
Abstract
The purpose of this study was to examine the factors contributing to achieving successful aging (SA) among the Korean older population and identified the strength of each factor’s contribution to SA. We extensively searched 4 Korean and 3 English online databases, extracting a total of 64 studies for the analysis. Finally, 42 associated factors and 347 correlation coefficients were found, which were then categorized into 5 domains: functional, psychological, familial, social, and demographic. The psychological domain had the highest effect size. This was followed, in descending order, by the social, functional and familial, and demographic domains. Importantly, the familial domain, which has not been explored in many existing SA models, emerged as a notable predictor. This study is meaningful in terms of understanding one of the minority older populations more deeply and providing stronger evidence for developing evidence-based intervention programs for Korean older adults.
Introduction
The concept of successful aging (SA) refers to having an overall positive aging experience despite the inevitable losses and gradual deterioration associated with aging. 1 Recently, it has become an important concept representing the current demographic changes of an increasingly older population. Along with an extended life expectancy, it is important to consider in gerontology how well older adults age, rather than just how long they live. Previous literature has contributed to conceptualizing SA. The most widely used model of Rowe and Kahn 2 defined SA by differentiating it from “usual aging” and addressing its elements. According to Rowe and Kahn, 2 in order to achieve SA, older individuals should avoid diseases and disabilities, maintain a high level of physical and cognitive functions, and actively engage in a social life.
Culture may be an important factor that strongly influences the aging process. For this reason, the components of SA should be nested within the culture to which one belongs. However, despite the plethora of definitions and models of SA explored by many researchers, a few appear to have considered the cultural aspects. 3 In this regard, the current SA models have received criticism. To date, the existing models do not show many patterns of SA; rather, they represent fixed and end-point criteria. Moreover, the models typically have a Western-centric view. 4 This might lead to a lack of understanding of the aging experience of the minority older populations.
South Korea is experiencing a relatively rapid demographic transition from high to low fertility and mortality. 5 In fact, Chung 6 reported that the rate of aging in Korean society is much faster than it is in other developed countries, such as Japan, France, or Sweden. In particular, the year when the proportion of the population aged 65 years and older reached 7% was 1865 in France, 1890 in Sweden, and 1970 in Japan. The length of time it took for this proportion to double (up to 14%) was 115 years in France, 85 years in Sweden, and 25 years in Japan. However, in South Korea, the proportion of those who were aged 65 years and older reached 7% in 2000, and this is expected to double within just 22 years (2022). 6 More interestingly, it is projected that the rate of aging is going to increase. 5 In addition, the suicide rate of Korean older adults is much higher than the highest rate in the countries of the Organization for Economic Cooperation and Development (OECD)—there were 80.3 deaths per 100 000 individuals according to the 2010 data.7,8 Furthermore, the rate was significantly higher than that of young or middle-aged adults, which were 9.4 deaths and 30.9 deaths, respectively. The Korean older population, therefore, seem to need an urgent care plan and policy to enhance their quality of life and help them undergo the aging process successfully.
So far, numerous studies have examined the factors associated with SA among Korean older adults.9,10 These studies are helpful with regard to developing diverse care plans and interventions for this population. However, no publication, as far as we know, has attempted to synthesize those results and present the overall correlates of SA in Koreans. Thus, the purposes of this study were to examine the correlates of SA and explore the correlates that have the strongest contribution to achieving SA in the Korean older population.
Literature Review
Confucianism is the central philosophy in South Korea. It originated in China and went on to have a considerable influence on other East Asian countries, including South Korea. 11 The current Korean older population also have lived under the influence of Confucianism. In addition, the current Korean older population has experienced a number of important historical events, including Japanese colonialism (1910-1945), the Korean War in the 1950s, and decades of division thereafter between South and North Korea, the rapid economic development (economic boom) in the 1960s and 1970s, and the democracy movement in the 1980s. While experiencing these events, Korean people have attempted to survive and overcome their daily life difficulties by working together as a family and society through strengthening their adherence to Confucian values. 12 For instance, during the economic boom in the 1960s and 1970s, workers in South Korea dedicated themselves to their companies to show loyalty to their country. 13 In other words, they considered their company and country as the same and were willing to sacrifice themselves for the company. Within the family unit, education and social success have been highly emphasized. In particular, mothers have sacrificed themselves for their husbands’ social success and children’s educational success (ie, getting into a good university), and children have been driven to achieve social success in the name of filial piety. 14 Paik 12 described how the Korean older people who went through this tumultuous period are those who grew up in a traditional agricultural society but later experienced rapid modernization. Consequently, they tend to have a strong sense of nationalism and collectivism. 12 Family-centered values and thoughts derived from traditional Confucianism values are still highly prevalent in this generation.
Methods
Data Collection
This study followed the guidelines of Preferred Reporting Items for Systematic Reviews and Meta-Analysis checklist (PRISMA). To find relevant literature, we searched 4 Korean online databases (RISS, KISS, DBpia, and National Assembly Library) and 3 English databases (PubMed, CINAHL, and SCOPUS). The search terms we used for the Korean databases were “older adult,” “older age,” and “successful aging” (in Korean language). The search terms we used for the English databases were “successful aging,” “factor” (or “correlate”) and “Korean.” The final search date was October 15, 2015. The PICOS (Participants, Intervention, Comparator, Outcome, Study design) framework was used for selecting the studies. For participants (P), we included studies that were conducted on Korean older adults aged older than 60 years who lived in South Korea. For outcome (O), we examined the relationships between correlates as independent variables and successful aging as the dependent variable. For study design (S), we used the studies reporting the correlation coefficient (Pearson’s r). Intervention (I) and comparator (C) were not applicable for the criteria of this study. The studies were excluded if they (a) used qualitative methodologies, (b) were experimental, and (c) did not report a Pearson’s r. First, 988 studies were discovered; however, after removing duplicates (n = 455), and excluding the studies in accordance with the exclusion criteria (n = 469), 64 studies remained. No additional studies were found through a reference search; therefore, 64 studies were included in the analysis (Figure 1).
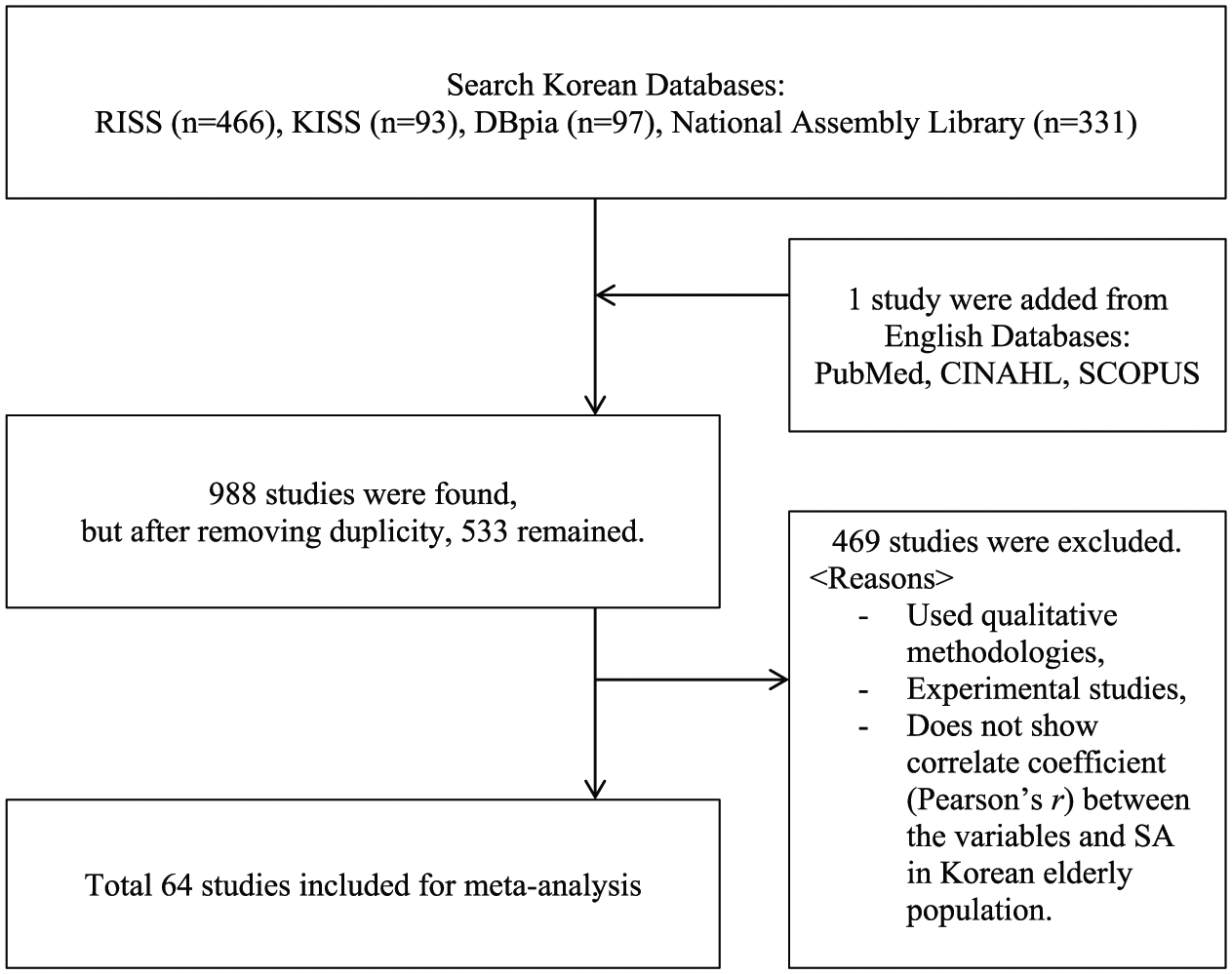
Flow diagram of study selection. SA, successful aging.
Data Analysis
The data were extracted and coded from the included studies as follows: study information (title, authors, year of publication, study type (eg, journal article or dissertation and sample size), participant characteristics (type of residency [eg, home or facility] and residential district), SA measurement, independent variables (correlates), dependent variables (successful aging), and correlation coefficient (Pearson’s r). To achieve reliability, 2 of the authors conducted data extraction and coding processes separately and later matched the results. Any disagreements were discussed until achieving 100% agreement.
In total, 347 independent variables were extracted from 64 studies. The variables with same concepts were then merged into a broader concept. Therefore, 42 concepts emerged that were categorized into 5 broader domains: functional, psychological, familial, social, and demographic. The entire categorization process was performed by the first and second authors. Furthermore, 2 experts—a professor of gerontological nursing and an expert in meta-analysis—reviewed and confirmed the results by cross-checking the included studies. Several discussions were conducted until a complete agreement on the categorization results among all those involved in the analysis was achieved. Finally, all correlation coefficients were transformed into Fisher’s z-scores. The effect sizes were weighted by sample size and inverse variance. Comprehensive Meta-Analysis version 2.0 was used for the analysis.
Results
Meta-Analysis of the Overall Effect Sizes
The correlates (independent variables) we found in this study were either risk factors or protective factors that affected SA negatively and positively, respectively. To examine the strength of the association between the overall domains and SA, all effect sizes were converted with absolute values, and the overall effect size of the correlates of SA was computed. The overall effect size of correlation r (ESr) was 0.41 [0.39, 0.44], which is a large effect size as defined by Cohen. 15 Therefore, we concluded that the correlates we found through the literature search in this study seemed to strongly associate with SA in Korean older adults.
Quality Appraisal
The included studies were evaluated by the criteria, which consisted of 5 elements: description of the study participants, sample size justification, indicating the sampling method, valid and reliable measurement, and appropriate statistical analysis. Each element was coded as either “Y” (yes) or “N” (no) by screening the included studies. Two of the authors of this study performed the quality evaluation separately, and the results were matched. They discussed disagreements until reaching a consensus. Thereafter, we scored the quality of each article. The evaluation results are shown in Table 1. The mean score of the quality of the included studies was 6.375 out of 10.
Included Studies and Quality Appraisals.
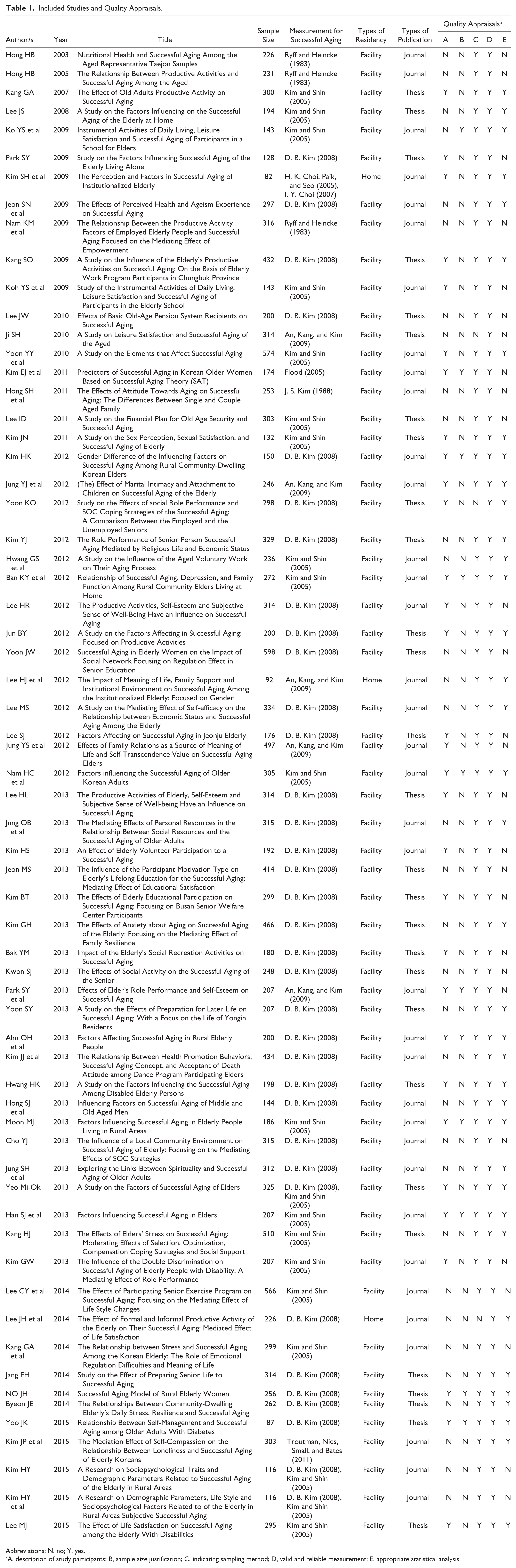
Abbreviations: N, no; Y, yes.
A, description of study participants; B, sample size justification; C, indicating sampling method; D, valid and reliable measurement; E, appropriate statistical analysis.
Publication Bias and Heterogeneity
One of the threats to the validity of a meta-analysis study is publication bias, especially when the results of the published literature are different from those of unpublished literature. 16 To test the possibility of any publication bias in our included studies, we used 2 methods: a funnel plot and Egger’s regression test. 17 The funnel plot, which is the most widely used method to determine publication bias, seemed to show a symmetrical pattern, indicating no possibility of publication bias. Egger’s test, which can statistically test for asymmetry in the funnel plot, 17 also demonstrated that there was no evidence of publication bias in the included studies (intercept = −0.72, SD = 1.052, P = .494).
Moreover, the heterogeneity of the effects was tested using a Q test and an I2 test. The Q value and I2 index were relatively large (Q = 7556.467, df = 346, P < .001 and I2 = 95.4%), which indicates inconsistency in the effect sizes as well as a high degree of heterogeneity. Since we assumed that the studies included in this study were not homogeneous in population parameters, and we wanted to achieve higher generalizability, a random-effects model was applied to this study. A meta-regression was used to test moderator effects. The results revealed that the effect sizes were not influenced by publication year (slope = 0.014 [0.00, 0.03], P = .772), residency type (slope = −0.024 [−0.13, 0.08], P = .813), publication type (slope = −0.008 [−0.05, 0.03], P = .403), sample size (slope = 0.007 [0.00, 0.00], P = .812), or SA measurement (slope = 0.009 [−0.02, 0.04], P = .794).
Effect Sizes of the Domains
The correlates were categorized into 5 domains as mentioned above, and the analysis results showed that each domain was strongly associated with SA in Korean older adults. Particularly, the psychological domain showed the largest effect size (ESr = 0.58 [0.53, 0.63]) compared with other domains; in other words, the psychological domain was the strongest contributor to SA in the Korean older population. This was followed, in descending order of effect size, by the social domain (ESr = 0.42 [0.37, 0.48]), functional domain (ESr = 0.37 [0.31, 0.44]), familial domain (ESr = 0.37 [0.3, 0.45]), and demographic domain (ESr = 0.27 [0.22, 0.32]). The effect sizes between the correlates and SA listed in Figures 2. In addition, the forest plot is illustrated.
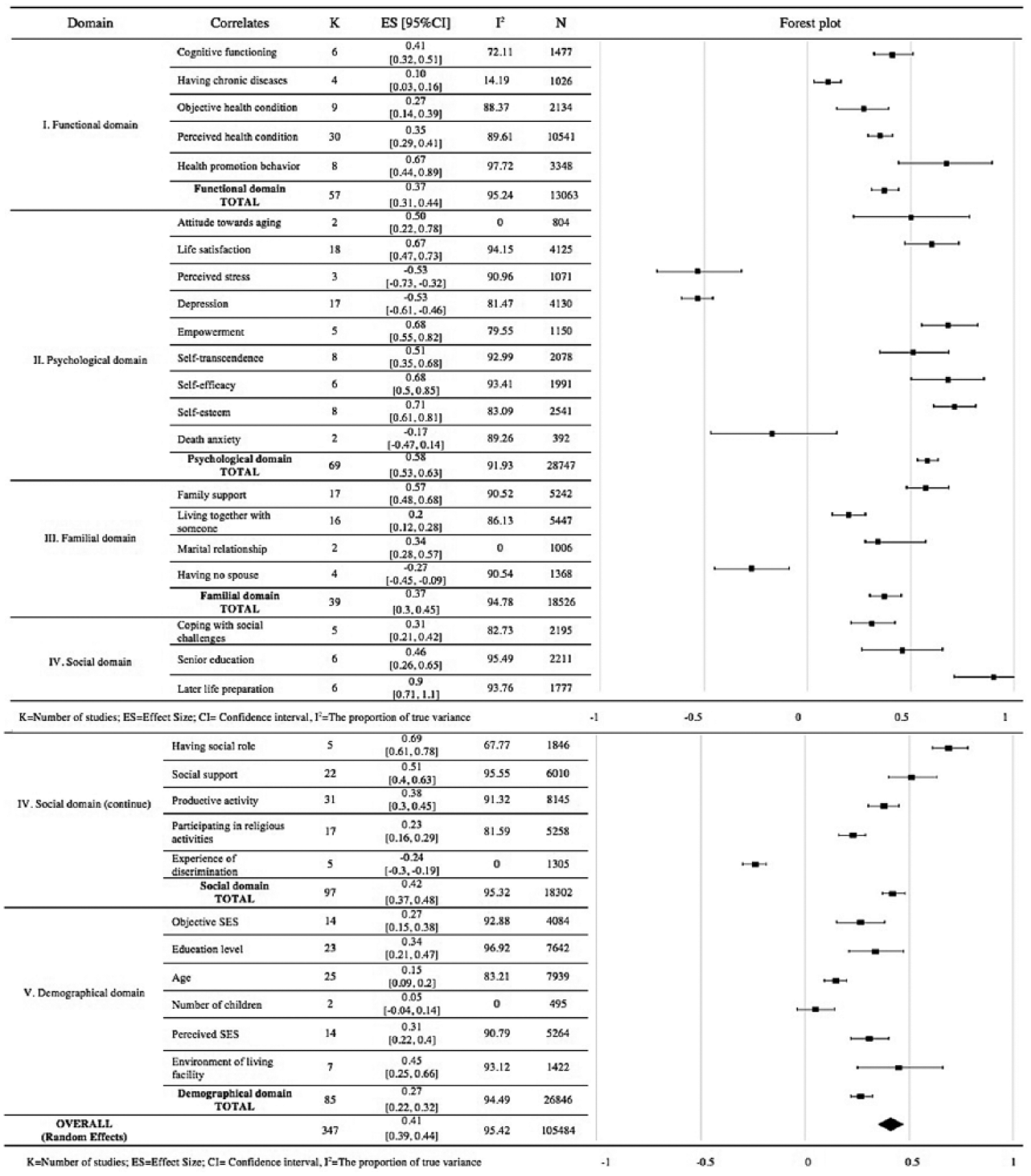
Effect sizes between correlates and successful aging and forest plot.
Functional domain
The factors related to one’s physical/cognitive functions and health conditions were categorized into the functional domain. There were five correlates of SA in this domain: cognitive functioning, having chronic diseases, objective health condition, perceived health condition, and health promotion behavior. Among the factors, health promotion behavior (ESr = 0.67 [0.44, 0.89]) had the largest effect size, and cognitive functioning (ESr = 0.41 [0.32, 0.51]) also showed large effect sizes. Perceived health condition (ESr = 0.35 [0.29, 0.41]), objective health condition (ESr = 0.27 [0.14, 0.39]), and having chronic diseases (ESr = 0.1 [0.03, 0.16]) also showed significant associations with SA.
Psychological domain
Nine psychological factors were allocated into the psychological domain: attitude toward aging, life satisfaction, perceived stress, depression, empowerment, self-transcendence, self-efficacy, self-esteem, and death anxiety. All 9 factors, except death anxiety, had significantly large effect sizes; that is, there were strong associations between these factors and SA in Korean older population. Specifically, perceived stress, depression, and death anxiety showed a negative association with SA, and among those factors, both perceived stress (ESr = −0.53 [−0.73, -0.32]) and depression (ESr = −0.53 [−0.61, −0.46]) had large effect sizes. The other 6 factors showed a significant positive association with SA, and particularly, self-esteem (ESr = 0.71 [0.61, 0.81]), empowerment (ESr = 0.68 [0.55, 0.82]), and self-efficacy (ESr = 0.68 [0.5, 0.85]) showed high effect sizes.
Familial domain
Four correlates were related to family; therefore, they were categorized into the familial domain: family support, living together with someone, marital relationship, and having no spouse. Only having no spouse showed a negative association with SA (ESr = −0.27 [−0.45, −0.09]), while other factors showed a positive association: family support (ESr = 0.57 [0.48, 0.68]), marital relationship (ESr = 0.34 [0.28, 0.57]), and living together with someone (ESr = 0.2 [0.12, 0.28]).
Social domain
The social domain involved 8 factors: coping with social challenges, senior education, later-life preparation, having a social role, social support, productive activity, participating in religious activities, and experience of discrimination. Among these factors, only experience of discrimination showed a significant negative association with SA (ESr = −0.24 [−0.3, −0.19]). The other 7 factors showed a large, positive association with SA: later-life preparation (ESr = 0.9 [0.71, 1.1]), having a social role (ESr = 0.69 [0.61, 0.78]), social support (ESr = 0.51 [0.4, 0.63]), senior education (ESr = 0.46 [0.26, 0.65]), and productive activity (ESr = 0.38 [0.3, 0.45]).
Demographic domain
The 6 demographic correlates were objective socioeconomic status (SES), perceived SES, education level, age, number of children, and residential environment. All the factors, except the number of children, were significantly associated with Korean SA in older population: residential environment (ESr = 0.45 [0.25, 0.66]), education level (ESr = 0.34 [0.21, 0.47]), perceived SES (ESr = 0.31 [0.22, 0.4]), objective SES (ESr = 0.27 [0.15, 0.38]), and age (ESr = 0.15 [0.09, 0.2]).
Discussion
This study explored the factors correlated with SA in Korean older adults through an extensive literature search, and the correlates we found were categorized and quantitatively synthesized into five domains. It was unsurprising that the psychological domain had the strongest effect size. Indeed, according to our previous research, 18 the psychological domain had the strongest contribution to achieving SA in the general population. Further, in this study, the Korean older population appeared to rely most on psychological components to achieving SA.
The social domain had the second highest effect size in achieving SA in this study. In particular, later-life preparation and having a social role had the 2 highest effect sizes among the correlates. In addition, many activity-related factors were strongly associated with SA; for instance, participating in senior educations, religious activities, and productive activity were highly related with achieving SA. It perhaps represents that joining groups and participating in activities seemed to be a big part of Korean older people’s lives. This finding provides useful evidence when developing an intervention program for the Korean older population. For instance, providing a chance to participate in diverse activities may enhance the SA of Korean older adults. On the other hand, the experience of discrimination played a negative role in achieving SA in Koreans. Indeed, Chun et al 19 described in their study that 23.5% of older Koreans reported the experience of discrimination based on education, age, birthplace, or gender, and these experiences highly predicted depressive symptoms and a poor self-rated health.
Functional and familial domains showed similar effect sizes. Especially, according to the results of this study, the family seemed to be important for the SA of Korean older adults. Indeed, among the existing SA models that explored the correlates of SA, family-related correlates were rarely identified. Nonetheless, many family-related correlates were found in this study, including family support, marital relationship and living together with someone, and so on. Most of these correlates showed large effect sizes and a strong association with SA. We assume that this is perhaps due to the influence of Confucianism that places a high value on the relationship between family members and blood ties. 14 This notion is also supported by a previous study conducted in South Korea, wherein it was shown that family cohesion was important for SA of the Korean older population 20 ; more specifically, family cohesion served as a moderator between SES and SA. Thus, even if one had a high SES, having a low family cohesion would weaken the positive relationship between SES and SA.
Interestingly, in terms of functional domain, having chronic diseases had a small effect size. This is peculiar since previous SA models have considered this a highly important factor.2,21,22 We suggest further studies confirm this result in the Korean population; however, we also assume that Koreans tend to value maintaining physical and cognitive functions by implementing health promotion behaviors, regardless of having a chronic disease. According to Yu, 23 there was no significant difference in the degree of SA between Korean older adults who had type 2 diabetes (3.57 ± 0.49) and the general Korean older population (3.54 ± 0.48). The author interpreted this result by stating that Korean older adults tended to have more than one chronic disease; therefore, having a chronic disease did not affect SA by itself, but rather perceived health and health promotion behaviors (self-management with diabetes) were more related to SA. 23
As we expected, there was a finding that we think only Korean people would show—an individual’s economic condition was an important factor in the Korean older population in achieving SA. The factors related to economic condition and its stability, such as an environment of the living facility, education level, and objective/perceived SES, were all significantly associated with SA in Koreans. This is interesting because studies on SA conducted in Western countries have rarely considered economic factors as critical to achieving SA. Cosco et al 24 explored the operation definitions of SA through a systematic literature review. 24 They found 105 definitions of SA in 103 studies. Based on that, they presented 5 constructs of SA: physical, well-being, engagement, personal resources, and extrinsic factors. Extrinsic factors involved environment and finance; however, it was operationalized in just 5.7% of the definitions (6 out of 105 definitions). Even Depp and Jeste, 21 who investigated the predictors of SA, reported that income and education were not related to SA. However, the importance of economic conditions in the Korean older population seemed to be highly stressed in this study, and this result is consistent with a previous study—Lee 20 reported that economic resources acted as a moderator between life satisfaction and SA in the Korean older population. In other words, the strength of the relationship between life satisfaction and SA was determined by existing economic resources.
One of the possible explanations for this phenomenon might be found in the historical period in which they lived. As noted above, the current Korean older population lived through the economic boom in the 1960s and 1970s. After the Korean War, the Koreans were driven to achieve economic prosperity to show loyalty to their country. Indeed, the Korean government at that time generated slogans aimed at unifying public opinion and stressing the importance of hard work for national economic development. 13 Such slogans included “Let us work for a better life” and “The better the economy, the better the life of every laborer.” Specific economic aims were US $1 billion in exports or 10% economic growth. In such circumstances, Korean workers—now Korean older adults—were willing to actively participate and sacrifice themselves for the industrialization of South Korea. The government and public described those workers as “export warriors” or “industrial soldiers” as part of the efforts to motivate them. 13 As such, the current Korean older adults are those who have lived through such an intense period of history and ultimately helped to achieve the economic miracle that is South Korea. Another possible explanation can be found in one of the previous studies. Kim et al 25 examined the association between economic status and mortality of Koreans, and they reported that the mortality of the lowest economic status was much higher in both men and women—2.48 and 2.02 times, respectively. It seemed to be not because of poor education or health behaviors since this relationship persisted even after adjusting health behaviors and past medical histories. Rather, the authors pointed out psychological factors as the contributing factors explaining the relationship between low economic status and high mortality. Thus, it is likely that economic status is somehow related to psychological well-being in the South Koreans. It may, however, be difficult to conclude that this is the main reason why Korean older adults place a high value on economic status for their SA process. Hence, we suggest future studies explore this phenomenon in greater depth in an attempt to confirm this possibility.
This study has critical implications. As their suicide rates say it, Korean older adults are one of the vulnerable populations at this point who need critical care. Moreover, South Korea is now rapidly becoming an aging society, and the health problems related to older adults would become more serious. Therefore, in practical aspects, this study’s findings provide valuable evidence, which could be helpful to health professionals as well as policy makers. Especially, we firmly suggest that health professionals provide cultural specific care plans for the Korean older adults by developing and applying evidence-based intervention programs for them. By facilitating the protective factors and reducing the risk factors identified in this study, the professionals could help this population to undergo their aging process healthily and successfully. In theoretical perspectives, this study shifted from the traditional views of SA, that was criticized as having a Western-centric view 4 and presented diverse patterns of SA by examining culture-specific factors that correlated with SA in the Korean older population.
This study has a limitation. We only included studies identifying the relationship between the variables and SA by providing correlation coefficients (Pearson’s r), and excluded those providing odds ratio or qualitative data. In addition, we discarded several stand-alone variables, which cannot be merged with other variables. For these reasons, there could be several missing variables related to SA.
Conclusion
It is an important task for health professionals to help the older population undergo their aging processes successfully. Multiple studies have attempted to define and measure SA; however, few studies have done this within a specific culture. The current study explored the correlates of SA in the Korean older population, and by meta-analysis, we identified the strength of each correlate’s contribution to achieving SA. We interpreted several correlates of the SA as actually reflecting the Korean older populations’ unique values and thoughts, shaped in response to them experiencing multiple major historical events and living in a unique culture. We believe that this study can help in understanding the older Korean population more deeply, which in turn can help in encouraging them to have a healthy and positive aging process. Finally, we suggest that future studies explore the correlates of SA among other cultures, so that health professionals can provide culturally competent care and treatment to older people from various cultural backgrounds.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Chung-Ang University Research Scholarship Grants in 2016.