
Abstract

Introduction
Contact tracing is one of the fundamental interventions in epidemic investigation and control of an epidemic with the goal of reducing the number of onward infections from the traced contact. 1 The efficacy of contract tracing and containment measures are related to the initial epidemic growth rate and epidemic duration; however, it is important to note that contract tracing is an intermediary function that results in isolation or treatment. Modelling studies have shown that contact tracing among clustered networks is more effective than among random networks, even at larger clustering. 2 At the same time, the importance of considering the extent of assortment of the networks has been highlighted in modelling studies. 2
Incorporating geographic contacts into contract tracing has been identified as a critical parameter, particularly in relation to diseases that has more transmission routes than direct person-to-person transmission. Models that have applied geographic contacts to SARS (severe acute respiratory syndrome) contact tracing showed a much higher connectivity than personal contacts and is useful for determining disease transmission scenarios in a given population. 3
This article describes the contact tracing and containment procedures in the Maldives and how the results correlate with the generated mathematical model for coronavirus disease 2019 (COVID-19) outbreak.
Methodology
This research was approved by the National Health Research Committee of the Maldives and the Ethics Approval Number is NHRC/2020/004. In the first phase, a mathematical model was developed to estimate the number of cases and contacts per imported case by considering the possible encounters of a traveler to the Maldives (see supplementary materials, available online, for the model parameters and outputs).
Model Assumptions
First case is assumed to be an imported case, and all imported cases are assumed to follow a similar path of case progression.
The intensity of containment measures is assumed to increase weekly from 1 till 10, which is the assumed highest level of intensity of the country’s capacity (including foreign aid), so it would remain at 10 after that until outbreak resolves.
At the beginning (week 1), with no containment measures a reproductive rate (R) is arbitrarily set at 3 (which is the number of cases that each infected case can produce), but as the intensity of the containment measures increases R is assumed to decrease steadily (by 1/12th) each week. The fraction (1/12th) is an arbitrary number, with the assumption that the outbreak will resolve in 3 months.
The cases will start at 1 for week 1 and 3 for week 2, after which the number of cases for each week (beginning with week 3) will be calculated by multiplying the number of cases of the previous week with the estimated value of R for the current week.
Of the contacts of the index case, only 3 will become infected cases of which we would be able to detect and isolate only 2 cases, leaving 1 undetected case within the community, which will then lead to community transmission. The weekly number of contacts is estimated by multiplying the new contacts from 1 case/week with the number of cases for that week. New contacts from 1 case/week is calculated by multiplying the proportion of contacts with the estimated number of contacts/weeks. The estimated number of contacts/weeks starts at 144 for week 1 and 21 from week 2 onward. The proportion of the contacts is an arbitrary number, which starts at 1 and decreases by 1/10th until 9/10th (1/10), after which it which remains constant.
The disease is assumed to become symptomatic within a week (7 days).
The model predicts incident cases and contacts, so those who recover, die, or become severe cases will not be removed from the model.
The model will become empty when the number of cases/contacts reaches 800 000 (estimated population of Maldives (immigrants inclusive).
The data from the actual confirmed cases and contacts were extracted from the Outbreak database. The first case in the Maldives was identified outside the country and hence contact tracing was started and actions taken according to risk categorization identified by the Health Protection Agency of the Maldives. 4 The first case was identified on March 6, 2020 (reported on 7 March), and the results were presented up to July 19, 2020.
The data from the model are then compared with the actual contact tracing of COVID-19 in the country. Inferences were drawn on the efficiency and effectiveness of contract tracing in containing disease transmission with reference to the mathematical model. Since the data are not normally distributed, a Mann-Whitney U test was carried out to find whether there is a significant difference in actual and predicted data.
Results
Figure 1 shows the mathematical model results for the progression of confirmed cases (weekly) from a single imported case compared with the actual number of cases for 29 weeks.
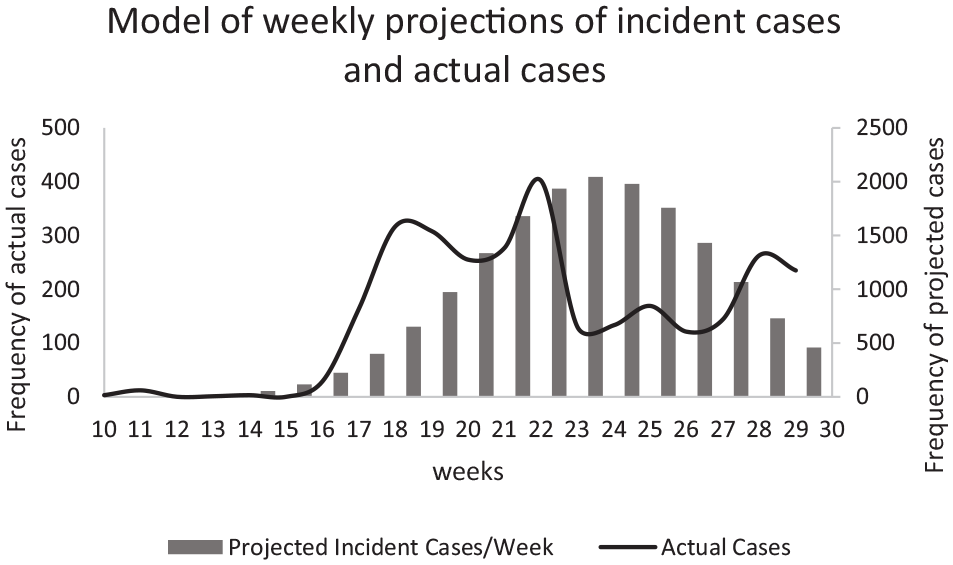
Number of cases in the predicted model compared with actual number of cases. Mann-Whitney U test result: W = 96.5, P = .005 (95% confidence interval, 5% error).
Mann-Whitney U test result showed that there is a statistically significant difference between the predicted number of cases and the actual number of cases. The actual number of cases are lower than that of the predicted number of cases each week, which indicates that the containment measures implemented in Maldives were successful in reducing the peak of the outbreak.
Figure 2 shows the mathematical model results for the progression of contacts (weekly) compared with the actual number of contacts for 29 weeks.
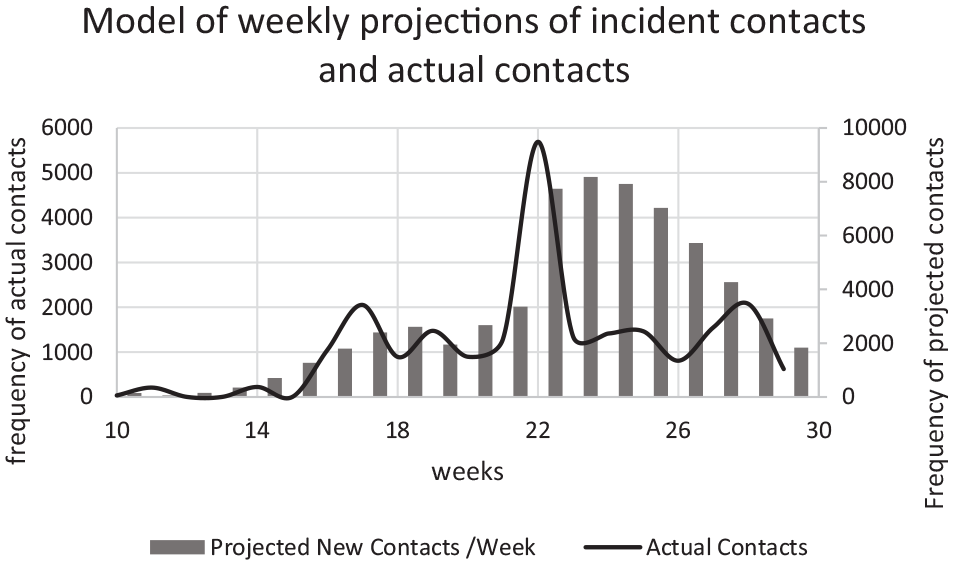
Number of contacts in the predicted model compared with actual number of contacts. Mann-Whitney U test result: W = 99, P = .006 (95% confidence interval, 5% error).
Mann-Whitney U test result showed that there is a statistically significant difference between the predicted number of contacts and the actual number of contacts. The actual number of contacts are lower that the predicted number of cases each week, which indicates that the contact tracing efforts and the containment measures were successful.
Discussion
The contract tracing approach in the Maldives allowed for near universal tracing of contacts and for prioritized action for high-risk contacts removing high infectious nodes in the network, which is considered to be more effective contact tracing.2,5 The results show that contact tracing was timely and close to complete since the actual values were not higher than predicted values. The reason for the actual number of cases being lower than the predicted value can be that very stringent measures were taken until July 19, 2020. Another reason might be that the number of samples tested for COVID-19 is lower than needed. While there is some debate with regard to the target of tracing, 6 emerging literature on COVID-19 suggests that tracing and containment of 70% of contacts is effective in early epidemic control. 7
Conclusion
The approach to contact tracing in the Maldives following imported cases of COVID-19 was vigorous and was effective in identifying close to all contacts. The effectiveness in containment is associated with the prompt quarantine, isolation of contacts and suspected cases, which delayed the community spread. If the COVID-19 tests were done on a larger sample of the population, the actual values may have been closer to the predicted values.
Supplemental Material
Supplementary_Tables – Supplemental material for Contact Tracing for Containment of Novel Coronavirus Disease (COVID-19) in the Early Phase of the Epidemic in the Maldives
Supplemental material, Supplementary_Tables for Contact Tracing for Containment of Novel Coronavirus Disease (COVID-19) in the Early Phase of the Epidemic in the Maldives by Ibrahim Afzal, Raheema Abdul Raheem, Nazla Rafeeq and Sheena Moosa in Asia Pacific Journal of Public Health
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.