
Abstract
The aim of this study was to examine the impact of maternal education on child immunization uptake in Pakistan, both at individual and community levels. Pakistan Demographic and Health Survey data were used for analysis. Multilevel logistic regression was used to access the individual- and community-level factors associated with childhood immunization coverage. Out of 6765 children 2659 (39.3%) were fully immunized. Parents education, access to media, and wealth status have positive while ethnicity and working status of mother have a negative impact on the immunization uptake. In the community with a high percentage of educated mothers, the odds of immunized children were high (odds ratio = 1.43, 95% confidence interval = 1.14-1.80) as compared with communities with lower percentage of educated mothers. Moreover, significant variation was found in the likelihood of full immunization across communities. Both community- and individual-level factors have substantial impact on children immunization status. There is a need of improvement in maternal education, poverty alleviation, and removal of rural-urban disparities.
What we Already Know
Conventional multivariate logistic regression has been used to find the significant factors of child immunization uptake in Pakistan.
Only individual-level factors were considered in previous literature regarding Pakistan.
What This Article Adds
Using multilevel logistic regression this study finds the impact of maternal education and other factors both at individual as well as community-level factors.
This study highlighted vital variation between communities regarding maternal and other caring factors.
Exclusive role of educated mother for better child health care both at individual and community levels has been proved.
Introduction
Complete vaccination is among the most cost-effective public health interventions to decrease the global burden of vaccine preventable diseases. The Expanded Programme on Immunization, launched by the World Health Organization (WHO) in 1974, has made significant contribution in increasing vaccination coverage in low- and middle-income countries (LMICs). 1
Pakistan, by area, is the 36th largest nation in the world with a population of 207.8 million. 2 In Pakistan, the Expanded Programme on Immunization was launched in 1978, with the aim of protection against infectious diseases among children of age less than 1 year. Effective vaccination of children may reduce morbidity and mortality. According to the guidelines of WHO, at birth a child should receive a dose of Bacillus Calmette–Guérin (BCG) vaccine against tuberculosis and one dose of oral poliovirus vaccine. At sixth week three doses of DPT for the prevention of diphtheria, pertussis, and tetanus and at ninth month 1 dose of vaccine against measles. 3 These vaccines are recorded on a prescribed card provided by the health department. However, in Pakistan about 46% of the children were not fully immunized as on 2018. 4
The role of maternal factors as well as other socioeconomic and demographic factors for the improvement of child health in LMICs is well established.1,5 Additionally, factors such as media exposure, child’s place of birth (eg, health facility), and region of residence also influence the immunization coverage among children. 5 Existing literature, however, reveals that improved maternal education can positively affect the health outcome of family through balance of power, better understating of risks, and benefits associated with vaccination. 1 However, few studies showed nonsignificant relationship, 6 while some other showed a negative association. 7 One possible reason for this negative association might be the time given to the child for feeding and other caring activities, such as vaccination. Since educated mothers are involved in economic activities outside the household, they have less time available for their children, which adversely affects children’s health care (HC). 8 Moreover, in some societies, even an educated mother sometimes, could not properly care for herself as well as her child. The reason might be the patriarchal framework of family, which limits maternal autonomy in the household and other might be some cultural norms and barriers in different societies. These bounds on the educated mothers also increase the stress, which negatively affects her child’s well-being. 9 Hence, there is a need to unravel the importance of maternal education for LMICs countries, like Pakistan, and to discourage unnecessary limitations for mothers to better HC of her children. Furthermore, these controversial results, perhaps, enhanced the need of more research in these areas.
Improvement in child health was one of the Millennium Development Goals, and now it is one of the Sustainable Development Goals to be achieved by 2030. Pakistan did not reach the targeted figures of 52 deaths in children and 40 deaths per 1000 live births in infants but showed some improvements in achieving this goal. Child mortality has decreased from 117 deaths in 1990-1991 to 89 deaths per 1000 live births in 2012-2013, while in the case of infant mortality, the number of deaths decreased from 102 to 74 deaths per 1000 live births in the same period. 10 There were 54% fully immunized children in 2012-2013 as compared with 35% in 1990-1991; however, the coverage of polio vaccine remains similar in 2006-2007 and 2012-2013, particularly in case of first and second dose. 3
Although different studies had examined different factors associated with childhood vaccination in Pakistan,11 -13 the influence of community-level factors on the children’s vaccination coverage had received no attention. Multilevel regression modeling examined the effects of community level as well as individual-level factors simultaneously. 14 Therefore, this study aims to contribute to the literature by identifying factors affecting the vaccination uptake both at individual and community levels in Pakistan, using multilevel logistic regression modeling technique.
Methods
About the Data
Pakistan Demographic and Health Survey (PDHS) data for the year 2012-2013 was used for analysis. The PDHS data comprise a range of maternal and child health-related information. A sample of 14 000 households from 500 primary sampling units (252 rural and 248 urban), was selected using two-stage stratified sampling procedure. 3 A total of 14 569 eligible women of age 15 to 49 years were selected for interview and 13 558 were successfully interviewed from these selected households. These women contributed a total of 11 763 live born children within five years before the survey. However, the analysis in this study was limited to 6765 live born children of age 1 to 5 years. The children of age less than 1 year and whose information was not completed were excluded from the analysis. Immunization status of a child was determined from the vaccination card and in case of no card the mothers were asked to recall whether the child had received prescribed doses of all recommended vaccines (BCG 1 dose, polio 4 doses, DPT 3 doses, and measles 1 dose). 3
Variables
Response Variable
The response variable is considered as a binary variable that takes the value 1 if the child has received all doses of recommended vaccines and 0 otherwise.
Explanatory Variables
We have included explanatory variables for two stages. Individual-level (Level-1): Following variables were included at individual level: mother’s age (<20, 20-24, 25-29, and 30 years or older), mother’s education (no education, primary, secondary, and higher and above education), father’s education (no education, primary, secondary, and higher and above education), place of residence (rural/urban), and household wealth status was used as proxy for wealth index given in the survey data. This index was constructed using principal component analysis on the factors of household’s ownership of assets (such as bicycle, motorcycle, car, radio, television, etc), characteristics of dwellings (such as roof material, main floor material, type of toilet facility, water resource, etc). 15 The constructed wealth index is subsequently divided into 5 quintiles as poorest, poorer, middle, richer, and richest, access to media (watching TV frequently or not), sex of child (male/female), ethnicity (Urdu, Punjabi, Sindhi, Pushto, Balochi, and others), working status of mother is assessed through respondent’s self-reported indicator that whether she is currently working or not, age at first birth (<20, 20-29, and more than 30 years), birth gap, and order (a variable generated by merging 2 variables labeled as “Preceding birth interval” and “birth order” in the survey). The generated variable was categorized into 7 groups as: first birth, birth order 2 to 3 with birth gap (<24 months), birth order 2 to 3 with middle gap (24-47 months), birth order 2 to 3 with long gap (48 months or above), birth order 4+ with short gap (<24 months), birth order 4+ with middle gap (24-47 months), and birth order 2 to 3 with long gap (48 months or above). Since DHS data contain information of children aged 0 to 59 months (5 years or less) so we distribute age with a gap of 24 months (2 years), which is minimum birth spacing according to the WHO report. 16 All the base line categories of the explanatory variables both at individual and community level were selected as referent categories.
Community level (Level-2): Following Acharya et al 5 and Smith and Shively, 17 this study considered clusters or primary sampling units (PSUs) as proxies for the community level. These clusters or PSUs are administratively defined areas used as proxies for “neighborhoods” or “communities.” 18 Moreover, PSUs are small and fairly homogenous with regard to sociodemographic characteristics, wealth status, and living standard. They consist of one or more enumeration areas (enumeration blocks for urban and mouzas/Deh/villages for rural areas in our case), which are the smallest geographic units for which census data are available in Pakistan. 3 Following community-level variables were included in the analysis:
Mothers’ education in community defined as the percentage of mothers with secondary education in the community and categorized as low or high.
Hospital delivery defined as the percentage of mothers who delivered their child in a hospital and categorized as low or high.
Prenatal care by doctor defined as the percentage of mothers who received prenatal care by a doctor in the community and categorized as low or high.
Statistical Analysis
Keeping in view the hierarchical nature of PDHS data (children are nested in communities); a multilevel logistic regression model, with two levels, was used for the analysis. Multilevel regression modeling is among the widely used methods to investigate the community effects on individual outcomes. Moreover, it helps to correct within-communities correlation among individual observations as well as adjusts for standard errors, giving efficient estimates for both individual- and community-level variables. 18
Descriptive analysis was presented as a percentage frequency distribution of the response variable (fully immunized children) across all categories of the selected predictors. Bivariate association of the response variable across all the selected explanatory variables was checked using χ2 test. Three models were fitted in the analysis. Model 1 contains no explanatory variables (empty model) and only decomposes the total variance between individual- and community-level factors. Model 2 contains the individual-level determinants and allows the assessment of the relation of response variable to the individual-level factors. Model 3 contains both individual- and community-level predictors. This model allows the assessment of the net effect of the community-level factors above the individual-level factors.
The results of fixed effects (measure of association) for each of the models were expressed as odds ratios (ORs) with 95% confidence intervals (95% CI). The random effects (measures of variation) were expressed as intracommunity correlation (ICC). ICC measures the percentage variance explained by the community-level factors. It measures the correlation among observations within communities. The ICC was calculated by using the formula
where
The presence of multicollinearity among explanatory variables was checked by variance inflation factor (VIF). The smaller values of VIF (mean value of VIF <10) indicates the absence of multicollinearity among the explanatory variables. 14 Akaike information criterion (AIC) and deviance information criteria (DIC) were used to test the goodness of fit for each model. The model with lower values of AIC and DIC was considered better fit. Stata version 14 was used for the data analysis.
Ethical Approval
This study did not require ethical approval as a secondary data analysis was performed using PDHS data for year 2012-2013. Data were obtained from measuredhs.com after permission. PDHS data are collected with due ethical considerations.
Results
Descriptive Analysis
The prevalence of immunized children was found to be 39.3% (2659 out of 6765) among the studied sample. Percentage of immunization in children who belong to the lowest wealth quintile (poorest families) was 10.3%, which is lowest among children of other wealth quintiles who received full immunization. Majority of fully immunized children (about 50%) belong to noneducated mothers while 57% of the mothers have access to media whose child cover all prescribed doses of vaccines. Only 18% of the fully immunized children belong to working mother, which is very low as compared with children of nonworking mothers. Moreover, all the selected variables, except child’s gender and maternal age, were found significant in bivariate analysis. Detailed description of these and other factors can be seen in Table 1. The mean value of VIF was estimated to be 1.72 for this study indicating the absence of multicollinearity. We also assessed interactions between individual- and community-level factors; however, there was no statistically significant interaction between individual- and community-level variables.
Percentage Distribution of Individual- and Community-Level Characteristics of Child Immunization. a
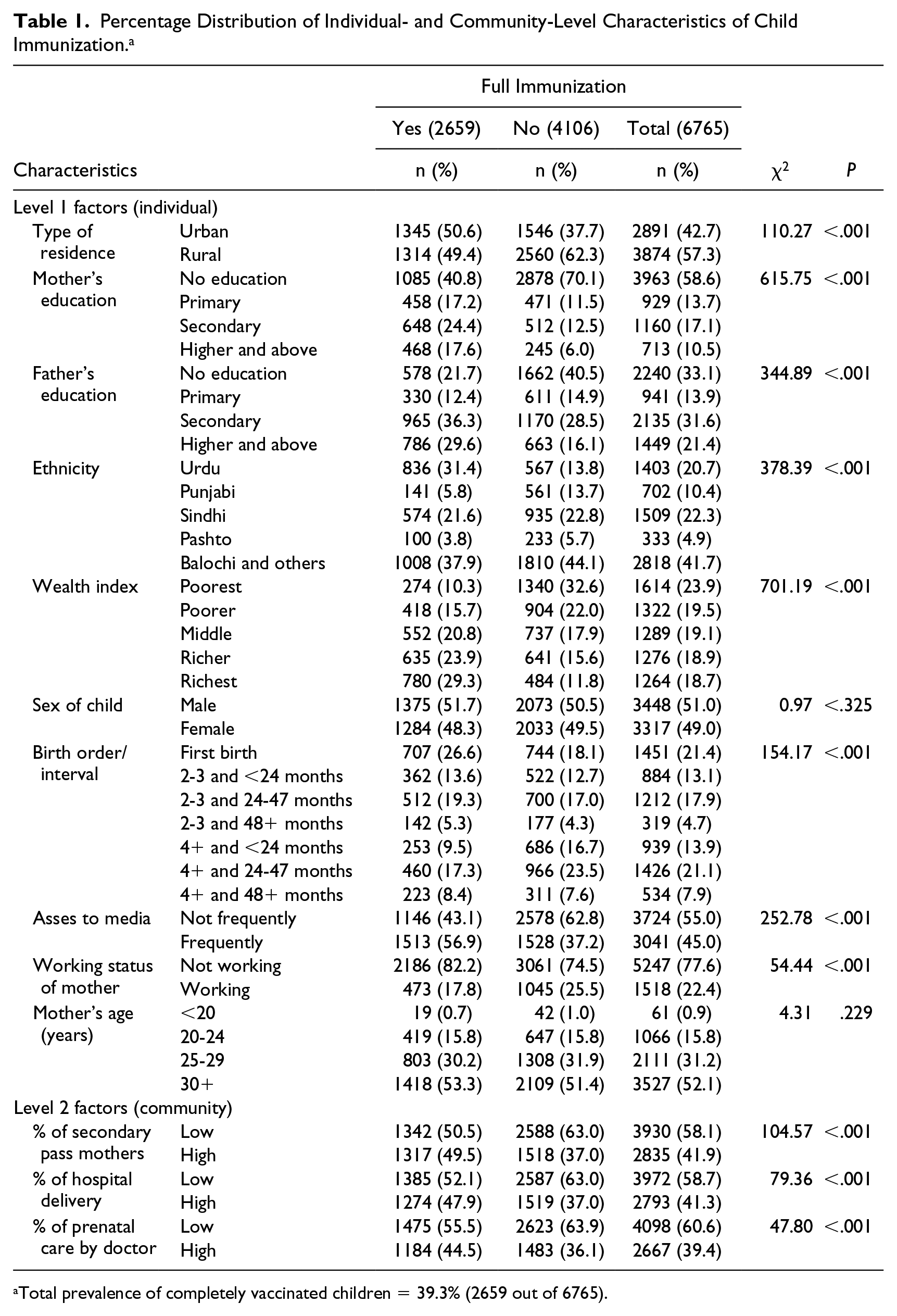
Total prevalence of completely vaccinated children = 39.3% (2659 out of 6765).
Multilevel Analysis
The results of Model 1 showed that variation in the likelihood of immunization across communities was significant (
Father’s education also has an impact on the immunization of the children, that is, if father has higher and above education then there are 41% more chances that his child is immunized (OR = 1.41, 95% CI = 1.15-1.72; P < .001). Access to media (TV) also increase the odds of immunization (OR = 1.19, 95% CI = 1.03-1.37; P < .05). The child of a working mother has 18% lower odds of getting immunized as compared with that of non-working mother (OR = 0.82, 95% CI = 0.70-0.96; P < .05).
In Model 3, we included both the individual- and community-level predictors. From individual level, mother’s education, ethnicity, wealth index, father’s education, access to media, and mother’s working status was found to have significant association with the response variable. While from the community-level variables only the percentage of mother’s education was turnout to be significant. The pattern of association remained the same as it was in Model 2. The results showed that the odds of immunization are high in the community where the percentage of educated mothers is high (OR = 1.43, 95% CI = 1.14-1.80; P < .005). There were higher odds of immunization for the children who reside in the communities where percentage of delivery in hospital is high, but these results were not statistically significant (OR = 1.13, 95% CI = 0.87-1.48; P < .35). The results of the 3 models are shown in Table 2. The values of AIC and DIC showed subsequent decrease, which indicated that the final model better fits the data (Table 3).
Multilevel Analysis of the Effects of Individual and Community Factors on Immunization.
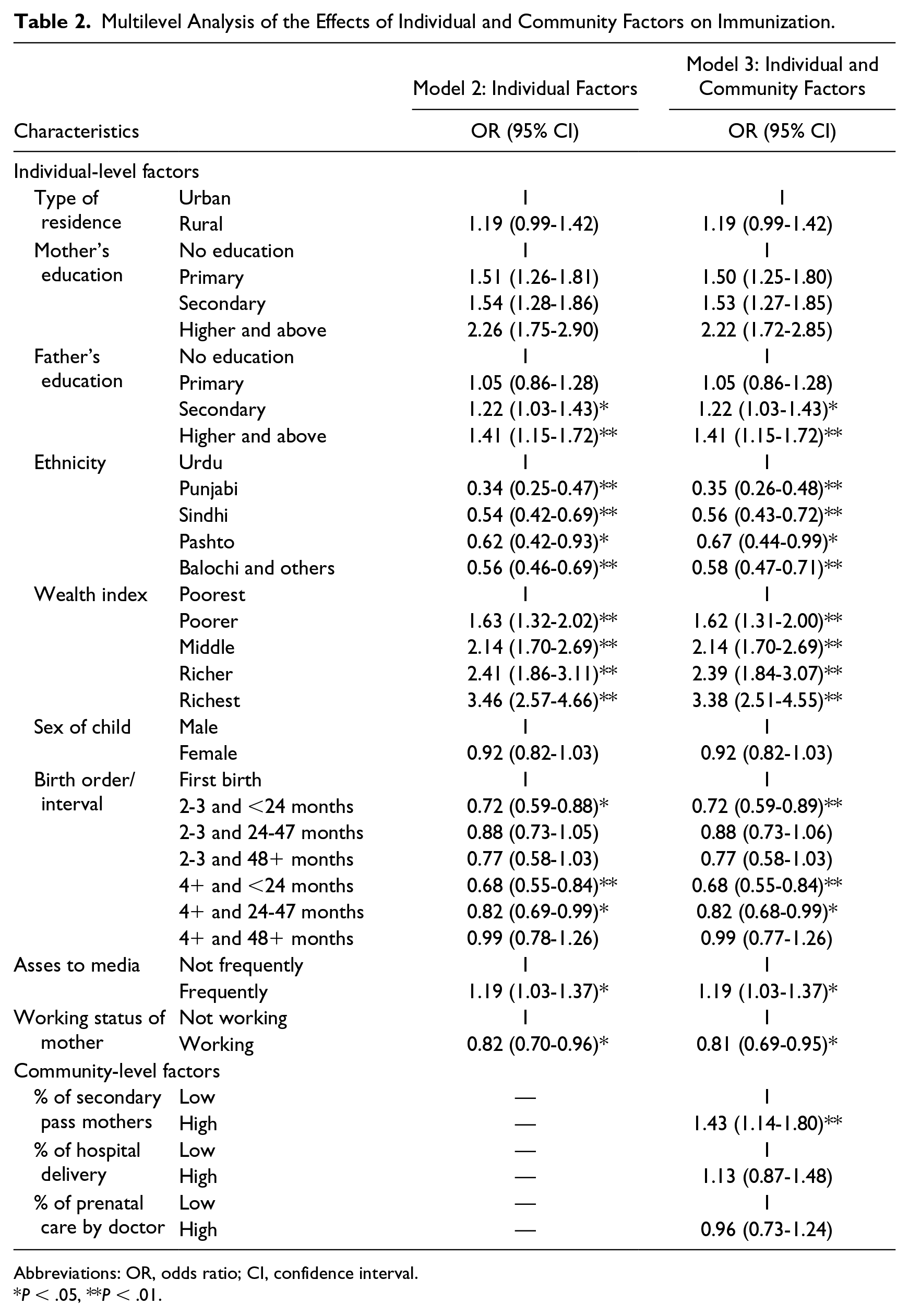
Abbreviations: OR, odds ratio; CI, confidence interval.
P < .05, **P < .01.
Measures of Variation and Model Goodness of Fit.
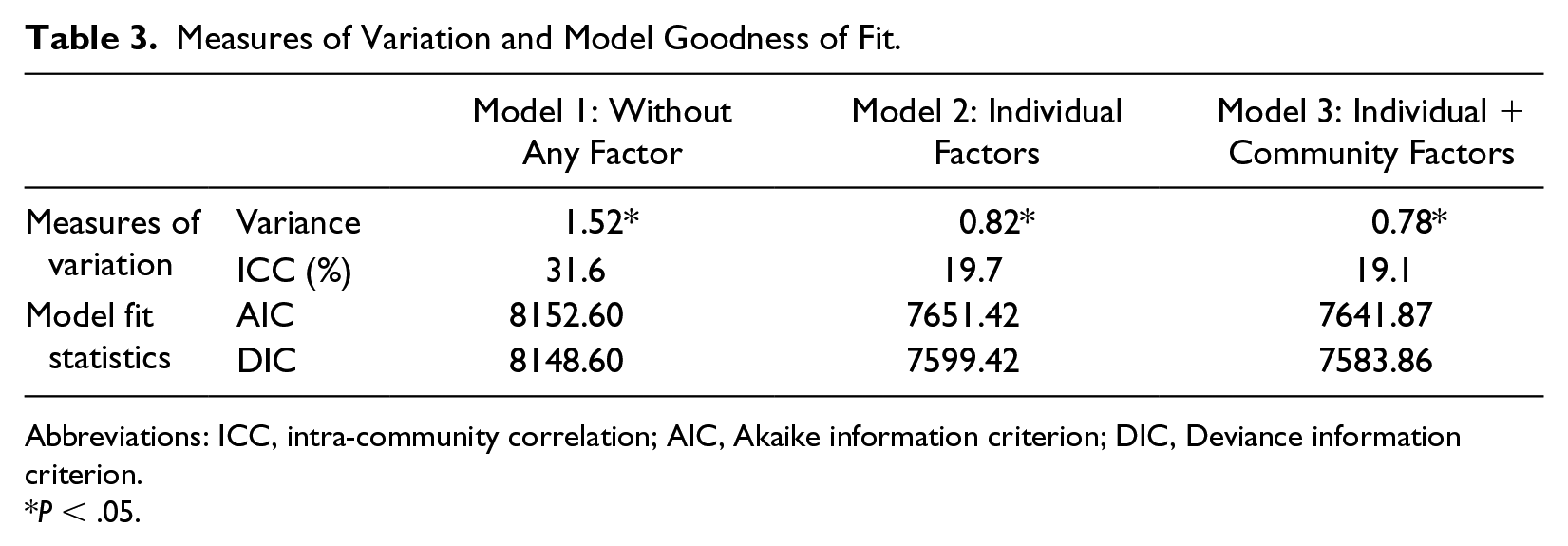
Abbreviations: ICC, intra-community correlation; AIC, Akaike information criterion; DIC, Deviance information criterion.
P < .05.
Discussion
The findings of this study indicate the significant association between child immunization and community-level factors. Mother’s education was significantly associated with the complete immunization. Parent’s education (especially mother’s education) has positive association with the vaccination uptake, which shows that parental education has strong positive effect on child health. The results are also consistent with other studies.1,5,20,21 An improved educational status of mother may consider as a proxy for the increment in the household decision making autonomy, which further act as a mediator for the relation between child’s health and mother’s decision-making autonomy. 22 Another way of explanation may be that an educated mother may get well pay jobs and more empowered in developing countries, 23 which positively affect the child’s health ultimately. Thus, we may conclude that improved educational status of mother may consider as a protective measure of child health. Different ethnic groups have specific cultural characteristics, which may affect the parent’s behavior regarding child’s HC. 24 Ethnicity also showed a significant relationship with child immunization status as depicted in Malaysia. 25 The children belonging to the Urdu ethnicity were more likely to be completely immunized than children of other ethnic groups while Punjabi children were more likely to be immunized in some other studies. 26 Wealth status of the households plays a key role in the health measures of the family. 27 Results of this study also demonstrate that the children of richest wealth quintile have more chances of full vaccination as compared with the poorest wealth quintile. It is also identified that as the wealth status of the family improves, the chance of child’s complete vaccination coverage increases. Moreover, along with improved household’s wealth status, the impact of maternal education may also be channelized through mothers better health knowledge, more access to and use of HC services, and better feeding practices. These findings are compared well with the findings elsewhere.28 -30 Access to electronic media also has significant association with vaccination of children. This is perhaps due the awareness through different programs and advertisements concerning the child health issues and the results are consistent with other findings. 31 Working status of mother has a negative impact on the vaccination of children, that is, the children of working mothers have lower chances of having immunized. We found similar findings in 20 that children living in the communities where the proportion of mothers with secondary education was high, have higher likelihood of having complete vaccination coverage. The children of the communities with high percentage of hospital deliveries were more likely to be vaccinated. Other studies discuss the same findings. 32
Study findings demonstrated that both community and individual-level factors have substantial impact on child immunization status. There is a need to increase maternal education, poverty elevation, and removal of rural urban differences for improvement in the present status of immunization. Community health workers, called lady health workers in Pakistan, may effectively improve the vaccination coverage especially in marginalized area and also in children of uneducated mothers, as lady health workers are often responsible for vaccination process within their community. Also, the findings of this study will help policy makers to consider the importance of these determining factors—specially, maternal education—to strengthen vaccination coverage. Since the community-level factors remained significant, further investigation of these factors will be of interest. Moreover, we may disaggregate the categories of response variable (such as not-immunized, partially immunized, and fully immunized) and can use advanced statistical methods (eg, multilevel multinomial logistic regression) to explore more detailed findings.
The results of this study should however be considered in the light of some limitations. First, the study used PSUs as a proxy for the community, which may generate information bias. Second, some important factors which may influence the immunization uptake (eg, distance to the health facility) are not included. Third, the use of indirect measure of household’s wealth status may be criticized. However, since it is hard to collect reliable information of income and expenditure data in developing countries like Pakistan, an asset-based wealth index is commonly considered a good proxy for household wealth status.31,33
Supplemental Material
DHS_Download_Account_Application – Supplemental material for Role of Maternal Education and Vaccination Coverage: Evidence From Pakistan Demographic and Health Survey
Supplemental material, DHS_Download_Account_Application for Role of Maternal Education and Vaccination Coverage: Evidence From Pakistan Demographic and Health Survey by Atta Muhammad Asif, Muhammad Akbar, Muhammad Ramzan Tahir and Irshad Ahmad Arshad in Asia Pacific Journal of Public Health
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.