
Abstract
In Cambodia, HIV prevalence at 4% remains high among people who use drugs (PWUD). Complex and overlapping risk behaviors may enhance sexual transmission risk beyond PWUD. This study, therefore, aims to assess the factors associated with sexual risk behaviors among PWUD. Respondent Driven Sampling was used to recruit 1626 PWUD. Univariate and multivariate logistic regression analyses were used to identify factors associated with transmission risk including that high mental disorder scores were a strong predictor of sexual risk behaviors (odds ratio [OR] ranged from 1.9 to 2.8). Factors associated with sexual risk behaviors varied by gender: for men, these included geographical regions, non-married status, and heroin use; and for women, factors were age ≤20 years (OR = 5.4), living with friends (OR = 6.4), living in Central coastal region (OR = 6.1), and heroin use (OR = 4.8).
Keywords
Introduction
In the mid-1990s, Cambodia struggled with one of the fastest growing HIV epidemics in Asia. In the past 15 years, however, the epidemic was successfully contained through effective HIV prevention and control programs and policies. 1 HIV prevalence among the adult population aged 15 to 49 years declined from 1.3% in 2001 to 0.6% in 2015. 2 Nonetheless, the burden of HIV epidemic among key populations remains high compared with the general population. 3 These include female entertainment workers (FEWs), men who have sex with men (MSM), and people who use drugs (PWUD) defined as those who have used illicit drugs (heroin, amphetamine, methamphetamine [yama, ice], inhalant, marijuana, cocaine, and others) across routes of administration.
The burden of drug use varies across different key population groups; it is estimated that 19% of MSM and 11% of FEWs regularly use drugs. 4 A 2007 assessment in Phnom Penh found that risk factors for HIV among people who inject drugs (PWID) seemed to be not only injecting related behaviors, but also the sexual behaviors including having multiple sexual partners and inconsistent condom use. 5
According to the 2012 Integrated Biological and Behavioral Surveillance (IBBS) among drug users, the estimated population size of PWUD in the past 12 months is between 12 000 and 28 000, of whom the PWID range from 1200 to 2800. The estimated HIV prevalence was about 4.0% among PWUD and 24.5% among PWID. 6 Exposure to HIV through sharing injecting equipment and practice of unprotected sex was associated with HIV infection among PWUD and PWID. 6
While there have been studies identifying the main factors associated with high-risk sexual behaviors among FEWs and MSM in Cambodia,7,8 no peer-reviewed studies have examined sexual behaviors and their determinants among PWUD. There have been several reports on factors associated with HIV transmission among PWUD in the regional and global literature,9-12 but these may differ in the Cambodian context. Understanding this will inform the development of comprehensive HIV prevention and harm reduction programs for PWUD to address not only drug-related behaviors but also sexual behaviors. Therefore, this article aims to identify the factors associated with practice of sexual risk among PWUD in Cambodia.
Data Source and Methods
Study Sites and Sampling Method
This study analyzes data from the IBBS 2012. It is a part of the HIV surveillance program conducted in 9 out of 25 provinces in Cambodia in June 2012 by the National Center for HIV/AIDS, Dermatology and STD (NCHADS) in collaboration with National Authority for Combating Drugs (NACD) and KHANA, a nongovernmental organization (NGO) working on HIV, drug use, and economic development. 6 It was estimated that the number of PWUD in the selected 9 provinces might represent about 85% of all PWUD in Cambodia. 6
A total of 1626 participants were recruited using Respondent Driven Sampling, a probability network and referral approach to sampling often used to access hard-to-reach drug users. 13 Four seeds were selected in each province to fill each cell in the matrix of 2 variables, gender (male vs female) and type of drug use (injecting vs non injecting), for a total of 36 seeds. Mapping exercises and input from local NGOs working with PWUD were used to identify the seeds. Each enrolled participant (a seed) was then provided 2 study coupons for recruiting their network members. The sample was generated by providing each seed with study coupons to give to 2 individuals from their network for an incentive for enrollment in the study to be redeemed at the research site. Seeds were also provided incentives for each person that enrolled with one of their coupons. The seeds that were provided study coupons for 2 of their network members representing the second recruitment “wave.” This process for coupon distribution was continued up to 4 to 5 waves. Before the interview, a screening process was made to ensure that the participants were eligible. All coupon holders had to meet the following criteria for enrollment: must be 15 years of age or older, current or past drug use in the past 12 months assessed by self-report, and have adequate conscience for oral communication in Khmer, the native language of participants.
Interviewer’s Training and Data Collection
The interviewers and supervisors were trained in the recruitment process, sampling, informed consent procedures, and questionnaire administration. After obtaining informed consent, interviewers administered the gender-matched and face-to-face interview using a questionnaire developed based on the version used in previous IBBS to assess trends in risk behaviors. 14 Each participant received US$1 as the primary incentive after completing the interview and donating about 5 mL of blood. Another US$1 was provided for successfully recruiting another participant.
Outcome and Predictor Measurements
For men, there were 2 outcome variables: (1) report of transactional sex partners in the past month; (2) report of inconsistent condom use with transactional sex partners in the past 12 months. For women, the outcome variables were the following: (1) report of transactional sex partners in the past month; (2) report of inconsistent condom use with casual partners in the past 12 months. A transactional sex partner was defined as a sexual partner whom a person has sex involving exchange of money or drugs. A casual partner was defined as a sexual partner whom a person is not living with or does not have sex with for money or drugs.
Independent variables included sociodemographic characteristics such as age, marital status, educational level, living arrangement, and geographical region. The geographical region was 9 provinces grouped into 3 regions: Southern region (Kampong Cham, Prey Veng, and Svay Rieng), Central coastal region (Phnom Penh, Kampong Speu, and Sihanouk Ville), and Northern region (Battambang, Banteay Meanchey, and Siem Reap).
Drug-using behaviors were assessed by asking about initial age of drug use, different types of drug use in the past 12 months, report of ever injecting drug, and frequency of sharing needle and syringes in the past month.
The type of drugs used in the past 12 months were grouped as stimulant methamphetamine (ice, ecstasy, yama), amphetamine, cocaine, marijuana, heroin, and inhalant.
HIV knowledge was assessed using 5 basic questions: 4 were about transmission mode of HIV and 1 was physical appearance indicating HIV status. A score of 0 was designated for a wrong answer or reported as unknown and 1 for the correct answer. Finally, the total score was added up and classified into 2 levels as having high HIV knowledge (score of 5) and low HIV knowledge (score <5). For HIV testing, the participants were asked to report their experience with having HIV testing in the past 12 months.
Mental health was measured using 10 standard questions from a distress scale, based on the Kessler Psychological Distress Scale (K10). 15 The score in each question was ranged from 0 (normal mental health condition) to 5 (severe mental health condition). Then, the total score was summed up and classified into 4 levels of mental health conditions: well-being (<20), mild mental disorders (20-24), moderate mental disorders (25-29), and severe mental disorders (≥30). 15
Statistical Analyses
We used STATA 14 (Stata Corp, College Station, TX) to analyze the data. The descriptive statistics were used to describe sociodemographic and behavioral characteristics of the study population in terms of frequency, mean (median), and proportion. The variables included sociodemographic characteristics, HIV-related sexual behaviors, drug-using behaviors, HIV knowledge, HIV testing, and mental health.
Logistic regression was used to identify factors significantly associated with the sexual risk behaviors. Only those who were sexually active (defined as those who reported ever have had sexual intercourse) were included in the regression analysis. All covariates with P value ≤.20 in univariate analyses were included in the multivariate logistic model.16,17 Variables of theoretical importance and potential confounders were also included in the final model regardless of their significance levels in univariate analysis. Then, a multivariate logistic regression model was applied to determine the independent associations between the determinants and the sexual risk behaviors. Different models were created for men and women separately.
The survey protocol and verbal consent sheets were reviewed and approved by the National Ethics Committee for Health Research (NECHR), Cambodia’s Ministry of Health in 2012 (111-NECHR 2012). All study participants provided verbal informed consent.
Results
Sociodemographic Characteristics and Drug-Using Behaviors
Of 1626 PWUD, 82.2% were men and 17.8% were women. For men, the mean age was about 25 years (median = 24.0 years), 2 years younger than women (median = 27.0 years). The proportion of non-married male and female PWUD was 59.5% and 17.0%, respectively. More than half of men but only one quarter of women completed at least secondary education (≥7 years of schooling); close to one third of women reported no education at all. While about 57% of men but only 15% of women reported living with parents, more than half of women reported living with friends/others.
Regarding the drug use, the mean age of first drug use for men was 19 years (median = 18.0 years), which was around 4 years younger than that of female PWUD with mean of 23 years (median = 22.0 years). In the past 12 months, most of men and women reported using ice or amphetamine and yama, while less than 10% reported heroin use. Among those who injected drugs, about 49% of male and 31% of female PWID reported sharing needles and syringes sometimes in the past month (Table 1).
Sociodemographic Characteristics and Drug-Using Behaviors of PWUD.
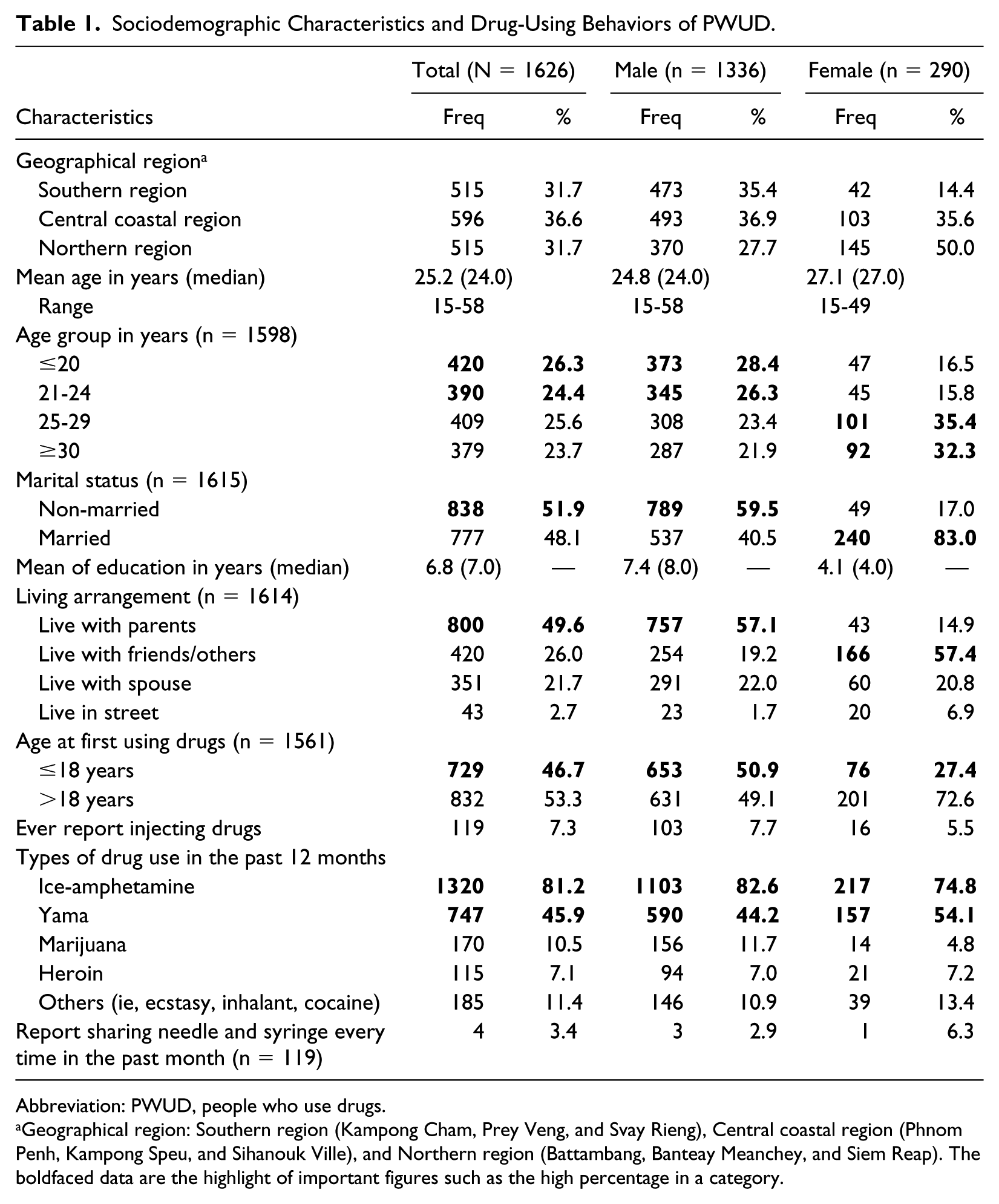
Abbreviation: PWUD, people who use drugs.
Geographical region: Southern region (Kampong Cham, Prey Veng, and Svay Rieng), Central coastal region (Phnom Penh, Kampong Speu, and Sihanouk Ville), and Northern region (Battambang, Banteay Meanchey, and Siem Reap). The boldfaced data are the highlight of important figures such as the high percentage in a category.
HIV Risk Behaviors, Knowledge, and Mental Health
For men, about 60% (n = 793) reported transactional sex in the past month; of those, 46% reported inconsistent condom use with transactional sex partners in the past 12 months. Almost of all women who were sexually active, 89.7% (n = 145) reported having transactional sex in the past month. Of 126 women having casual partners, around 18% reported inconsistent condom use with these partners. With regard to HIV awareness, only one third of men and nearly half of women were defined as having high knowledge. Finally, about 44% of men and 49% of women were defined as having mental health disorders ranging from mild to severe (Table 2).
HIV Risk Behaviors, Knowledge, and Mental Health Disorders.
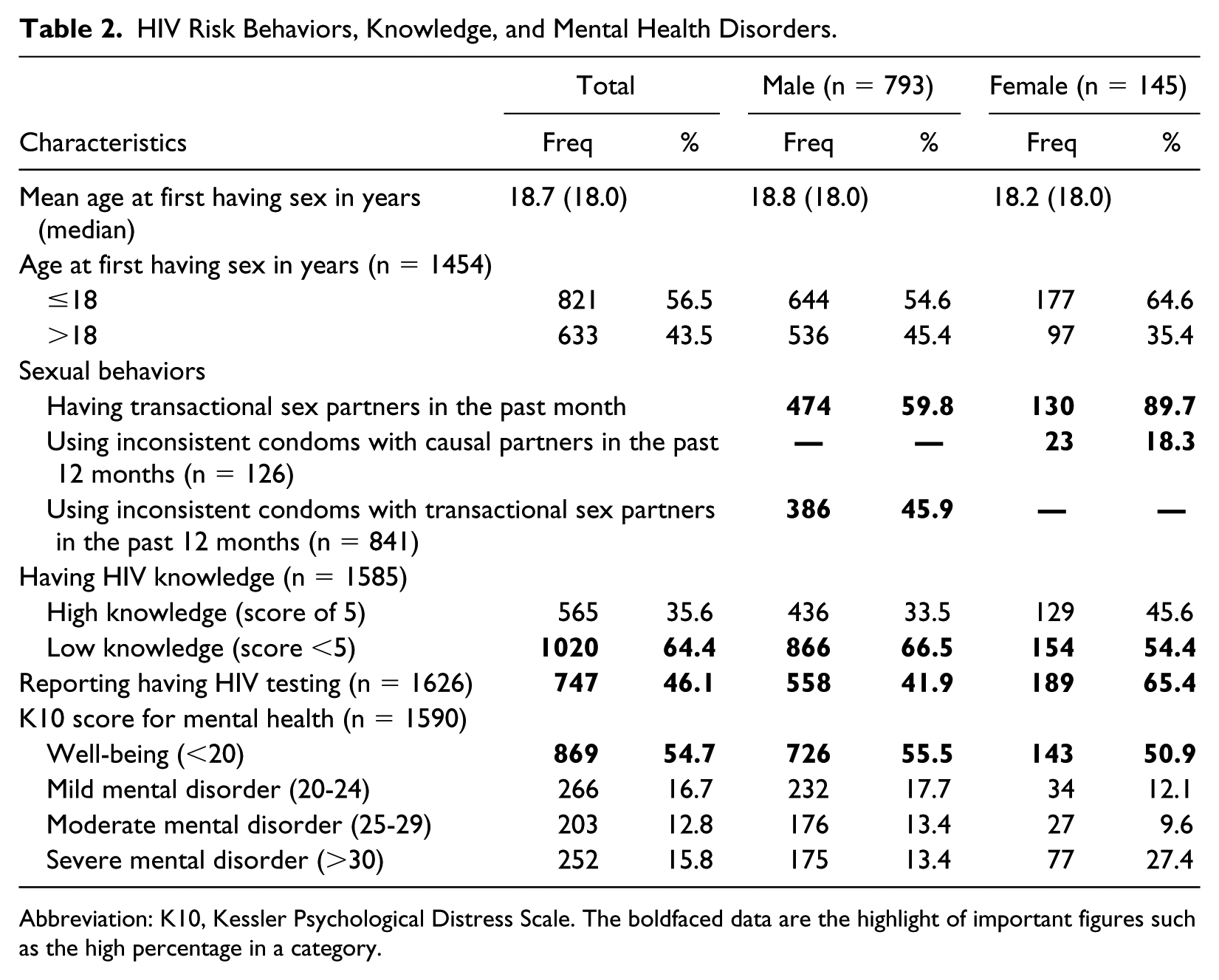
Abbreviation: K10, Kessler Psychological Distress Scale. The boldfaced data are the highlight of important figures such as the high percentage in a category.
Factors Associated With Sexual Risk Behaviors Among Male PWUD
Factors Associated With Having Transactional Sex Partners in the Past Month
In univariate analyses, the following factors were found to be associated with males reporting transactional sex in the past month: non-married (odds ratio [OR] = 2.7, 95% confidence interval [95% CI] = 2.0-3.6), age ≤20 years (OR = 2.5, 95% CI = 1.6-4.0), 21 to 24 years (OR = 1.9, 95% CI = 1.3-2.8), recent heroin use (OR = 0.5, 95% CI = 0.3-0.9), and recent stimulant drug use (i.e. ice, amphetamine, cocaine, ecstasy, yama) with OR = 2.6 (95% CI = 1.0-6.7). Those reporting first using drugs at the age ≤18 years had higher odds of having transactional sex partners than those who started using at an older age (OR = 1.5, 95% CI = 1.1-2.0). Significantly more of those with high HIV knowledge (OR = 0.7, 95% CI = 0.5-1.0) and severe mental disorders (OR = 1.8, 95% CI = 1.2-2.8) also reported transactional sex. In the final multivariate model, only 3 covariates remained independently statistically significant after controlling for age, geographical region, age at first using drugs, using stimulant drugs, and having high HIV knowledge: being unmarried (adjusted OR [AOR] = 2.8, 95% CI = 2.0-3.7), the use of heroin (AOR = 0.5, 95% CI = 0.3-1.0), and severe mental disorders (AOR = 1.9, 95% CI = 1.2-3.0; Table 3).
Factors Associated With Sexual Risk Behaviors Among Male PWUD.
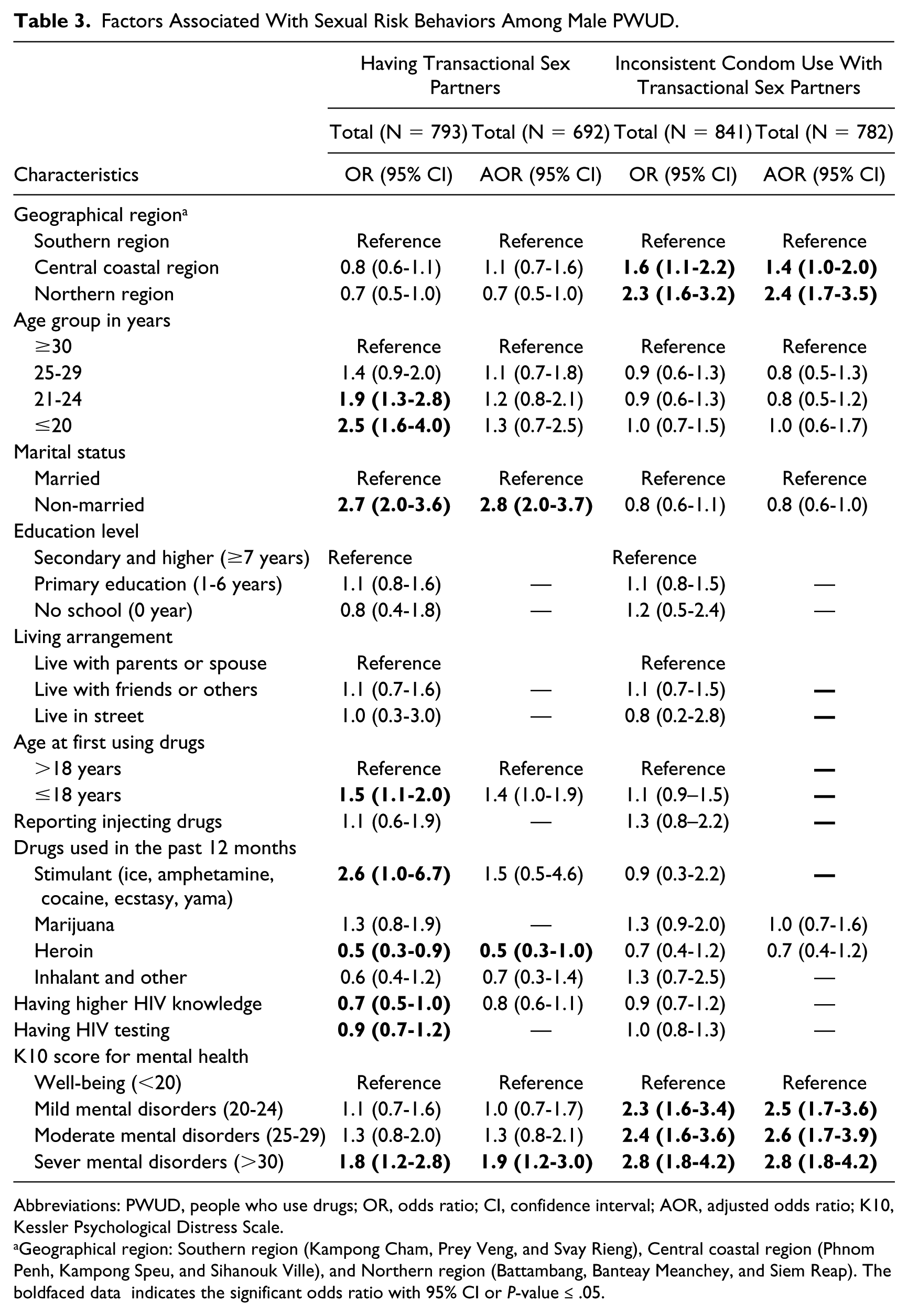
Abbreviations: PWUD, people who use drugs; OR, odds ratio; CI, confidence interval; AOR, adjusted odds ratio; K10, Kessler Psychological Distress Scale.
Geographical region: Southern region (Kampong Cham, Prey Veng, and Svay Rieng), Central coastal region (Phnom Penh, Kampong Speu, and Sihanouk Ville), and Northern region (Battambang, Banteay Meanchey, and Siem Reap). The boldfaced data indicates the significant odds ratio with 95% CI or P-value ≤ .05.
Factors Associated With Inconsistent Condom Use With Transactional Sex Partners in the Past 12 Months
The factors found to be significantly associated with inconsistent condom use with transactional sex partners in the past 12 months in univariate logistic regression were Central coastal region (OR = 1.6, 95% CI = 1.1-2.2), Northern region (OR = 2.3, 95% CI = 1.6-3.2), severe mental disorders (OR = 2.8, 95% CI = 1.8-4.2), moderate mental disorders (OR = 2.4, 95% CI = 1.6-3.6), and mild mental disorders (OR = 2.3, 95% CI = 1.6-3.4). However, in the multivariate model, only geographical region and mental health disorders remained statistically significant after controlling other covariates (ie, age, marital status, using marijuana, and inhalant): Central coastal region (AOR = 1.4, 95% CI = 1.0-2.0), Northern region (AOR = 2.4, 95% CI = 1.7-3.5), severe mental disorders (AOR = 2.8, 95% CI = 1.8-4.2), moderate mental disorders (AOR = 2.6, 95% CI = 1.7-4.0), and mild mental disorders (AOR = 2.5, 95% CI = 1.7-3.6; Table 3).
Factors Associated With Sexual Risk Behaviors Among Female PWUD
Factors Associated With Having Transactional Sex Partners in the Past Month
Factors found to be associated with having transactional sex partners in the past month in univariate analysis were reporting living with friends/others instead of family (OR = 5.7, 95% CI = 1.7-18.7) and first using drugs at age ≤18 years (OR = 0.3, 95% CI = 0.1-0.9). However, in final multivariate model, women who lived with friends/others (AOR = 6.4, 95% CI = 1.8-22.3) and women living in Central coastal region (AOR = 6.1, 95% CI = 1.1-35.8) were independently associated with having transactional sex partners after controlling for age, marital status, and first experience of using drugs (Table 4).
Factors Associated With Sexual Risk Behaviors Among Female PWUD.
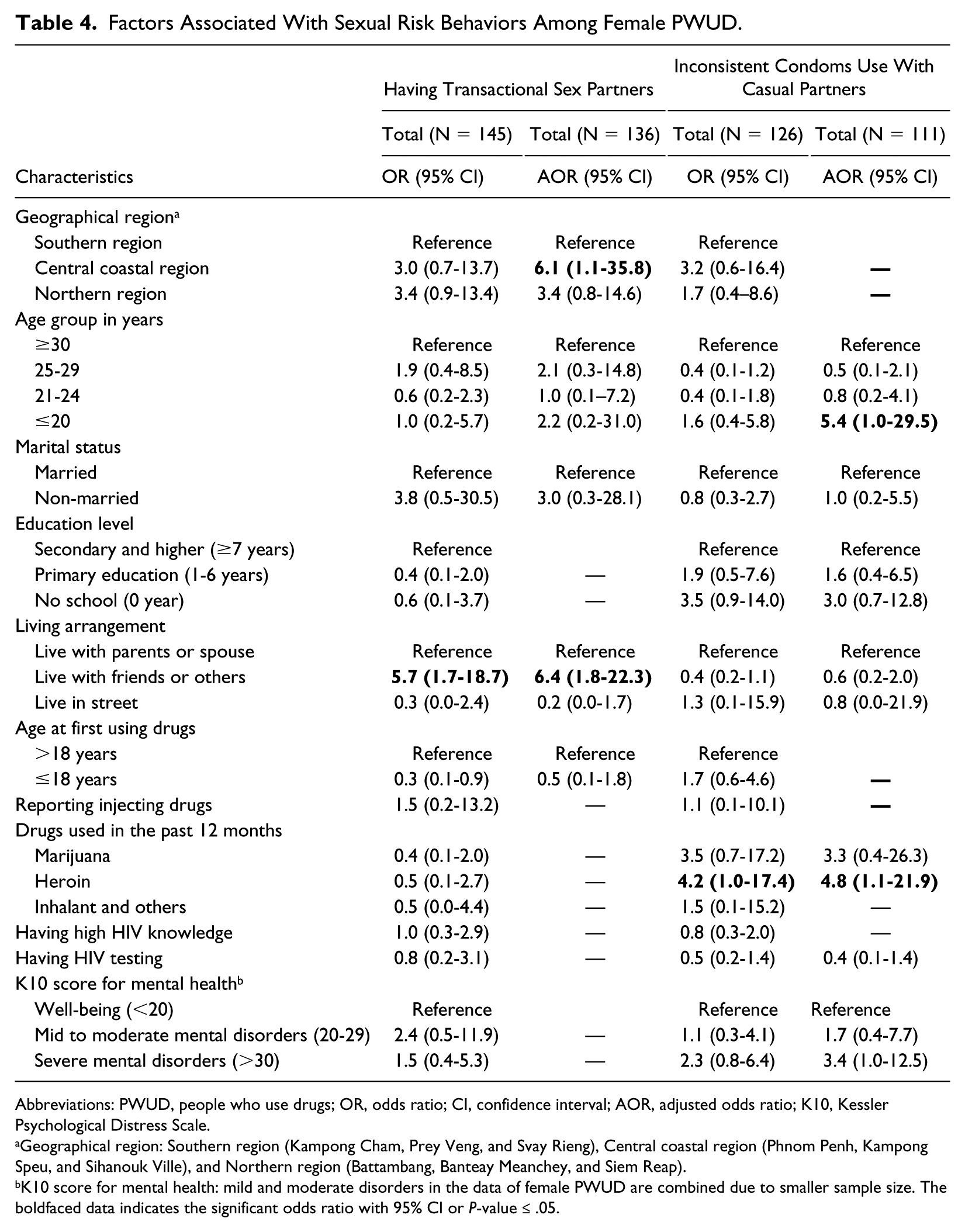
Abbreviations: PWUD, people who use drugs; OR, odds ratio; CI, confidence interval; AOR, adjusted odds ratio; K10, Kessler Psychological Distress Scale.
Geographical region: Southern region (Kampong Cham, Prey Veng, and Svay Rieng), Central coastal region (Phnom Penh, Kampong Speu, and Sihanouk Ville), and Northern region (Battambang, Banteay Meanchey, and Siem Reap).
K10 score for mental health: mild and moderate disorders in the data of female PWUD are combined due to smaller sample size. The boldfaced data indicates the significant odds ratio with 95% CI or P-value ≤ .05.
Factors Associated With Using Inconsistent Condoms With Casual Partners in the Past 12 Months
In univariate logistic regression, using heroin (OR = 4.2, 95% CI = 1.0-17.4) was the only covariate found associated with inconsistent condom use with casual partners in the past 12 months. Nevertheless, in the final model, after controlling marital status, education level, living arrangement, using marijuana, mental health disorders, and having HIV testing, the strongest associations with the inconsistent condom use with causal partners were heroin use (AOR = 4.8, 95% CI = 1.1-21.9) and younger age ≤20 years (AOR = 5.4, 95% CI = 1.0-29.5; Table 4).
Discussion
Using data from a surveillance survey conducted in multiple provinces in Cambodia among PWUD, we identified very different patterns of factors associated with sexual risk behaviors by gender. For men, the main factors associated with sexual risk behaviors are marital status (non-married), geographical region, heroin use, and severe mental disorders. For women, however, younger age (≤20 years), living with friends/others instead of family, living in Central coastal region, and heroin use are the factors independently associated with sexual risk behaviors.
For men, our study demonstrated that non-married PWUD were more likely to have 3 times odds to report transactional sex compared with married drug users. A possible explanation is that sexually active and non-married men seemed to utilize transactional sex to fulfill their physical, psychological, and sexual needs. Another explanation is that married men may have less discretionary income to spend on sex as their spouse and family may take up most of their resources and after drug use little is left. Similar results have been reported in China and Vietnam. However, in a study in Vietnam, the significant level of the association of marital status was not as strong as ours.12,18
For women, living with friends/others was significantly associated with having transactional sex partners. On the basis of sociocultural norms in Cambodia, women who leave their families to live with friends/others before marriage tend to represent a nonnormative pattern and as such those who use drugs may seek more lenient housing arrangements where they have greater opportunity to engage in drug use or practice transactional sex partners lacking family control. 10 Similar findings were noted in Malaysia where parental bonding and connectedness were found to be protective factors against sexual risk activities among adolescents. 19 It is also possible that drug-using women share housing with other female drug users. In this situation, peer pressure to use drugs or sell sex may be an influence under these living arrangements.
Moreover, among women using heroin, there was more inconsistent condom use with casual partners reported. As previously reported, heroin users may use condoms inconsistently because they might find themselves too intoxicated to protect themselves during sexual intercourse. 20 Heroin may also create extreme needs for drug driven by its highly addictive properties, and as noted in China, this physical craving for the drug may compromise choices by addicts to protect themselves in the context of sex. 21
We were not surprised to find that PWUD living in Central coastal region and Northern region appeared to have higher HIV-related risks compared with those in the Southern region. In the Cambodia, the Northern and Central coastal regions are known as high economic hubs as well as tourist destinations thus having more entertainment facilities (ie, karaoke, night clubs, hotels, and guesthouses) than other parts of the country. Thus, drug users living in these regions might easily access those facilities and have more opportunities to engage in sexual risk activities including transactional sex. Furthermore, historically high HIV prevalence among entertainment workers and the general population in these regions reflects a long history of local HIV transmission activities. 22
Our findings reveal that mental health disorders may have a dose-response association with HIV risk behaviors. This may suggest that individuals with severe mental disorders have difficulties in establishing stable social and sexual relationships. Risky sex might be used to relieve the tension or even served as self-medication. 23 It may also reflect a lack of personal control and ability to judge what behaviors may be risky. This may result in sexual abuse and vulnerability to practice risky sexual behaviors. Other studies in the United States, Taiwan, and Uganda have also indicated a significant association between depressive symptoms and the practice of unprotected sex among male adolescents and the adult general population.24-26
Of note is our finding among male PWUD that few reported both heroin use and transactional sex. This may be due to the effect of heroin on lowering the levels of sex hormones, which might be associated to sexual dysfunction. 27 This interpretation was supported by the evidence from several studies showing the high prevalence of sexual dysfunction among the heroin dependents compared with non-heroin users.28,29
This study has several limitations. First, the survey asked for reports of some experiences for recall periods as long as the past 12 months. Thus, the recall bias might occur, and this may be particularly problematic for drug users whose memory may be impaired by substance use. This bias may be relatively minor since the recall of HIV risk behaviors in the past months among drug users was found to be reliable in the previous study. 30 Second, social desirability may have influenced reports of personal and sensitive information, particularly around drug use and sexual behavior. However, such bias may have been minimized by using a validated questionnaire and offering sufficient and standardized trainings to interviewers. 31 In addition, because our study population did not include PWUD living in the settings such as prisons, methadone treatment centers, and rehabilitation centers where their responses could have consequences on their care or be reported to those with authority and control over them, the bias may have been minimized.
Another limitation is that unprotected sex with high-risk partners was measured differently for men and women. While men were asked about their practice of transactional sex and condom use with such partners, women were asked about transactional sex and their condom use with casual partners, not transactional partners. This makes the comparison of high-risk condomless sex among PWUD not directly comparable by gender.
Despite these limitations, this is the first nationwide survey among PWUD in Cambodia using the Respondent Driven Sampling method developed by the collaboration between NCHADS, NACD, UNAIDS, and international and local NGOs. It offers the resourceful findings of risk factors associated sexual risk behaviors of PWUD in Cambodia context, which could be used to develop comprehensive HIV prevention and harm reduction programs.
Further studies should focus on the sexual risk behaviors among PWUD in both community and rehabilitation centers so that sexual risk behaviors of drug users could be compared in the different settings and living conditions. In future studies, condomless sex with transactional partners should be measured for females as well as males so that high-risk condomless sex among PWUD could be directly compared by gender. The influence of peer pressure on sexual risk behaviors among PWUD should be covered in future studies, since this might be a potential determinant of sexual risk behaviors among non-married men and women living with friends and others.
Conclusion
Our study indicates many Cambodian male and female PWUD practice HIV sexual transmission behaviors, especially non-married men and women living with friends/others and those living in Central coastal region. Strong associations between sexual risk behaviors and severe mental disorders and geographical region (Northern and Central coastal region) were found for male PWUD. While fewer male heroin users seemed to report transactional sex partners, we found more female heroin users reporting inconsistent condom with casual partners. HIV interventions for drug users should be more targeted at unmarried men and women, those living in Central coastal region as well as women living outside of family settings. HIV prevention programs should consider incorporating mental health services for PWUD to lessen transmission risk and expanding access to an integrated approach to substance use and mental health treatment.
Supplemental Material
Supplementary_file_table_4 – Supplemental material for Factors Associated With Sexual Risk Behaviors Among People Who Use Drugs in Communities in Cambodia
Supplemental material, Supplementary_file_table_4 for Factors Associated With Sexual Risk Behaviors Among People Who Use Drugs in Communities in Cambodia by Chamnab Ngor, Heng Sopheab, Sovatha Mam, Pamina Gorbach and Chhorvann Chhea in Asia Pacific Journal of Public Health
Footnotes
Acknowledgements
We thank Prof John Kaldor, Dr Bradley Mathers, and Dr Kathy Petoumenos from Kirby Institute at the University of New South Wales for their support in scientific writing training, and Dr Ly Penh Sun, Director of National Center for HIV/AIDS, Dermatology and STD, Cambodia, for his administrative support for the study data.
Authors’ Note
The datasets used and analyzed in the current study are available from the corresponding author on reasonable request.
Author Contributions
HS and CC conceived and designed the study. CN and HS wrote the early draft of the manuscript; and SM was in charge of data management. PG contributed by providing and revising technical input, and proofreading the manuscript. CN was responsible for conducting the statistical analyses and data interpretation, and HS contributed to revising and finalizing. Other coauthors participated in interpretation and gave technical input. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: CN received financial support from the Fellowship in Field Research Training Program (FRTP) from Kirby Institute, the University of New South Wales.
Ethical Approval and Informed Consent
The survey protocol and verbal consent sheets were reviewed and approved by the National Ethics Committee for Health Research (NECHR), Cambodia’s Ministry of Health in 2012 (111-NECHR 2012). The verbal informed consent was taken for this study since the study population, people who use drugs (PWUD), were with low education with about 5 to 6 years of basic schooling. Therefore, their level of reading and writing were very limited. Our verbal informed consent sheet was conducted in Khmer, the native language of participants. After the consent process was explained, the study staff had to sign in the consent sheets and these sheets were kept for the proof of informed consent procedure for the supervisors and lead researcher. A participant could have a copy of the consent if he/she wished. The purpose of the study was clearly explained in detail in the consent. Privacy, confidentiality, and anonymity of the participants were ensured at all stages of data collection. Participants’ involvement in the study was voluntary. If they wished to withdraw their participation, they were informed they could do so at any time with no repercussions.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.