
Abstract
Little is known about the prevalence of depression diagnosis in Korea. We aimed to compare the prevalence of depression diagnosis between Medical Aid and health insurance beneficiaries in an outpatient setting in Korea. The data of patients who visited a medical institution for outpatient care in 2015 were extracted from the Health Insurance Review and Assessment Service National Patient Sample claims database, and those diagnosed with major depressive disorder, single episode (F32) or recurrent (F33), were identified. The adjusted odds ratio (aOR) and 95% confidence interval (CI) were estimated through logistic regression analyses. Among the outpatients, 2.51% were diagnosed with depression at least once. Medical Aid beneficiaries (aOR = 1.97; 95% CI = 1.96-1.98) were more likely to be diagnosed with depression than health insurance beneficiaries.
Introduction
Depression is an important public health issue. 1 The number of patients with depression increased by 18% from 2005 to 2015 worldwide, and this trend is expected to continue. 2 Depression is a leading cause of disability worldwide and can lead to suicide at its worst. 2 Suicide is a leading cause of death in Korea. 3 In the United States, the prevalence of depression was shown to have increased significantly in the lower income group, and the expansion of Medicaid coverage for low-income adults led to the increase in depression diagnosis.4,5 However, no recent report on the prevalence of depression diagnosis in Korea has been established in the general population.6,7 The National Health Insurance in Korea covers the entire population and thus provides a rich source of data to study the prevalence of depression diagnosis. In addition, low-income families are entitled to receive a medical assistance scheme called Medical Aid program. Therefore, this study aimed to compare the prevalence of depression diagnosis between national health insurance and Medical Aid beneficiaries in an outpatient setting in Korea, after adjusting for age, sex, type of medical institution, area of residence, and comorbidities.
Methods
The study population was defined as the patients who visited a medical institution for outpatient care between January and December 2015 based on the Health Insurance Review and Assessment Service National Patient Sample claims database. Patients with depression referred to those diagnosed with major depressive disorder, single episode (F32) or recurrent (F33), at least once. Since, the 2015 claims database does not provide the tools that the physicians can use to make a diagnosis, we assumed that they used similar diagnostic tools to make a depression diagnosis regardless of the type of health coverage.8,9
The prevalence of depression diagnosis was calculated as the proportion of outpatients diagnosed with depression, analyzed based on age group (0-19, 20-44, 45-64, 65-84, and ≥85 years), sex, area (rural and urban), type of health care coverage (health insurance and Medical Aid), type of medical institution (primary, secondary, tertiary, and public), and comorbidities. The type of medical institution was defined based on the number of beds and funding source (primary, 0-29 beds; secondary, 30-99 beds; tertiary, ≥100 beds; and public, publicly funded institution). Patients who used Medical Aid at least once were classified as beneficiaries of Medical Aid. Patients with veteran’s coverage were excluded because the number was too small to warrant a separate analysis. Comorbidities include general anxiety disorder (F41.1), panic disorder (F41.0), brief reactive psychosis (F23.9), posttraumatic stress disorder (PTSD) (F43.1), schizophrenia (F20), diabetes (E10-E14), osteoarthritis (M15-M19), rheumatoid arthritis (M05-M06), asthma (J45-J46), ischemic heart diseases (I20-I25), and hypertensive diseases (I10-I15). The unit of analysis was the patient with all factors except for the area and medical institution type, which were based on claims, because a patient may visit multiple institutions.
We conducted several logistic regression analyses to identify the factors associated with depression. Our covariate of interest was health coverage type, and the adjusted variables were age group, sex, area, type of medical institution, and comorbidities. The adjusted odds ratios (aOR) and 95% confidence intervals (CI) were calculated. The level of significance was identified as a P value of <.05. All statistical analyses were performed using the SAS 9.4 for Windows (SAS Institute Inc, Cary, NC, USA). The study protocol was approved by the Institutional Review Board of Sungkyunkwan University (IRB no. 2017-01-004).
Results
Among the 1 403 193 patients who received outpatient care in 2015, 2.51% (n = 35 200) were diagnosed with depression at least once, with a mean (±SD) age of 55.24 (±18.56) years. The prevalence rates of depression were 3.08% and 1.89% in women and men, respectively, and 2.60% and 2.82% in those living in urban and rural areas, respectively (Table 1). Primary (2.54%) and public (4.85%) institutions had the lowest and highest prevalence of depression, respectively. Furthermore, the prevalence of depression among Medical Aid beneficiaries was 8.22%, whereas that among health insurance beneficiaries was 2.32%. Patients with comorbidities displayed higher prevalence than those without comorbidities, ranging from 3.24% for asthma to 50.83% for PTSD.
General Characteristics of the Study Population. a
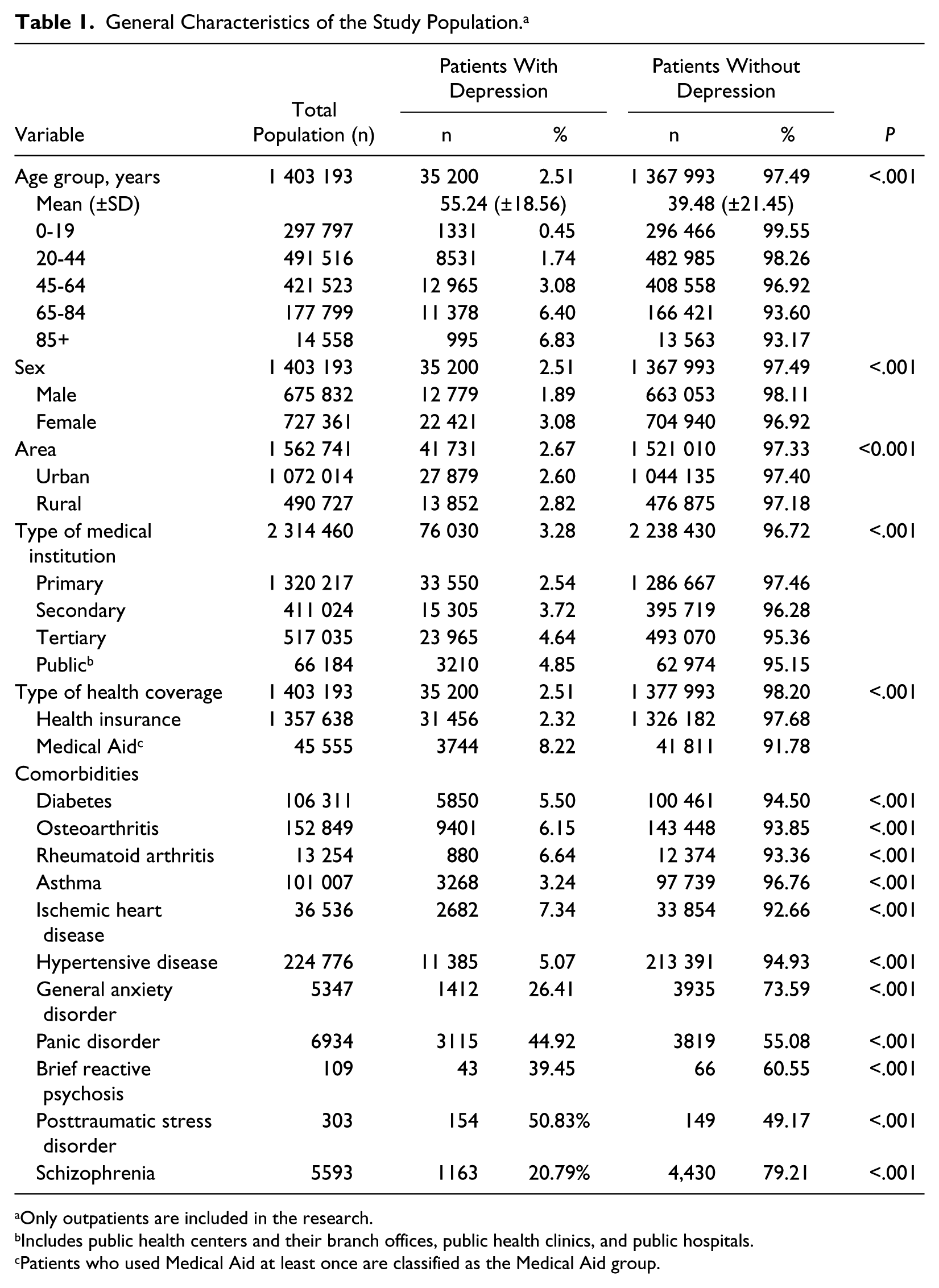
Only outpatients are included in the research.
Includes public health centers and their branch offices, public health clinics, and public hospitals.
Patients who used Medical Aid at least once are classified as the Medical Aid group.
The results of the multivariate logistic regression analysis showed that Medical Aid beneficiaries showed higher odds of being diagnosed with depression than health insurance beneficiaries (aOR = 1.97; 95% CI = 1.96-1.98). Moreover, the depression likelihood increased with age until it peaked at 65 to 84 years (aOR = 1.37; 95% CI = 1.36-1.38) and declined at ≥85 years (aOR = 1.24; 95% CI = 1.23-1.26). Women (aOR = 1.34; 95% CI = 1.33-1.35) were more likely diagnosed with depression than men. Patients from tertiary hospitals (aOR = 1.45; 95% CI = 1.44-1.46) and those from public medical institutions (aOR = 0.70; 95% CI = 0.69-0.71) were the most and least likely diagnosed with depression, respectively (Table 2).
Multivariate Logistic Regression Analysis of Factors Associated With the Prevalence of Depression Among Koreans in 2015.
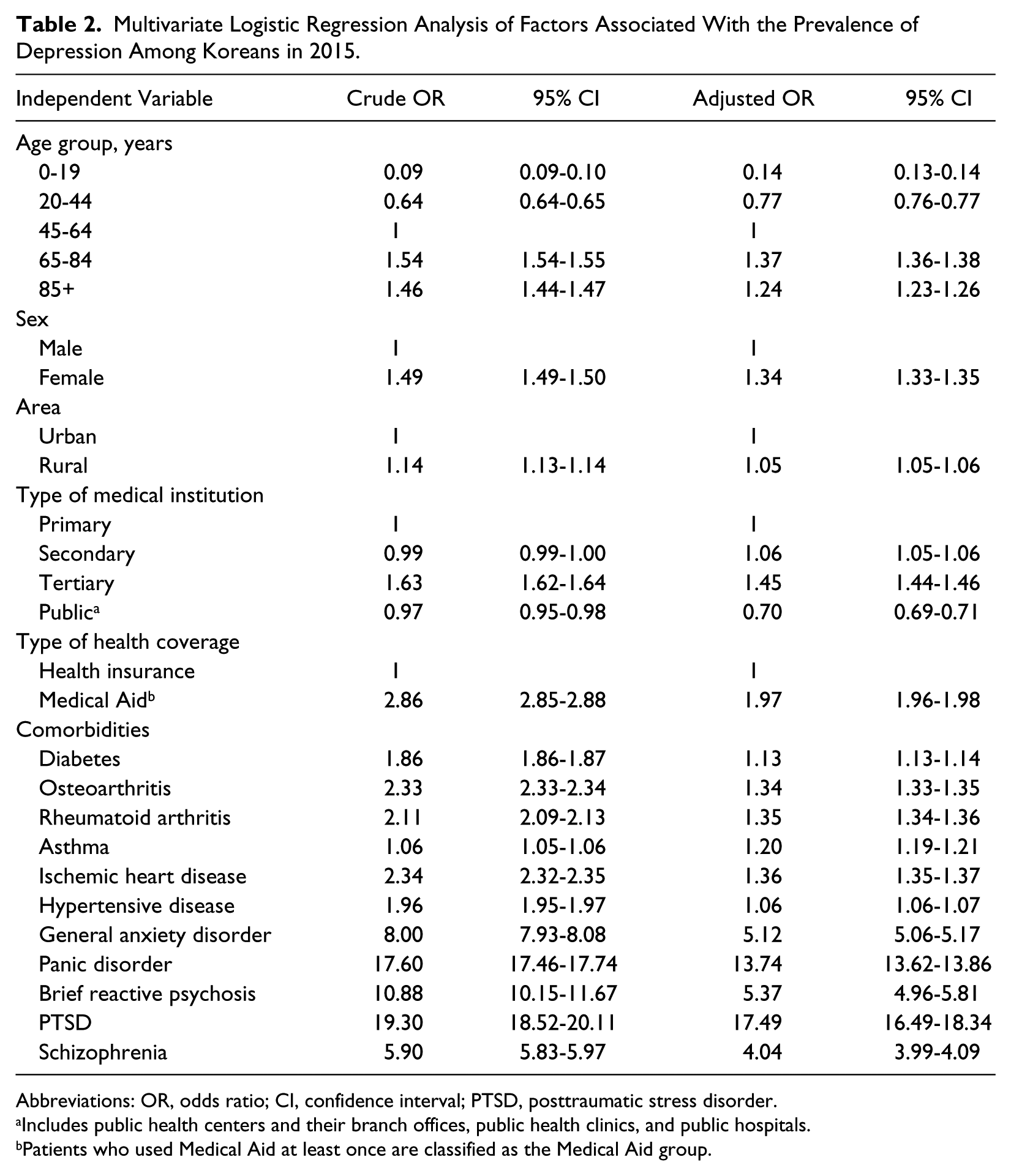
Abbreviations: OR, odds ratio; CI, confidence interval; PTSD, posttraumatic stress disorder.
Includes public health centers and their branch offices, public health clinics, and public hospitals.
Patients who used Medical Aid at least once are classified as the Medical Aid group.
Discussion
Based on the nationwide insurance claims data, the estimated prevalence of depression diagnosis in Korea was 2.51%. Therefore, the prevalence of depression diagnosis in Korea was lower than that in some other high-income countries: Greenberg et al reported that the prevalence of depression was 6.8% in American adults aged 18 to 64 years, while a cross-national survey revealed that the prevalence of major depressive episodes were 8.3%, 5.9%, and 3.0% in the United States, France, and Germany, respectively.10,11 The prevalence of depression reported in our study was lower than the previously reported rate of 3.1% in a Korean-based survey. 12 This may be attributable to some of the self-reporting patients not seeking medical care, suggesting that some cases may be undiagnosed and, thus, untreated.
The Medical Aid beneficiaries were twice more likely to be diagnosed with depression than the health insurance beneficiaries, according to a previous study, wherein socioeconomic status influenced the prevalence of depression. 13 Additionally, our findings imply that the coverage for low-income individuals could contribute to the increased access to medical care and, thus, increased diagnoses of depression, which is consistent with the results of a study in the United States. 4
Factors such as being female and rural residence were associated with higher odds of depression diagnosis, which was consistent with the findings of the previous research. 5 The higher risk of depression in individuals living in rural areas may be due to their low economic status. In addition, patients older than 84 years had a lower prevalence of depression diagnosis than those aged 65 to 84 years. This decline in the oldest group may be due to their lower mental health literacy and lesser use of mental health care.12,14 Approximately 60% of patients with depression and mood disorder in Korea do not seek medical services due, in part, to the low recognition rate of mental disorders. 12 The recognition rate of depression in Korea was even lower at 14% in the elderly. 14 Nonetheless, the higher likelihood of depression recognition in tertiary hospitals in our analysis raises the possibility that elderly patients visiting medical institutions for other chronic conditions were screened for diagnosis, as older patients with chronic conditions are more likely to choose tertiary institutions. 15 The higher odds of depression diagnosis at tertiary hospitals may be highly attributed to the specialization of the type of institution and the availability of psychiatrists.
This study estimated the prevalence of depression diagnosis in Korea based on a large sample (1.4 million). This study showed that low-income people with a medical assistance program were more likely diagnosed with depression, suggesting that ensuring access to mental health care will have significant public health implications in the vulnerable population in Korea as well as in countries in the Asia Pacific region with similar socioeconomic structures. However, it has potential limitations. First, given that some patients with depression chose not to seek medical care, our study based on claims data might have underestimated the prevalence. In addition, we excluded patients with veteran’s coverage from the analysis. This might have influenced the gender-based analysis, as patients with the coverage were predominantly males. However, the exclusion was intentional as the primary aim of this study was to compare the prevalence of depression between health insurance and Medical Aid beneficiaries.
Conclusion
In conclusion, the depression prevalence in Korea was 2.51%, which was considerably lower than the rates in the United States and some western European countries. After adjusting for age, sex, area, and medical institution type, results showed that patients with Medical Aid were more likely diagnosed with depression than those with health insurance. These findings will serve as a basis for the development of a depression management policy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.