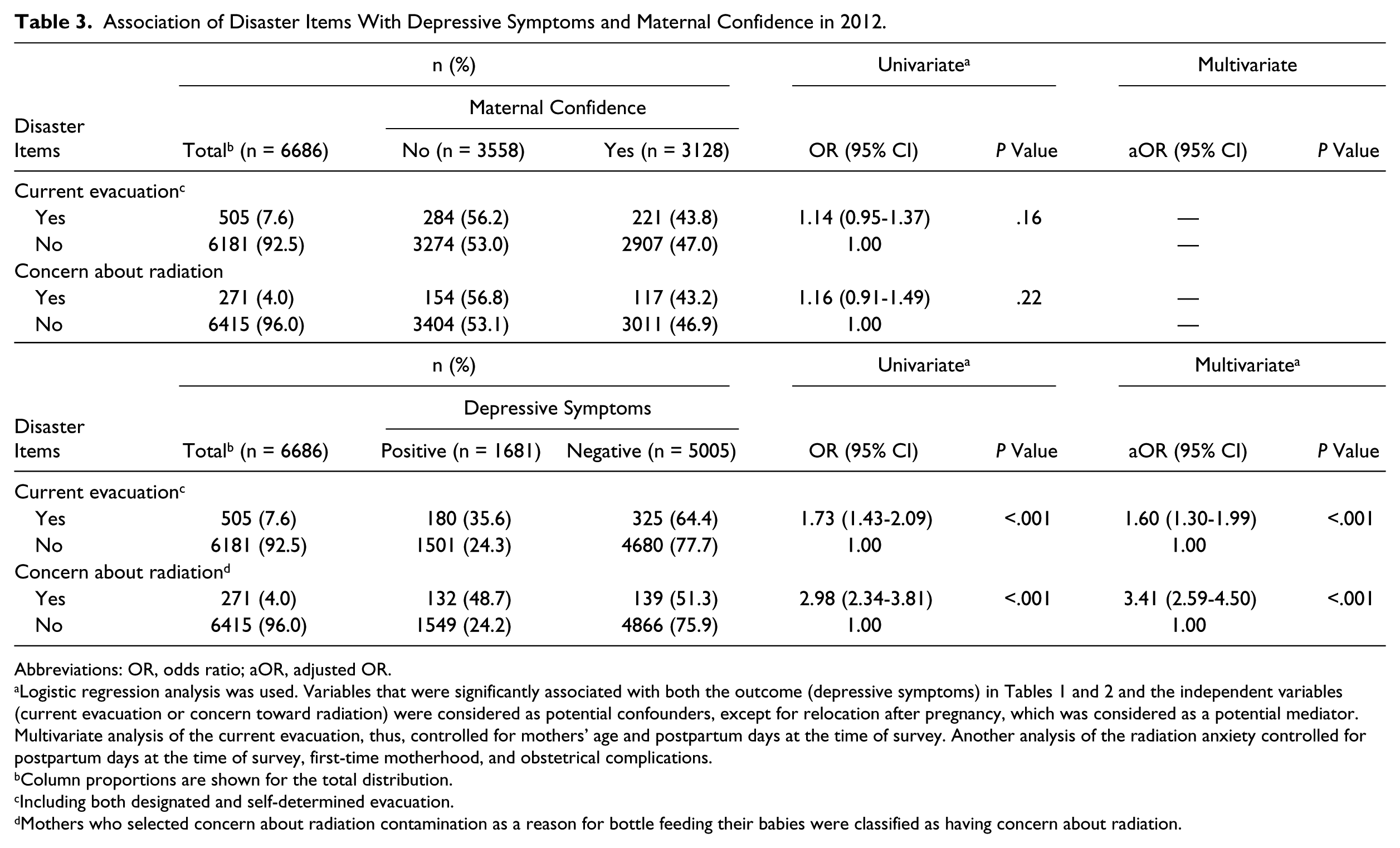
Association of Disaster Items With Depressive Symptoms and Maternal Confidence in 2012.
Abbreviations: OR, odds ratio; aOR, adjusted OR.
Logistic regression analysis was used. Variables that were significantly associated with both the outcome (depressive symptoms) in Tables 1 and 2 and the independent variables (current evacuation or concern toward radiation) were considered as potential confounders, except for relocation after pregnancy, which was considered as a potential mediator. Multivariate analysis of the current evacuation, thus, controlled for mothers’ age and postpartum days at the time of survey. Another analysis of the radiation anxiety controlled for postpartum days at the time of survey, first-time motherhood, and obstetrical complications.
Column proportions are shown for the total distribution.
Including both designated and self-determined evacuation.
Mothers who selected concern about radiation contamination as a reason for bottle feeding their babies were classified as having concern about radiation.
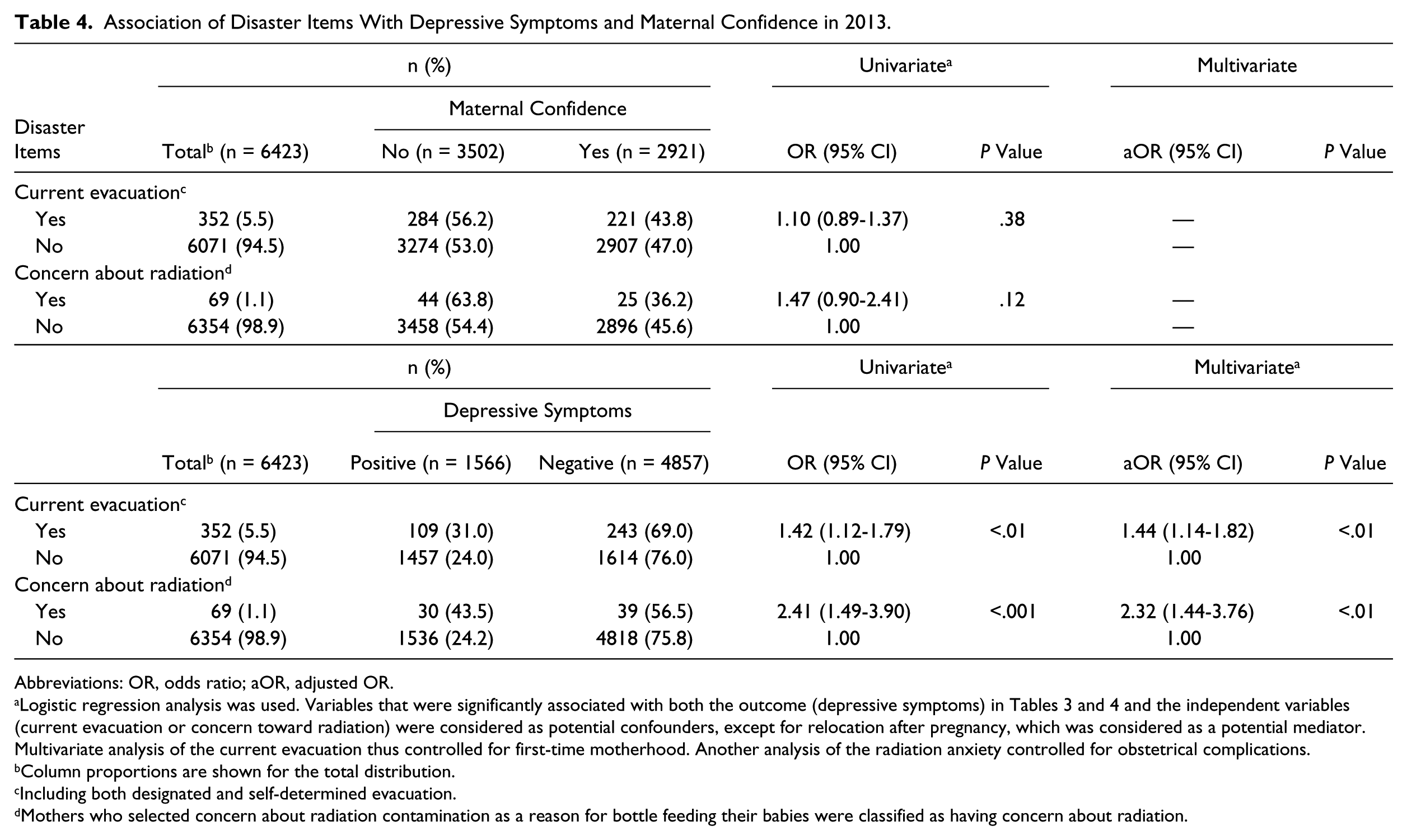
Association of Disaster Items With Depressive Symptoms and Maternal Confidence in 2013.
Abbreviations: OR, odds ratio; aOR, adjusted OR.
Logistic regression analysis was used. Variables that were significantly associated with both the outcome (depressive symptoms) in Tables 3 and 4 and the independent variables (current evacuation or concern toward radiation) were considered as potential confounders, except for relocation after pregnancy, which was considered as a potential mediator. Multivariate analysis of the current evacuation thus controlled for first-time motherhood. Another analysis of the radiation anxiety controlled for obstetrical complications.
Column proportions are shown for the total distribution.
Including both designated and self-determined evacuation.
Mothers who selected concern about radiation contamination as a reason for bottle feeding their babies were classified as having concern about radiation.
Two additional analyses were conducted. The first analysis tested changes in results when answering “yes” (excluding “unsure”) to having times when they lacked self-confidence was classified as lacking confidence in child rearing. The second analysis explored association between maternal confidence and depressive symptoms using χ2 tests and odds ratios (ORs). We further tested a potential moderator effect of maternal confidence on the relationship between disaster-related stressors and depressive symptoms by conducting stratified multivariable analyses by maternal confidence.
A conservative P value of less than .01 was considered as statistically significant given the large sample sizes and the number of comparisons. All statistical analyses were conducted using STATA, version 10.
Ethical Considerations
The ethics committee of Fukushima Medical University approved this study (No. 13048). The survey aims were explained to all respondents in a cover letter that was sent out with the questionnaire. By responding to the survey, participants were considered to have consented to participation.
Results
The median maternal age was 31 years in both 2012 and 2013, and the median number of postpartum days at the time of the survey was 134 in 2012 and 171 in 2013 (Tables 1 and 2). The proportion of infants with a low birth weight was 8.1%, whereas 2.2% were born with congenital anomalies in both 2012 and 2013.
Among the 6686 women analyzed in 2012, 53.2% lacked confidence in child rearing and 25.1% screened positive for depressive symptoms. The percentages among 4623 women in the 2013 survey were 54.5% and 24.4%. When the prevalence of lower maternal confidence and depression screen positive was compared between mothers who responded within 6 months postpartum or later, only the depression screen positive in 2013 showed a significant difference (26.2% for within 6 months and 22.0% for later responses; P < .001). We note that by comparison, for the 2012 survey, the proportions were 25.8% within 6 months and 23.2% for later responses.
In both years, mothers lacking confidence were more likely to be older, mothers who had responded on an earlier postpartum day, first-time mothers, those who resided in the central region, those who had relocated after this pregnancy, and those who had a history of psychiatric disorder and complications during pregnancy (Tables 1-4). Mothers who screened positive for depressive symptoms were more likely to be younger, mother who had responded on an earlier postpartum day, first-time mothers, those who had relocated after this pregnancy, and those who had reported a history of psychiatric disorder and complications during pregnancy.
In univariable analysis (Tables 3 and 4), maternal confidence was not significantly associated with either current evacuation status or concern about radiation in either year. On the other hand, depressive symptoms were significantly associated with both disaster-related stressors. These associations remained significant after controlling for potential confounding factors that were significant in the univariable analysis: current evacuation in 2012 (adjusted OR [aOR] = 1.60; 95% CI = 1.30-1.99, P < .001), concern about radiation in 2012 (aOR = 3.41; 95% CI = 2.59-4.50), current evacuation in 2013 (aOR = 1.44; 95% CI = 1.14-1.82; P < .01), and concern about radiation in 2013 (aOR = 2.32; 95% CI = 1.44-3.76; P < .01). Of note, the proportion of mothers who were concerned about radiation (specifically, bottle feeding their babies because of radiation concern) decreased from 4% in 2012 to 1% in 2013.
Two additional analyses were conducted. First, the analysis redefining lower maternal self-confidence as answering “yes” to having times when they lacked self-confidence showed that 15.5% of mothers in 2012 and 17.6% in 2013 were in that group. We found a significant association using this for the 2012 sample with radiation concern after controlling for potential confounders (postpartum days at the time of survey, first-time motherhood, and obstetrical complications; aOR = 1.88; 95% CI = 1.36-2.59; P < .001) but not for the 2013 sample. Second, there was a significant association between maternal self-confidence and depressive symptoms (P < .001 in both 2012 and 2013). That is, mothers with lower maternal confidence were more likely to screen positive for depressive symptoms. Furthermore, results in Table 5 from repeating the above multivariable analyses (on depressive symptoms and associated factors) stratified by maternal confidence showed a slight increase in OR for less-confident mothers compared with confident mothers in both years for the analysis of current evacuation.
Association of Disaster Items With Depressive Symptoms Stratified by Maternal Confidence in 2012 and 2013.
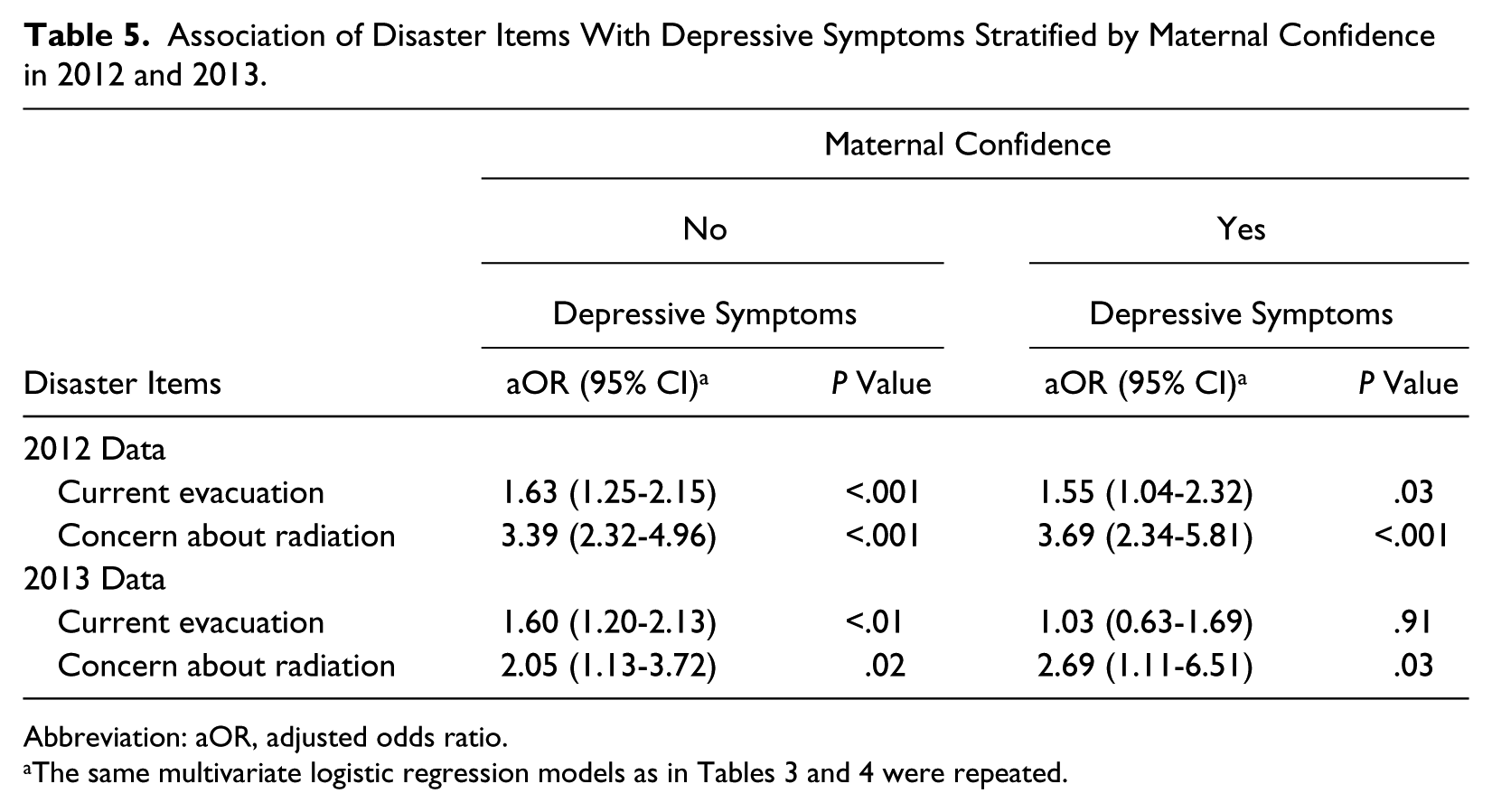
Abbreviation: aOR, adjusted odds ratio.
Discussion
Similar proportions of mothers expressed decreased self-confidence and depressive symptoms during the second and third years after the 2011 Fukushima NPP accident. For reference, in the year before the accident, 50% of mothers in Fukushima city had decreased maternal confidence, whereas in 2011, when the accident occurred, the percentage increased to 60% and then declined to 53% in 2012. 8 This proportion in Fukushima city is similar to that in the prefectural data reported in the present study. Regarding depressive symptoms, we found that as high as 27% were screened positive in the first FHMS survey. 6 The present study showed that the prevalence did not show a significant decline, and mental health support for mothers with infants continues to be a high priority in Fukushima. Considering that our telephone counseling service provided as a part of the FHMS only reached those who participated in the survey and expressed symptoms and concerns, mental health support for mothers needs to be incorporated more broadly into existing maternal and child health services in the prefecture. One possible mode of wider support is the maternal and child health handbook provided to all pregnant women in Japan. The handbook consists of nationally standardized and municipality modifiable parts, and the latter could be utilized to respond to local mothers’ information needs. Another option is the child health checkups. We previously reported how Fukushima City utilized the opportunity to strengthen the mental health support for mothers after the NPP accident.8,12
Comparison of how disaster-related stressors were associated with parenting and mental health indicators showed an interesting difference, which may indicate resilience of Fukushima mothers. The disaster-related stressors did not associate with maternal confidence (as a parenting indicator), although they showed significant association with depressive symptoms (as mental health indicators). Even when lacking maternal confidence was redefined as those who endorsed not feeling confident about child rearing (excluding not sure), it was associated only with the concern about radiation in 2012. Our previous study revealed that the one-question maternal confidence measure is strongly associated with mothers’ general self-efficacy. 10 There are a few recent studies in a nondisaster setting exploring association among maternal self-efficacy, postpartum depression, and stressors.13,14 Similar to our finding without the obvious moderation effect of maternal confidence, they report that the association between stressors and depression is independent of maternal self-efficacy without mediation and moderation effects.
Similarly, a recent review of Japanese parenting studies urged that a traditional view of motherhood as innate should be changed to a more holistic view that parenting skills reflect changing and complex sociocultural environments. 15 The notion is that maternal confidence as a measure of parenting is associated not just with mothers’ mental health, but also reflects broader sociocultural factors. This may explain, in part, our findings that maternal confidence and depressive symptoms were strongly associated, but their association with disaster-related stressors differed. It may also help explain our finding that maternal confidence was associated with relocation after pregnancy but not with the evacuation status per se. Of note, “resilience refers to the capacity for adapting successfully in the context of adversity.” 16 The present study merely shows an absence of decline in maternal confidence, and further investigation regarding positive adaptation behaviors among mothers is needed to confirm their resilience.
Our results, in fact, suggest that long-term evacuation status and concerns toward radiation continue to affect maternal mental health in particular. Such negative psychological consequences among mothers is expected to persist based on findings from previous accidents in Three Mile Island and Chernobyl.17,18 Likewise, a recent analysis of the FHMS data among evacuees in a coastal region revealed that the concern about radiation risks was associated with psychological distress. 19 It is, thus, recommended that mental health support for mothers be strengthened and close attention is paid to their evacuation status and concerns regarding radiation.
On the positive side, the proportion of mothers who bottle fed their babies out of concern about radiation declined from 2012 to 2013. Similarly, the top 3 contents of FHMS’s telephone counseling for depressed mothers showed that the ranking of concern about radiation changed from the top in 2011 to third in 2012 and was no longer in the ranking in 2013. 20 Major concerns in 2012 and 2013 were about mothers’ and children’s health and parenting. Thus, radiation concerns should not be the exclusive focus of postpartum health care, particularly if mental health and parenting support for mothers are integrated into existing health systems. 21 We must be cautious, however, in drawing inferences about mothers’ concerns, which could reflect underlying worries about radiation. After both the Chernobyl and Three Mile Island accidents, the majority of mothers of young children believed that their health was affected by the accidents, and this belief contributed strongly to their negative views of their and their children’s health. 17
A major strength of the present study was its wide coverage of all pregnant women in Fukushima Prefecture, which was possible because of the national pregnancy registration system. There were, however, 3 major limitations. First, the response rate was <50%, which might have influenced the prevalence figures for maternal confidence and depressive symptoms. Similarities with data from previous studies indicate that such response bias is unlikely, however. Second, we used a proxy measure to assess mothers’ concerns about radiation and could only detect those mothers who altered their babies’ feeding methods as a result of concerns about radiation. The proportion of mothers who were concerned about radiation contamination, but not to the extent of changing their parenting behavior, might be higher. Third, because the measures were embedded in a longer questionnaire about current and past health history, we were only able to include screening items of depressive symptoms and maternal self-confidence. Future studies should incorporate more comprehensive measures to confirm the present findings.
Conclusion
The analysis of data from the population-based FHMS sample of mothers with infants born in 2012 and 2013 suggested that maternal confidence was not affected by the disaster-related stressors, indicating resilience in parenting. On the other hand, we confirmed that mothers’ experiences and concerns in the aftermath of nuclear disaster were associated with depressive symptoms, highlighting the importance of providing ongoing mental health support. Such efforts should be incorporated into existing maternal and child health services, with special attention provided to evacuees and mothers who express concerns about possible radiation exposure.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The findings and conclusions of this article are solely the responsibility of the authors and do not represent the official views of Fukushima Prefecture government.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The surveys were supported by the national “Health Fund for Children and Adults Affected by the Nuclear Incident.”