
Abstract
Medical and long-term care costs are increasing all over the world. In this study, we investigated the characteristics of groups with high cost of medical and long-term care to define targets for curbing social security costs. As a result, for the population covered by the National Health Insurance, a large portion of medical costs were incurred for mental disorders, malignant neoplasms, and lifestyle-related diseases. For those covered by the Late Elderly Health Insurance System, most medical costs were incurred for lifestyle-related diseases, femoral fractures, neurological diseases, mental disorders, pneumonia, malignant neoplasms, and Alzheimer’s disease. From multiple regression analysis, the hospitalization days, use of advanced medical treatment, outpatient days, and high long-term care level influenced the increased costs. On the other hand, disease characteristics had only a very low effect. These findings suggest that the target population has complex medical and long-term care needs because they have multiple diseases.
Introduction
Failure in chronic diseases management is linked with higher risks of repeated hospital emergency admissions and poor care coordination, thus resulting in high medical costs.1-3 Appropriate diagnosis and coordinated care management of chronic diseases remain a challenging issue for any insurer. Recently, the control of ever-expanding medical and long-term care costs (ie, costs of support for persons who are ≥40 years old who need assistance with daily life care) is one of the major challenges in high-income countries.4,5 In the United Kingdom, a combined predictive model was developed based on hospitalizations, outpatients, and emergency care unit data to reduce medical costs. Based on this model, people are stratified by their risk of emergency hospitalization, whereas case management and disease management programs are provided for the high-risk group and intermediate-risk group, respectively. 6 In the United States, Accountable Care Organizations were introduced in a public medical insurance system in 2010 for specific people ≥65 years of age and patients on dialysis who incurred higher expenditure for health care. 7 It coordinated the groups of health care providers and medical institutions to reduce medical costs and provide high-quality care for people covered by Medicare. In this system, case management (disease management, coordination, arrangement of discharge and medical services, and aiding decision making) and process control are also implemented.
The percentage of the elderly population was as high as 26.0% in 2014, the highest rate among Organization for Economic Co-operation and Development (OECD) member countries.8,9 Advanced medical technology, easy access to health care information, and modern society increase the life expectancy. Aging people and the increase in the number of patients with cancer, cardiovascular diseases, and other chronic diseases contribute to rising medical costs. 10
Even in Japan, a system is required to assess the needs of individual patients, to allocate medical and long-term care resources properly, and to improve the quality of care. To curb health care costs in Japan, it is necessary to determine what kind of group should be targeted. Although there are reports of health insurance claims data analysis in and outside Japan, many of the articles analyzed disease-specific medical costs and contributing factors, such as cost analyses for metabolic syndrome, diabetes, cardiovascular disease, and mental disorders.11-14 To date, there are no reports that include the analysis of costs for long-term care, despite the increases in long-term care costs because of a higher necessity of long-term care associated with reliance on medical services and aging.
In this study, because of the increase in the number of patients with multiple chronic diseases, we decided that it was undesirable to limit to a specific disease and that long-term care costs should be analyzed. The study aims to clarify the characteristics of groups with high medical and long-term care costs to determine proper targets for controlling health care costs.
Methods
Study Design and Participants
A retrospective cohort study design was used in this study. As the model district, we chose Kure City (Hiroshima Prefecture, Japan) in which we have been working to reduce medical costs together with the medical insurer. The individuals analyzed in our study were the residents of Kure City who were covered by the National Health Insurance (NHI) and the Late Elderly Health Insurance System (LEHI). NHI includes persons who are ≤74 years old, individual business owners, those in the agriculture and fishing industries, short-time employees, and unemployed persons. LEHI covers persons aged 75 years or older as well as those who are 65 to 74 years old with specific impairments and other conditions. The long-term care insurance system supports the elderly in society as a whole. We identified the following conditions: (1) 65 years or older and in a state requiring long-term care or assistance in daily life, and (2) those aged 40 to 64 years with specific diseases requiring long-term care and support (such as end-stage cancer, rheumatoid arthritis, etc). 4
Kure City has a higher percentage of elderly people than other cities in Japan and has many medical institutions as per the population. 15 For this reason, the medical costs per insured person are higher than the national average. In the future, we will target Kure City to develop advanced case management as the model district.
Data Collection and Analysis
We analyzed 12 months’ health insurance claims data from April 2014 to March 2015. The following information was extracted and reconciled from data: age, sex, medical costs, diagnosis, duration of medical services, long-term care costs, and long-term care level. The health insurance claims have 3 different sheets for hospital inpatient services, outpatient services, prescriptions, and long-term care. When a patient receives a service, 1 sheet is issued monthly to him/her by each medical institution that he/she consults.
First, we examined variables related to the participants’ disease characteristics as an influencing factor for medical and long-term care costs. At this time, a medical cost grouping technique was used. 16 In Japan, details of the provided medical service are recorded in a database for health insurance claim data. However, in the data, disease names described in medical claims are not erased when the treatment finishes. Therefore, in this technique, a system that correlates all disease names with medications and medical treatment practices is constructed. Then, the hospitalization costs listed on health insurance claim sheets were linked with the disease primarily responsible for hospitalization and summarized. If there were multiple primarily diseases, costs were divided by the number of diseases and assigned equally to each disease. Outpatient services/prescriptions health insurance claim sheets were linked with diseases and summarized. Medical charges that were not linked to any disease were assigned to the primary disease requiring outpatient clinic visits. With regard to the Pareto analysis, after sorting the costs in descending order from high to low, the rate of accumulated costs to total costs was calculated. In addition, the percentage of the cumulative number of participants versus the total number of participants was calculated.
Next, for the participants with high medical and long-term care costs, we analyzed the disease characteristics, medical service usage, and long-term care level. Furthermore, multiple regression analysis was performed to clarify the influence of these factors on the medical and long-term care costs.
The insurer of Kure City provided the data, and analysis was conducted on an opt-out basis by us. Approval for this study was obtained from the ethics committee of Hiroshima University.
Results
Changes in Medical Costs and Disease Characteristics Accompanied by Aging
Comparison of Total Medical Costs, Hospitalization, and Outpatient Costs
The patients covered by NHI used about 20.6 billion yen, and those covered by LEHI used nearly 37.8 billion yen. With respect to hospitalization costs versus outpatient costs, patients covered by NHI and LEHI were 56.7% and 43.3%, and 50.0% and 50.0%, respectively. When scrutinizing the medical expenses per patient, we found that the patients covered by LEHI used 1.1 times the hospitalization costs of the patients covered by NHI and 2.0 times their outpatient costs.
Comparison of the Disease Characteristics by Medical Insurance
Table 1 shows the number of patients with diseases and the medical costs. In this study, the economic analysis of health care showed that the patients covered by NIH and LEHI, in terms of hospitalization and outpatient costs, the top 10 diseases accounted for 30.6% and 31.9%, and 38.7% and 42.6%, respectively. The leading diseases involving high health care costs were heart disease, cerebrovascular diseases, pneumonia, metabolic disorders, diabetes, kidney diseases, malignant neoplasms, bone fractures, neurodegenerative diseases, mental disorders, and Alzheimer’s disease.
Top 10 Diseases in Terms of Hospitalization Costs.
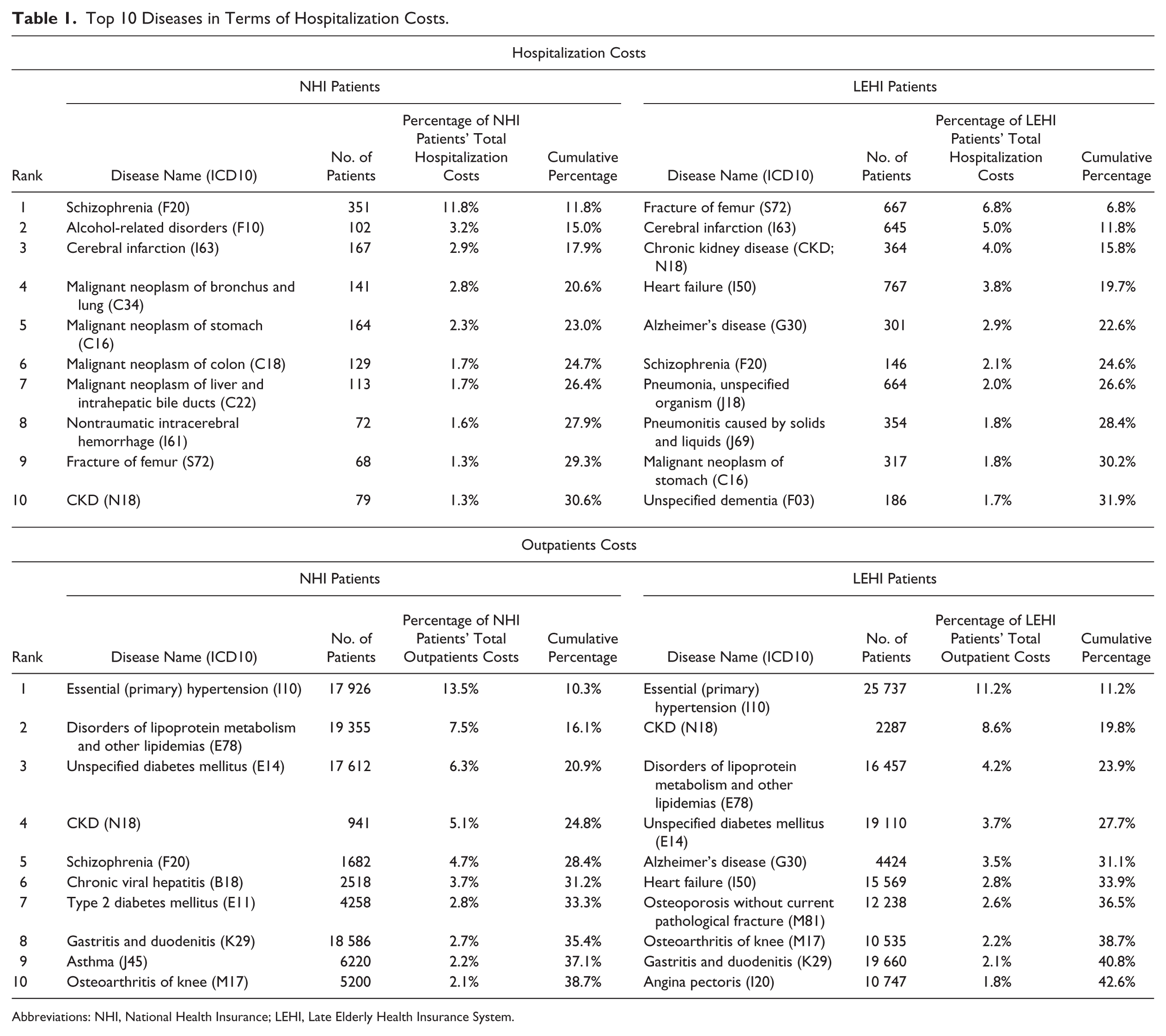
Abbreviations: NHI, National Health Insurance; LEHI, Late Elderly Health Insurance System.
Analysis of High-Cost Users of Medical and Long-Term Care Services
Identification of High-Cost Users of Medical and Long-Term Care Services
The Pareto analysis was conducted to show the relationship between costs and the number of people who used medical services and/or long-term care services for 12 months (Figure 1). From this analysis, it was found that 11 209 (25.1%) individuals used 80.0% of the total medical and long-term care costs of NHI and 12 710 (33.4%) individuals used 80.0% of the total medical and long-term care costs of LEHI. In this study, we defined them as high-cost users of medical and long-term care services. The Pareto chart of total medical care/long-term care costs were almost consistent with the Pareto chart of medical costs.
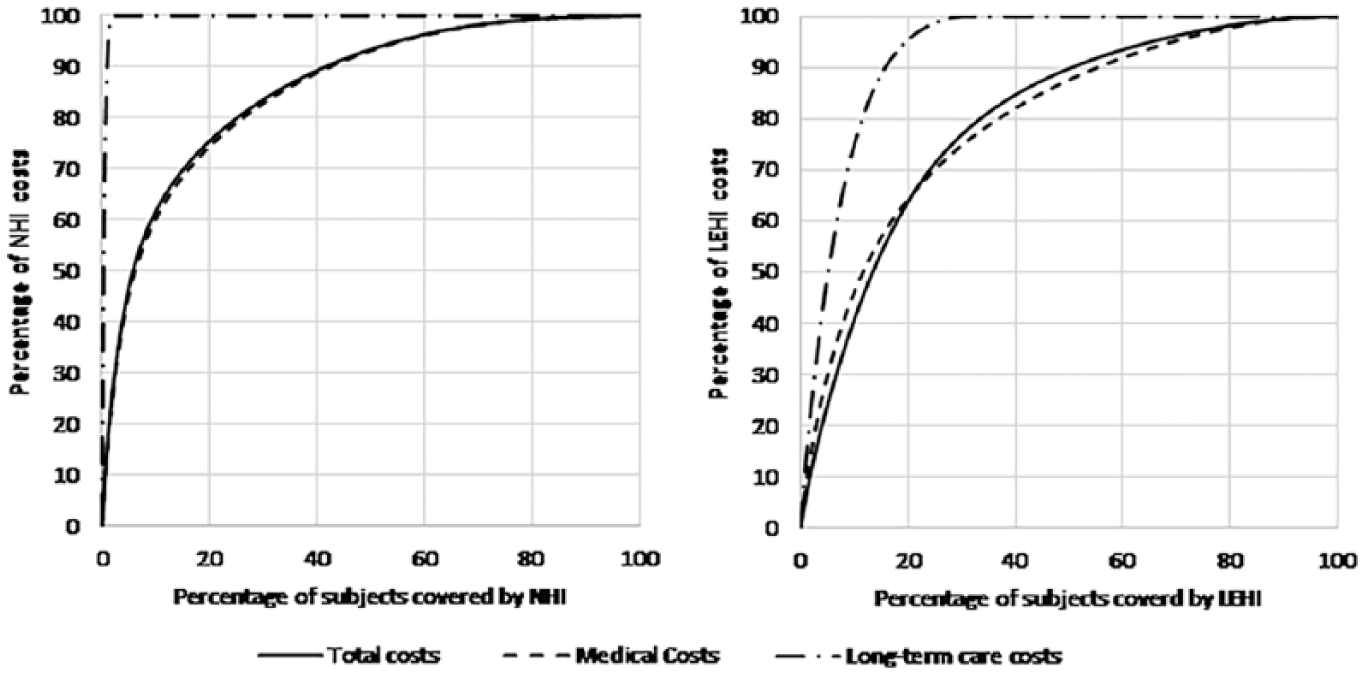
Pareto analysis of the distribution of total costs, medical costs, and long-term care costs. In total, 91 205 residents in Kure City were covered by the NHI and LEHI as of March 2015. Among them, 52 101 (57.1%) were covered by the NHI and 39 104 (42.9%) were covered by the LEHI. With regard to sex, 38 429 (42.2%) were males and 52 713 (57.8%) were females. When grouped by insurance and age, the 70- to 74-year-old group accounted for the highest percentage (14 004 persons [26.9%]) among the residents covered by the NHI. Furthermore, the 75- to 79-year-old group accounted for the highest percentage (13 966 persons [35.7%]) among the residents covered by the LEHI.
Analysis of the High-Cost Users of Medical and Long-Term Care Services
Outline of the high-cost users
With regard to sex, NHI (21 469 [44.1%] males and 27 249 [55.9%] females) and LEHI (14 169 [37.3%] males and 23 833 [62.7%] females) covered a significant number of high-cost users. For the high-cost users covered by NHI, the 55- to 64-year-old group accounted for the highest percentage (34 770 persons [71.4%]), followed by the 0- to 44-year-old age group (10 502 persons [21.6%]) and 45- to 74-year-old age group (3446 persons [7.1%]). For the high-cost users covered by LEHI, the 75- to 84-year-old age group accounted for the highest percentage (24 569 persons [64.7%]), followed by the 85 years and older (11 517 persons [30.3%]) and 65- to 74-year-old age group (1916 persons [5.0%]).
Analysis of factors influencing high-cost usage
With regard to factors influencing high costs, the variables related to the primary attribute were age and sex. The variables related to the disease characteristics were decided based on the medical cost grouping results. The variables associated with medical and long-term care services were the number of medical claim sheets, hospitalization days, usage of intensive care (emergency hospitalization fees, critical and emergency care unit fee, high-care unit fee, and stroke care unit fee), and outpatient days as well as high long-term care level.
As a result, the high-cost users’ characteristics were several medical claim sheets (frequent consultations and hospitalizations at multiple medical institutions), prolonged hospitalization, and usage of intensive medical treatment (Table 2). Furthermore, the high-cost users covered by LEHI had more multiple chronic diseases and required higher long-term care levels than the high-cost users covered by NHI.
Analysis of High-Cost Users and Factors Influencing Medical and Long-Term Care Costs.
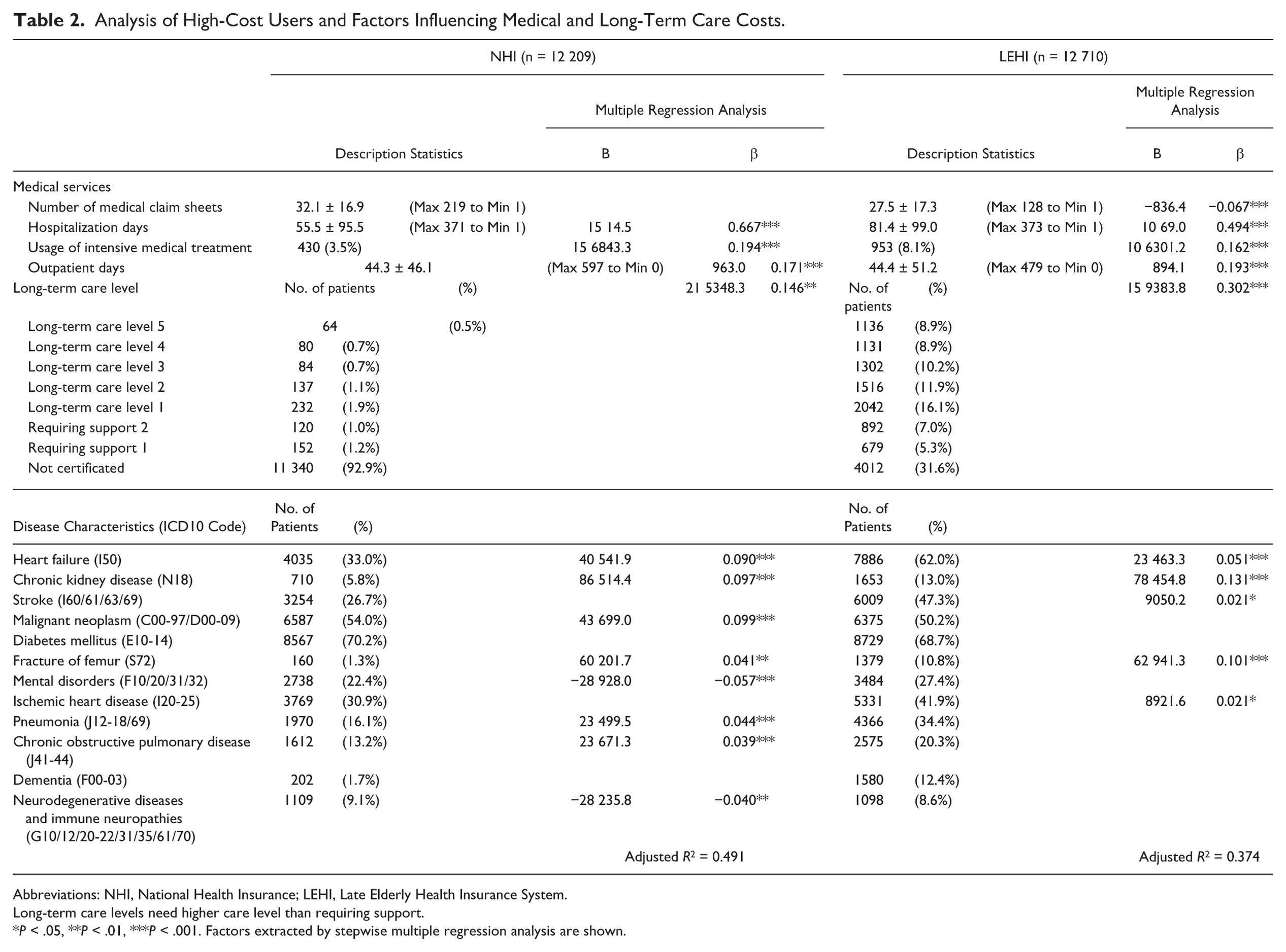
Abbreviations: NHI, National Health Insurance; LEHI, Late Elderly Health Insurance System.
Long-term care levels need higher care level than requiring support.
P < .05, **P < .01, ***P < .001. Factors extracted by stepwise multiple regression analysis are shown.
Regarding the percentage of patients with each disease among the high-cost users covered by NHI, diabetes mellitus accounted for the highest percentage followed by malignant neoplasm, heart failure, and ischemic heart disease. For the high-cost users covered by LEHI, diabetes mellitus accounted for the highest percentage followed by heart failure, malignant neoplasm, and stroke.
Subsequently, to clarify the influence of high costs, multiple regression analysis by the stepwise method was carried out (Table 2). We defined medical/long-term care costs as a dependent variable, and disease characteristics, medical services, and long-term care level as independent variables. We analyzed NHI and LEHI data separately because their base factors are different.
As a result, in both NHI and LEHI, the hospitalization days were the most influential factor in total costs (NHI: β = 0.667, P < .001; LEHI: β = 0.494, P < .001). The low-level influential factors’ effects were usage of intensive medical treatment (NHI: β = 0.194, P < .001; LEHI: β = 0.162, P < .001), outpatient days (NHI: β = 0.171, P < .001; LEHI: β = 0.193, P < .001), and high long-term care level (NHI: β = 0.146, P < .01; LEHI: β = 0.302, P < .001).
The coefficients of long-term care level, chronic renal failure, and femoral fracture were higher in the LEHI than in the NHI patients. However, although some diseases were significant, β was very low, and there was little correlation between the prevalence rate and total costs. When the collinear diagnosis was performed, multiple collinearity was not observed.
Discussion
In this study, we investigated the characteristics of patient groups with high medical and long-term care costs, to appropriately define targets for curbing health care costs in Japan. Our findings show that higher medical/long-term care costs were likely to be associated with multiple medical institution visits, extended periods of hospitalizations, and multiple chronic diseases. It also showed that a high long-term care cost was associated with elevated medical cost. Taken together, this analysis of health care costs offers a unique opportunity to both address questions about medical care and long-term care issues and improve coordination between the health sector and social welfare by directly applying our recommendations to structures committed to interventions. Multiple regression analysis indicated that the use of medical services and long-term care levels in individuals had a low to moderate effect, and the disease characteristics had only a very low effect. These findings suggest that the target individuals suffering from multiple diseases need complex medical and long-term care, making it difficult to explain their needs in terms of the diseases. Regarding social security factors, the number of clinic visits per capita in Japan is the second highest among OECD countries, and the number of hospitalizations is also very high. 5 This may be a common occurrence in Japan because the country offers universal health insurance coverage to its population, free access to the health care system, and minimal gatekeepers. Furthermore, it is well known that the cost of long-term care in Japan is likely to increase because of the rising numbers of elderly patients and patients with chronic diseases. 17 Our findings suggest that it is crucial to identify persons who are highly dependent on medical services (based on their use of medical services) along with those who require high-level long-term care, regardless of their disease types. This would help identify which care services would be of value for individuals who have high medical/long-term care costs.
Concerning the characteristics of groups with high medical costs outside of Japan, in the United Kingdom, people were stratified by risk of emergency hospitalization, a factor that profoundly influenced medical expenses. 6 These data showed that in the top 20% of persons ranked by risk, the percentage of emergency hospitalizations was 1.7 to 18.6 times higher than average, visits to outpatient departments were 1.9 to 5.8 times higher than average, and visits to emergency rooms were 1.4 to 8.5 times higher than average. 6 These high-risk persons had chronic diseases such as malignancies, asthma, cardiac diseases, diabetes, chronic obstructive pulmonary disease, or depression and were characterized by aging and use of multiple medications. In addition, research reports contributing to suppression of medical expenses by avoiding rehospitalization recommend early case management of patients with frequent hospitalization, elderly patients with acute myocardial infarction, and patients with specific diseases, including malignant tumors.18-21 In these studies, the targets for case management were characterized by the frequent use of medical/long-term care services; they also had chronic diseases that had higher risks of emergency hospitalization if appropriate disease management or coordinated services were not provided. These results are consistent with the findings of our analysis on the characteristics of persons who have high medical/long-term care costs.
This study has limitations. First, we could not analyze the relationship between medical costs and the end of life, which is an essential factor when analyzing the medical expenses of elderly individuals. 22 In the year 2010, a survey conducted in Japan reported that only 12.6% of the people died at home, which is a markedly low percentage when compared with the rest of the world.23-26 Furthermore, Tajika and Kikuchi 27 reported that 25.1% of the total hospitalization costs of the elderly are spent during the 12 months prior to death. 27 There are also available reports outside Japan on the relationship between medical costs and the end of life.28-30 Considering these existing findings, end-of-life medical costs should be included in future analyses as a factor that contributes to medical expenditure. It is worth noting that this study included only 1 local government, but useful suggestions for social welfare policies in the other Asian countries were obtained; this is because in this region, declining birthrate and aging population are progressing like in Japan. Further studies covering a wider area with many people may provide more suitable suggestions. In addition, close coordination between social welfare and the health sector is needed to further deeply examine this issue. Second, although the characteristics of patient groups with high medical and long-term care costs were clarified, the individual risks could not be identified. Analysis of the individual risk was beyond the scope of this initial investigation. This limitation will be addressed in our future analysis.
Finally, the public health implication of our findings can also be discussed in relation with the required support for the groups with high medical and long-term care costs in Japan. Although Japan has a public long-term care insurance system with care managers, most of these care managers are positioned as welfare workers and cannot coordinate services that involve disease management. In addition, medical remuneration as incentives for disease management is lower for outpatient treatment than inpatient treatment, and there is a shortage of skilled professionals who can provide appropriate services. For those with complicated medical care and long-term care needs like the participants in this study, we recommend support that can prevent hospitalization by case management and urge that home care continuation is useful.
This study was designed to investigate the characteristics of patient groups with high medical and long-term care costs, and we look forward to reconsidering the results in the future.
Conclusion
In this study, we investigated the characteristics of groups with high medical and long-term care costs. It was found that for the patients covered by NHI, tremendous medical costs were incurred for mental disorders, malignant neoplasms, and chronic diseases such as cerebrovascular disease, kidney disease, and heart disease. For the patients covered by LEHI, high medical costs were incurred for lifestyle-related diseases, femoral fractures, neurological diseases, mental disorders, pneumonia, malignant neoplasms, and Alzheimer’s disease. Furthermore, as the result of multiple regression analysis, it was found that medical services and long-term care level had a moderate to low effect, and disease characteristics had only a very low effect.
Footnotes
Acknowledgements
We thank Kure City for providing us the data and Data Horizon Corporation for helping us with processing health insurance claim sheets freely.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.