
Abstract
Bhutan aims to achieve 100% institutional delivery coverage. While evidence indicates improved institutional delivery coverage over the years, coverage in some of the districts is only 49%. This study was aimed at exploring barriers to institutional delivery in three low-coverage districts. In-depth qualitative interviews and six focus group discussions were conducted in December 2015. The analysis was done as per the Braun and Clarke’s 6-phase guide to doing thematic analysis. This study sheds light on 15 barriers for institutional deliveries, which include hesitancy to seek health care when the pregnancy is out of wedlock, the restriction of alcohol consumption at health centers, fear of hypothermia in cold places, pastoralism, health care providers shortage, lack of maternity waiting home and food, distance, difficult terrain, lack of transportation services, and financial constraints. Some of these barriers could be unique to Bhutan. The coverage could be improved considerably if the recommendations in this article are implemented.
What We Already Know
Till date, two quantitative studies on low institutional delivery were conducted in Bhutan.
Mother’s age, socioeconomic status, location (rural vs urban), region of the country, antenatal visits, delivery history, and distance to health facilities were found to be associated with home delivery in Bhutan.
What This Article Adds
This articles sheds lights on some 15 barriers to low institutional delivery in Bhutan from a qualitative study.
Some of these barriers could be unique to Bhutan and similar settings.
Introduction
Globally, more than 71% of births were assisted by skilled health care providers in 2014, an increase from 59% in 1990. 1 Similarly, Bhutan has made commendable progress over the years. The proportion has increased from 19.8% in 2000 to 73.7% in 2012.2,3 However, almost one third of deliveries still take place at home, exposing mothers and newborns to a greater risk of morbidity and mortality.
While the National Health Survey (NHS) 2012 has shown an overall increase in institutional delivery rate, the disparity among the districts remains hugely pronounced, with some districts reporting institutional delivery rates as high as 96% and some as low as 49%. 3 All these pieces of evidence underscore the need to scale up institutional delivery to ensure proper medical attention for every birth and during the critical period after delivery. However, except for a small study carried out in one of the districts and secondary analysis of NHS 2012 data,4,5 no other studies have been carried out to understand the determinants of institutional deliveries in the country. These 2 quantitative studies found Mother’s age, 5 socioeconomic status, 5 location (rural vs urban), 5 region of the country, 5 number of antenatal visits, 5 delivery history,4,5 and distance to health facilities 4 to be associated with home delivery. Studies conducted elsewhere have reported that human resources,6-8 services,6,7,9 distance, terrain, and transportation,6,7,10,11 economic hardship and handling domestic chores,6-10 feeling shy,7,11 traditional practices,6,7,9 decision-making power,6,7,10 awareness, and low risk perception6,7,9,10 to be associated with low institutional delivery. In this light, this qualitative study aimed at exploring barriers to institutional delivery in Bhutan.
Methods
The in-depth interviews (IDIs) and focused group discussion (FGD) were carried out in three districts of Bhutan with low rates of institutional deliveries. These three districts were Zhemgang, Samdrup Jongkhar, and Trashigang. The IDI were intended to collect information associated with the behavior of the individual interviewed, and the FGD were intended to collect information about participants’ views about some type of normative behavior.
Study Setting
Bhutan is a small landlocked country in the Eastern Himalayas with the current population of 748 931. 12 The country is in pursuance of the developmental philosophy of Gross National Happiness, and health care services are provided by the government, free of cost at the point of delivery. The health care system of Bhutan is 3-tiered. There are three referral hospitals, 46 hospitals, 185 primary health centers (PHCs), 49 sub-post, five health information service centre (HISC), and 553 outreach clinics (ORC) besides the military health care facilities. 13 About 95.4% of the population stays within 3-hour distance from the health centers. 3 In terms of institutional delivery proportion, while the overall percentage for Bhutan in 2012 was 73.7%, the coverage rates for Zhemgang, Samdrup Jongkhar, and Trashigang districts were 49.4%, 49.5%, and 52.5%, respectively. 3 During the 2-year period prior to the 2012 survey, a total of 2338 live births were reported. Out of these live births, 144 (3.59%), 113 (4.42%), and 141 (9.42%) were from Zhemgang, Samdrup Jongkhar, and Trashigang districts, respectively. 3 While the national poverty rate in 2017 was 8.2%, the poverty rates were 25.1% in Zhemgang, 8.3% in Samdrup Jongkhar, and 10.7% in Trashigang.
Zhemgang is located in central Bhutan and is one of the least developed districts in the country. Samdrup Jongkhar and Trashigang districts are located in eastern Bhutan, and districts in eastern part of the country are generally less developed than districts in central and western regions. All in all, these three districts had the lowest institutional delivery rates in 2012 (Figure 1).
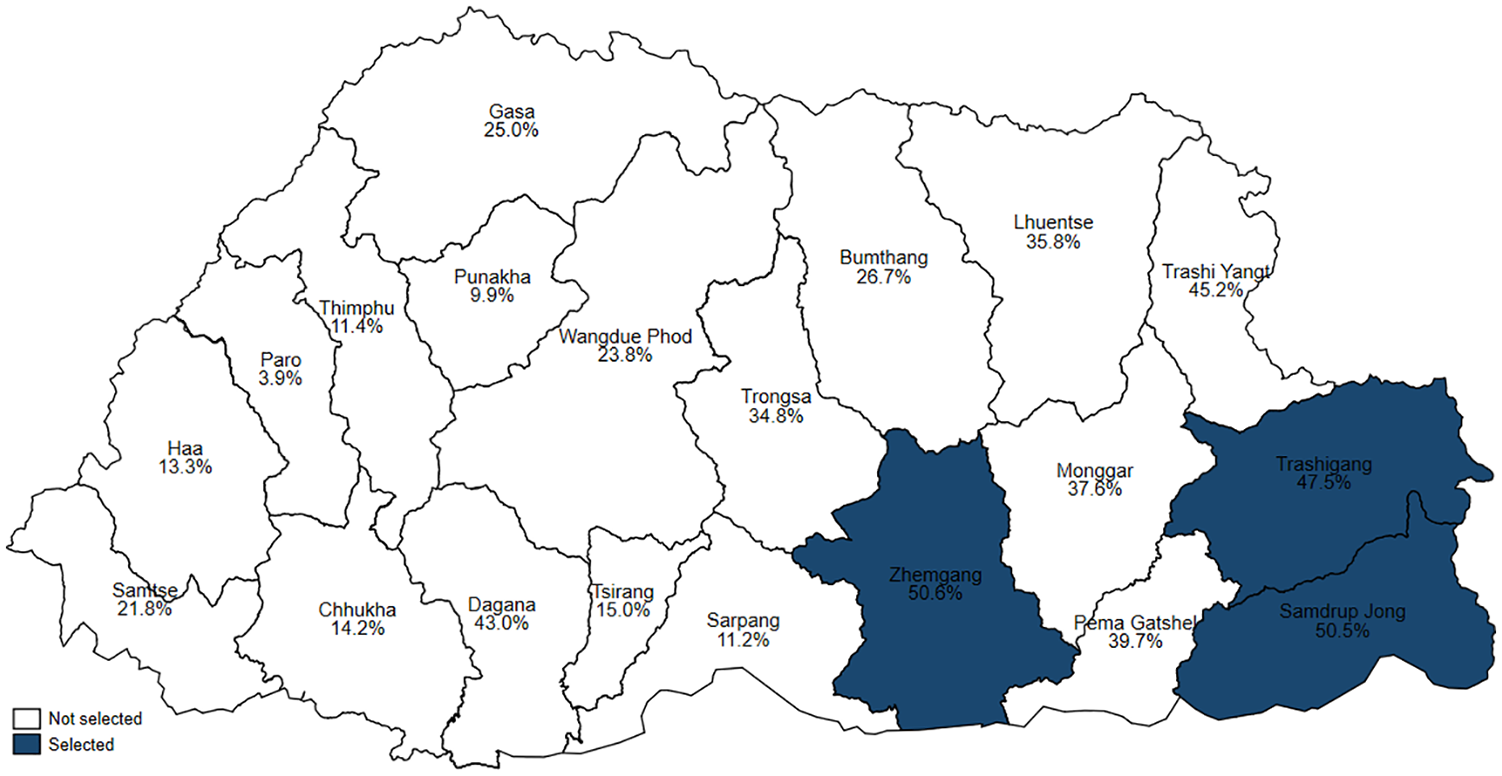
Percent of home delivery in Bhutan by district as per National Health Survey 2012 with the study districts highlighted.
Study Participants and Sampling Technique
All mothers who had delivered at home in 2015 in the selected study sites were considered eligible for IDIs, except for mothers with hearing and speaking impairments, serious illness, and mental unsoundness. Fifty IDIs were conducted with the women who had not delivered at health centers (Table 1).
Sociodemographic Characteristics of the Participants of In-Depth Interviews on Factors Associated With Home Deliveries in Zhemgang, SamdrupJongkhar, and Trashigang Districts of Bhutan, 2015.
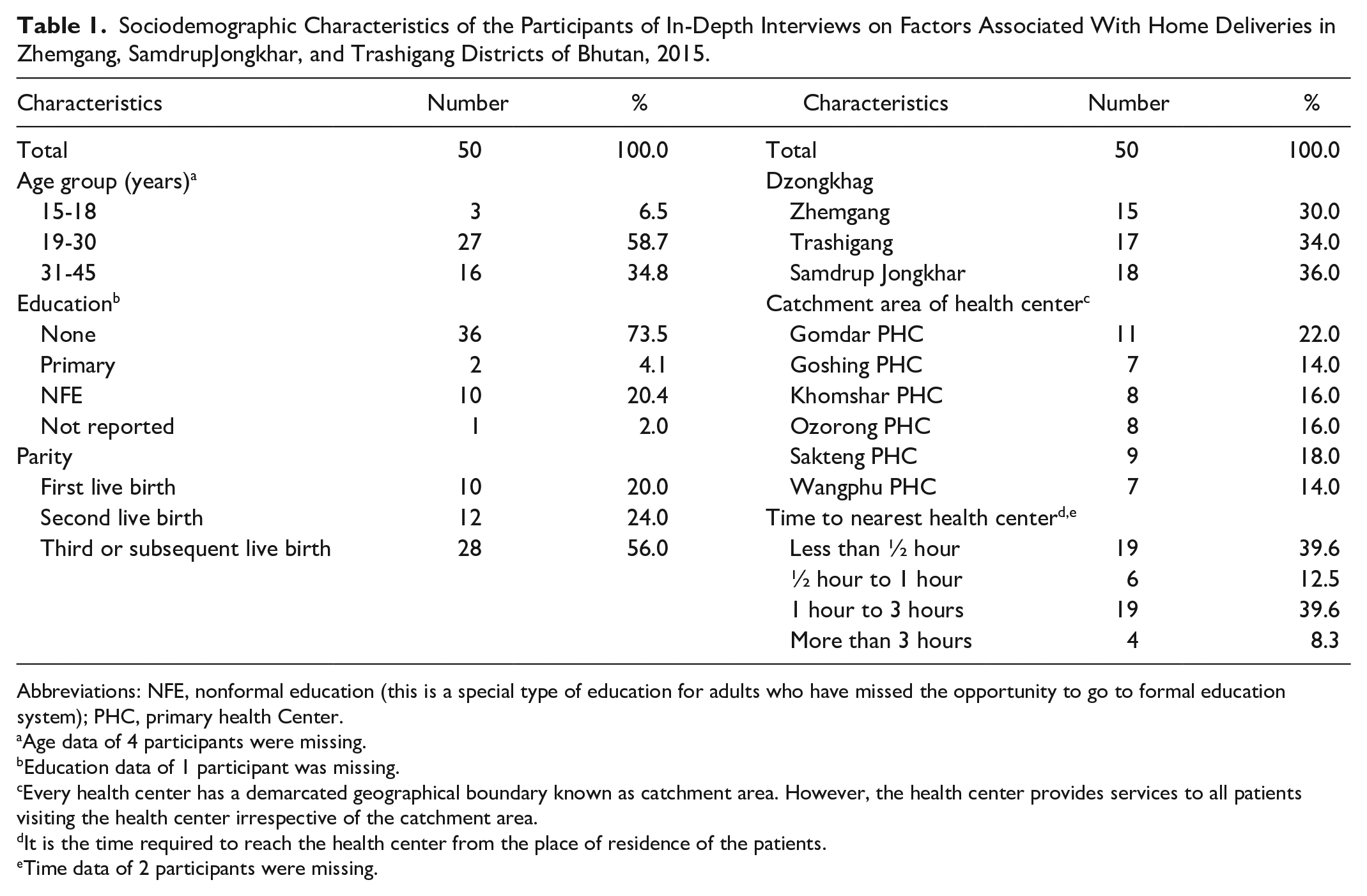
Abbreviations: NFE, nonformal education (this is a special type of education for adults who have missed the opportunity to go to formal education system); PHC, primary health Center.
Age data of 4 participants were missing.
Education data of 1 participant was missing.
Every health center has a demarcated geographical boundary known as catchment area. However, the health center provides services to all patients visiting the health center irrespective of the catchment area.
It is the time required to reach the health center from the place of residence of the patients.
Time data of 2 participants were missing.
The list of home deliveries were collected from the selected districts with help from the district health offices. Based on the list, the health center catchment areas with the highest and second-highest numbers of home deliveries were selected as study sites under each district. A minimum of 15 women were recruited from each district. The first eight mothers were randomly selected from the health center catchment areas with the highest home deliveries, and the remaining seven mothers were randomly selected from the area with second-highest home deliveries.
The FGDs were stratified by gender into two groups. The homogeneous women group consisted of only women, including pregnant women, and the mixed group was composed of the key informants from the community such as the local health care providers, mothers, fathers, village elders, local leaders, and village health workers. There were 10 to 15 participants in each FGD. A total of six FGDs were conducted; one women group FGD and one mixed group FGD in each district. The participants of FGD were purposively selected by the researcher with the help of the local health care providers.
Data Collection
The data were collected in December 2015. The IDIs were conducted at the residence of the selected mothers and took around 20 to 30 minutes to complete. The FGDs were conducted at the health centers and lasted about 1 hour each.
Two sets of guidelines, one for an IDI and one for FGD, were developed and pretested (Annexure I, available online). The two researchers, fluent in the local languages, conducted IDIs and FGDs. Prior to each interview or FGD, they introduced themselves as public health professionals from the Ministry of Health conducting research to to find out why some females are not coming to health facilities for delivery. The participants were explained about the purpose and benefits of the study. The range of themes covered in the interviews included sociodemographic information, mother’s knowledge on pregnancy and childbirth, delivery care practices, danger signs of pregnancy and childbirth, decision making, and reasons for home delivery. Interviews and FGDs were recorded, transcribed, and translated into English by the researchers. To minimize errors, all transcriptions and translations were verified collaboratively by the two researchers who conducted IDIs and FGDs.
Analysis
The translated transcriptions were the primary data source for the analysis presented in this article. WEFT QDA software was used for categorizing (coding) and analysis. Thematic analysis was done as per the Braun and Clarke’s 6-phase guide to doing thematic analysis. 14 The phases in the analysis included a line-by-line reading and rereading of all the transcriptions to gain a descriptive understanding of the responses to each research question and come up with codes and patterns. Next, the information pertaining to the research questions were coded based on theory as well as the responses by three of the researchers. Then, the thematic analysis was drawn based on the codes. This was followed by reviewing themes, refining themes, naming themes, final analysis, and report writing.
Ethics Approval and Informed Consent to Participate
Administrative clearance for conducting the study was sought from the Ministry of Health, and ethical approval was obtained from the Research Ethics Board of Health. The ethics approval number is REBH/Approval/2015/045, dated December 8, 2015. Participation in the study was voluntary, and prior written informed consent was obtained from all participants. For the two participants who were minors, informed consent from their parents or legal guardians in addition to informed assent from the minor themselves were obtained. Personal identifiers were not used in the report to ensure confidentiality, and the researchers ensured there was no one else in the interview vicinity for privacy and confidentiality as well as to encourage open sharing by the participants. All transcripts have been coded with unique alphanumeric codes. The first three alphabets indicate FGD and IDI. It is followed by 2-digit district code, 2-digit health center code, and 2-digit participants serial number in case of IDI. The FGDs are coded by 2-digit district code, and 2-digit FDG serial number.
Result
Six FGDs with 74 individuals and 50 IDIs were conducted. Every individual was approached for the study participated. Among participants in the IDIs, 58.1% were in the age group of 19 to 30 years and 73.5% were uneducated (Table 1). There were comparable numbers of participants from each district.
The analysis identified 15 barriers to institutional delivery in the study sites, which are reported as four broad themes and 15 subthemes (Figure 2).
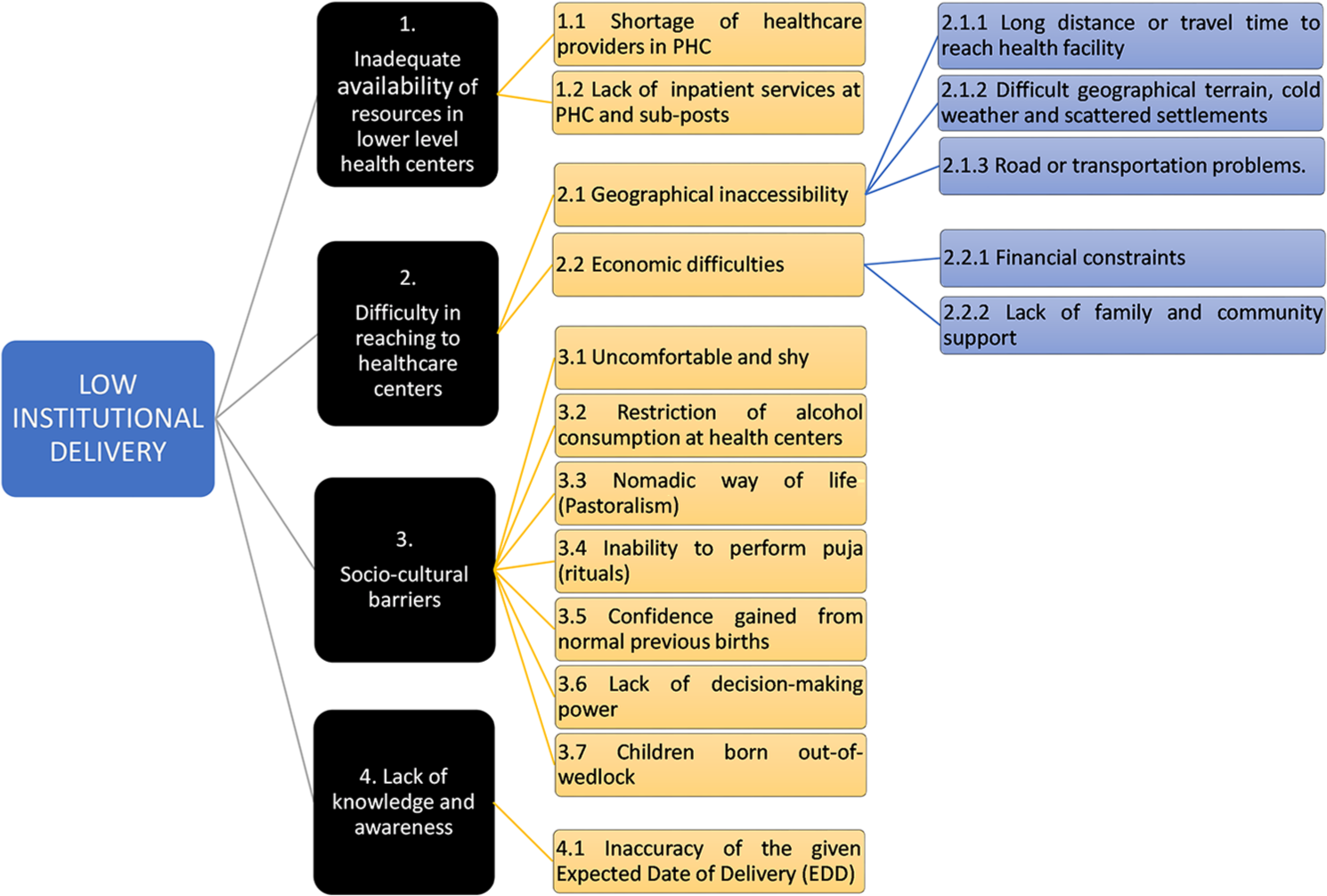
Barriers to institutional delivery in Zhemgang, Samdrup Jongkhar, and Trashigang districts of Bhutan 2015.
Theme 1: Inadequate Availability of Resources in Lower Level Health Centers
The barriers under this theme are categorized into following two subthemes.
Theme 1.1: Shortage of Health Care Providers in PHC
Many health centers in Bhutan, particularly in rural areas, are still staffed by a single health care provider. The absence of health care providers in the health center was one of the reasons for home deliveries. One of the PHCs in Eastern Bhutan caters to over 400 households and a central school, but it had only one health care provider. In the absence of another health care provider, the PHC often remains closed. The lone health assistant said, I often have to close the PHC when I am away for duty travel like attending the outreach clinics, trainings, meetings, and workshops or when I am on leave.
Participants also repeatedly pointed out the shortage of health care providers as a hindrance to institutional delivery as indicated by the following quotes so much so that one of the woman had actually “. . . reach PHC [for delivery] and I found that the sister wasn’t there at the station.” (IDI250209—28-year-old mother).
There is shortage of health worker in . . . PHC. Upon calling to the Sister, she told me that she was at Deothang [attending training]. The PHC remains closed quite often. (FGD2502—a mother who delivered at home) We need one more health worker as existing one have to attend workshop, trainings, and meetings. In his absence, the center remains closed. (FGD2102—Gup, a local leader) There is a need for [additional] female health worker because . . . it is difficult for one health care providers to manage all patients. (FGD2502—Mangmi, a local leader)
The lack of experience of health care providers in conducting deliveries was also found to hinder the pregnant women from availing an institutional delivery.
I came here to the health facility. HA [Health Assistant] told me that she did not have experience to deliver a baby . . . I went home. This is how I delivered at home. (IDI210105—17 year old mother)
Theme 1.2: Lack of Inpatient Services at PHC and Sub-Posts
Most women cited lodging and food availability as a deciding point for home delivery, and many of them felt that inpatient services have to be made available in PHC too.
Even if we wish to come here [PHC], we don’t have good provision to stay nearby and there is no cooking facilities . . . We need to carry everything as we don’t have any shops nearby. (IDI300203—24-year-old mother) In bigger hospital, the patients get food. But out here, we don’t have such services. (IDI300207—39-year-old mother) We can bring edibles and food items with us. There is a need to have cooking facilities such as gas stove to heat our butter and food. (IDI300102—34-year-old mother)
In one particular case, a local leader mentioned that the local government provided necessary amenities to the PHC to encourage institutional delivery and help the expecting mothers coming from poor background with financial incentives.
LG [local government] has supported with rice cooker, curry cooker, and water boiler to the BHU [Basic Health Unit; now renamed as Primary Health Center (PHC)]. For expecting mothers, coming from distant villages and who are poor may be given the financial incentive to buy foods. (FGD2102—Gup, a local leader)
Theme 2: Difficulty in Reaching Health Care Centers
This theme is further divided into two subthemes.
Theme 2.1: Geographical Inaccessibility
This, in turn, is further categorized into three themes.
Theme 2.1.1: long distance or time taken to reach to health facility
Many of the respondents have pointed out the distance or time taken to reach to health centers to be the crucial factor for them.
I have been advised [by health care provider] to go to Gelephu hospital . . . for delivery . . . An ambulance from Yebilaptsa [Hospital] was also arranged. As my house is far from motorable road, I was carried on the [traditional] bamboo stretcher by four men including my husband . . . I delivered on the way before reaching the motorable road. (IDI300106—23-year-old mother)
The last quote tells us how some of the women fail to reach to health centers for delivery because of difficult geographical terrain and lack of motorable roads. The health care provider had advised her, and she was on her way to a health center.
I couldn’t go to health center as it is located far away from my home. (FGD3002—a mother of four children) It’s difficult here as my house is far from the motorable road. It is also difficult to find vehicle from the road point. (IDI300101—39-year-old mother) It takes 6 hours to reach to the PHC from my home. (IDI210108—28-year-old mother)
On the other hand, some of the women were staying in the vicinity of a health care facility but they still delivered at home. Many women who lived very near to health centers also delivered at home in Ozorong and Sakteng gewog (block) under Trashigang district.
Theme 2.1.2: road or transportation problems
Not having a motorable road in remote areas and the damage of roads and foot path during rainy seasons were highlighted as one of the pertinent factors for pregnant women not availing services at health centers.
Lack of road connectivity in those villages that are 4 or 5 hours walking distance away from health centers make people deliver at home. (FGD2102—Lama, a religious figure) Lack of road in Hyla village is a problem. It is difficult to bring in the stretcher. (FGD2102—a village health worker) Lack of reliable road connectivity is a major problem. Few years back, a young boy studying in 10th class has died mainly due to road block . . . couldn’t reach the destination due to monsoon roadblock. (FGD3001—Tshogpa, a local leader)
Theme 2.1.3: difficult geographical terrain, cold weather, and scattered settlements
Some of the settlements in Bhutan are located at high altitude, and they are inaccessible during winter because of heavy snowfall. As reported by the respondents from Sakteng gewog, the people living in very cold places in Bhutan do not come to health centers for delivery because of fear of suffering from hypothermia in the health centers as well as on the way from health care facility to their home. The researchers during the data collection observed that the health centers do not have proper heating systems. The traditional heating system, Bukari, did not warm up the rooms.
Our place is very cold and the new born could die of cold weather if we come to deliver to health centers. Our homes are warm and suitable for both mother and child. (FDG2501—a mother of two children)
Theme 2.2: Economic Difficulties
Under this theme, the barriers identified are coded into two themes.
Theme 2.2.1: financial constraint
A village health worker said that financial constraint kept the expecting mothers of a poor economic background from attending an institutional delivery. Many women narrated the stories of facing financial hardship while planning to go for an institutional delivery.
I have been asked to go to Gelephu Hospital [Central Regional Referral Hospital] due to bleeding problem but could not manage to go this time due to financial problem. Also there are no relatives at Gelephu. We require lot of money to go to delivery at Gelephu. I have incurred about Nu 30 000 during my previous childbirth. So I decided to deliver at home this time. (IDI300103—29-year-old mother) Some are very poor and can’t afford to come to health center. (FGD3001—a village health worker)
Theme 2.2.2: lack of family and community support
The average household size in Bhutan is 4.6, 15 and a typical household will have two adults and 2 to 3 children. All children go to school, and the parents have to take care of household chores and tend to the domestic animals. They also have to cook for their children and ready them for school. It is difficult for pregnant women to travel alone to health facilities for availing the services, particularly if the distance is far and if the path is through difficult geographical terrain or dense forest. As a result, some of the women in this situation could not come to the health centers for delivery.
Lack of family members to look after cattle and household chores . . . makes it not possible for women to visit health centers. (FGD2102—a village health worker)
The absence of husbands at home during delivery time and difficulties in arranging for people to carry the delivering mother to a health center were also some of the difficulties the women faced.
During delivery time, my husband was away herding our cow in the Jangsa [cow herding land which are usually far away from their home] and children were in the school. So I could not manage to come to health center. (IDI300202—41-year-old mother) There was no one to accompany me during the labor pain. I don’t have husband. (FGD2102—24-year-old mother)
Theme 3: Sociocultural Barriers
Barriers identified under this theme are categorized into following seven subthemes.
Theme 3.1: Feeling Uncomfortable and Shy
While a few participants highlighted feeling uncomfortable and shy to be the reason as to why they did not come to a health facility for delivery, there were other participants who were of the opinion that embarrassment is not a barrier for an institutional delivery.
I feel comfortable and convenient to deliver at home because less number of people come at home during delivery. (IDI250102—26-year-old mother) Mothers don’t come for institutional delivery could be feeling reluctant to expose their private parts to healthcare providers at health facility. (FGD3001—a village health worker) I don’t think feeling shy to expose our body is problem here . . . The main problem is due to different kind of labor pain. Some can easily delivery and some takes longer time to deliver . . . some don’t experience any signs thereby people failed to prepare to go to health facility. (FGD3001—a mother who delivered at home)
Theme 3.2: Nomadic Way of Life or Pastoralism
The pastoral nomads of Bhutan migrate with yaks/cattle/sheep to high-altitude zones during summer and descend down to the lower land during winter. Such migratory culture compels pregnant women to deliver in the makeshift huts.
I could not come for any antenatal checkups as I was with our yaks and cattle at the Jangsa. I delivered my baby at the tent/shelter in the pastures where we herd yaks and cattle . . . However, I have no idea how delivering in the health facility benefits us. (IDI250107—20-year-old mother)
Theme 3.2: Restriction of Alcohol Consumption at the Health Centers
Some respondents said that most of the women in their village drink alcohol often, even when they are pregnant. Such pregnant mothers find it difficult to adjust to a health facility where alcohol use is restricted. In addition, pregnant mothers were of the opinion that they could easily deliver without pain under the influence of alcohol.
Some of the women preferred to deliver at home because they can deliver quickly at ease with the use of alcohol. (FGD2501—a mother who delivered at home)
Theme 3.4: Inability to Perform Rituals
Some said that they had to perform rituals prior to leaving to health facility for delivery. It is their belief that they have to attend rituals before they venture on a long journey.
I have planned to deliver my baby in National Referral Hospital in Thimphu. But I have been bit late while preparing to perform rituals before leaving for Thimphu. I delivered at home. (IDI300203—24-year-old mother)
On one account, a woman said that she went home from the health center, with a plan to return to the health center for delivery. She first needed to perform some rituals so the baby could be delivered without any complications. However, she delivered at home. Some parents seem to be persuading their daughters to deliver at home, based on their own poor knowledge, attitude, and past practice.
Our parents say that the delivery can easily be conducted at home. They perform rituals for this at home. (IDI300106—23-year-old mother) While Rimdos (rituals) should be performed hand in hand with health care, we have to make every effort to bring all pregnant mothers to deliver at health center despite challenges such as road connectivity. (FGD3001—Lama, a religious figure)
Theme 3.5: Children Born Out-of-Wedlock
Pregnant mothers with an illegitimate child feel embarrassed to visit a health facility for antenatal checkups unless delivering at home gives rise to complications.
Drang [Child born out-of-wedlock] is a problem. Due to such problem, some pregnancies are revealed only at the time of delivery, which is a big problem for concerned people and health service provision. (FGD3001—a village health worker)
Theme 3.6: Lack of Decision-Making Power
The decision for seeking health care services is often made by the husband and parents, especially in households in rural areas with low socioeconomic status. In such cases, the husband’s and parental influence hinders institutional deliveries.
Another reason is that mostly elderly people in my village say that in their times they could easily delivery at home without visiting health center for once. They say that nowadays there are more hassles of going to health center and people face more problems. In our locality, usually our elderly don’t ask us to go to health center. (FGD3002—a mother who delivered at home) When we get symptoms of labor pain, our parents asked us to wait and say that we can delivery in a while. So when the labor pain is in full swing, it is difficult to walk or carry to the center. (FGD3002—a mother who delivered at home)
For one of the respondents, she said that the place of delivery was determined by the decision of her husband, My husband wanted me to deliver at home because he was drunk that time. My husband drinks and never listens. (IDI250202—30-year-old mother)
Theme 3.7: Confidence Gained From Normal Previous Births
Almost all previous deliveries of the respondents had taken place at home. Most mothers said that they could deliver at home without any difficulty as they did not face any complications in their previous delivery.
I had easy delivery without labor pain previously as well as this time. (IDI210202—36-year-old mother) I don’t prepare to come to deliver in the BHU [Basic Health Unit; now renamed as PHC]. My mother also delivered at home. (IDI250101—20-year-old mother) I tell women to go to PHC for delivery. Parents do not support institutional delivery saying that they delivered easily in the villages in the past. (FGD2102—Tshogpa, a local leader)
Theme 4: Knowledge and Awareness
None of the women who delivered at home could explain the benefits of an institutional delivery. Rather they were of the opinion that a home delivery is safe both for themselves and the newborn.
Theme 4.1: Inaccuracy of the Given Expected Date of Delivery (EDD)
Many women who delivered at home did not know their EDD. Of those who knew their EDD, some were not accurate and some of them had an unexpected preterm delivery.
Expected date of delivery is not accurate. I had a labor pain at 5 We could not go to health center because it was night. I had a labor pain at around 12 midnight and delivered in about 2 minutes. (IDI300102—34-year-old mother) In certain cases, the mothers immediately delivery without sign of much pain . . . so there is no time to prepare. (FGD3001—Tshogpa, a local leader)
Discussion
This study sheds light onto 15 barriers to institutional delivery in Bhutan. Some of the barriers identified in this study were not reported in any other studies so these factors could be unique to Bhutan and similar settings. These possibly unique barriers include difficulty in reaching health care centers for nomadic groups who migrate seasonally with their herds, the restriction of alcohol consumption at health centers, hesitancy to avail care in cases of pregnancy out of wedlock, and fear of hypothermia in cold places.
Women pregnant with unidentified fathers not only do not turn up for institutional delivery, but they also do not come forward to seek health services like antenatal clinics. Some of the nomadic herders have given birth, while they were with herds away from human settlements. Their pasturelands are usually very far away from the health centers, making it difficult for the herders to visit health centers and for the health care providers to reach them. Blockages of roads or footpaths by landslides and swollen rivers during the rainy season were pointed out as reasons for not being able to come for institutional delivery by some of the participants. Barriers like those mentioned above require multisectoral approaches to overcome them.
Although two quantitative studies4,5 were conducted in Bhutan to study the factors associated with low institutional deliveries, this is the first qualitative study on the topic. This study corroborates the findings of other studies conducted elsewhere on barriers related to human resources,6-8 services,6,7,9 distance, terrain, and transportation,6,7,10,11 economic hardship and handling domestic chores,6-10 feeling shy,7,11 traditional practices,6,7,9 decision-making power,6,7,10 awareness, and low-risk perception,6,7,9,10 Almost all previous deliveries of the respondents had taken place at home. Most mothers said that they did not face any complications in their previous delivery. This finding supports the findings of the quantitative study carried out in Chukha Bhutan in 2012 4 and those conducted elsewhere. 16
Bhutan is in an advanced stage to launch the “accelerating mother and child health care—1000 golden day plus allowance.” This conditional cash transfer mechanism is expected to boost achievements in institutional delivery and other related indicators such as exclusive breastfeeding. 17 However, it may not address the issue of inequity as per Indonesian experience. 18
Following are some of the recommendations to overcome the barriers to institutional deliveries highlighted by this study: (1) Simple needs-based interventions such as improving the heating system and providing warm clothes to be used after being discharged from the health centers coupled with awareness on the importance of an institutional delivery could encourage women in cold places to come to health centers for their delivery. (2) Community support for taking care of household chores, particularly in those households with fewer household members, while the women go to the health centers for their delivery should be encouraged. (3) Given that almost all women visit health care centers for at least one antenatal care (ANC) visit, health care providers should make extra efforts to convince the women to come for institutional delivery. A birth preparedness plan is supposed to be prepared during the ANC visit. However, it was observed during the field visit that the birth preparedness plan was not taken seriously by many health care providers. There was inadequate involvement of the women and/or their husbands during the birth preparedness planning. The birth preparedness plan was done as a 1-time event in the first ANC visit but the follow-up on the birth preparedness plan was usually not done. Therefore, the birth preparedness plan should be reviewed and strengthened. It should focus on plans for institutional delivery, transportation, food, lodging, and an alternative for taking care of household chores. The practice of required follow-up on birth preparedness plan at 36th weeks should be ensured to capture changes, if any, as well as to remind the women to have an institutional delivery. (4) Although all health care centers, excluding sub-posts, are supposed to have a minimum of two health care providers, there is only one in many health centers. Such health care centers often remain closed, resulting in home deliveries. Therefore, efforts to staff all health care centers adequately needs to be ensured. (5) Every health care center, excluding the sub-posts, has a separate physical structure to be used as a kitchen. However, these structures are either used as storage or simply kept locked. Therefore, even if the government cannot provide meals like in bigger health care centers, the kitchens at health care centers in rural areas should remain open and be provided with cooking utensils so that people can prepare meals during their stay.
One of the limitations of this study, like most qualitative studies, is that of small sample size; and therefore, the findings cannot be generalized to the whole target population. However, in-depth information and variation in views were explored and exposed by this study. Other limitations of the study include the following: the sociodemographic details of the participants of the FDG were not collected and comparative analysis of responses from the IDIs and the two types of FDGs are not presented in this article. The number of IDIs and FGDs were predetermined by the authors, and all predetermined IDIs and FGDs were conducted. Nonetheless, data coding and analysis showed that the data saturation was achieved at 37th IDI as no new information or themes emerged from the remaining 13 respondents of the IDIs.
Conclusion
This study sheds light on at least 15 barriers for institutional deliveries. Implementation of the recommendations of this article coupled with the benefits of the conditional cash transfer through the newly initiated “accelerating mother and child health program” has a huge potential to improve the institutional delivery coverage in Bhutan.
Supplemental Material
InstitutionalDeliveyQualitativeStudy_IDIandFGDguides_V02 – Supplemental material for Barriers to Institutional Delivery Services in Districts With the Lowest Institutional Delivery Coverage in Bhutan
Supplemental material, InstitutionalDeliveyQualitativeStudy_IDIandFGDguides_V02 for Barriers to Institutional Delivery Services in Districts With the Lowest Institutional Delivery Coverage in Bhutan by Mongal Singh Gurung, Sonam Wangdi, Pema Lethro, Tashi Tshomo, Tashi Dema and Dorji Pelzom in Asia Pacific Journal of Public Health
Footnotes
Acknowledgements
The authors would like to thank Dr Phillip Erbele and Dr Krista Erbele for their critical review of the article and UNFPA Bhutan for the financial support.
Authors’ Note
The datasets (transcripts) used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Author Contributions
MSG made substantial contributions to conception and design, analysis and interpretation of data, drafting the manuscript, and revising manuscript critically for important intellectual content. SW made substantial contributions to conception and design, acquisition of data, and revising manuscript critically for important intellectual content. PL made substantial contributions in acquisition of data, analysis and interpretation of data, and revising manuscript critically for important intellectual content. TT made substantial contributions to conception and design, and revising manuscript critically for important intellectual content. TD made substantial contributions to analysis and interpretation of data, and revising manuscript critically for important intellectual content. DP made substantial contributions to analysis and interpretation of data, and revising manuscript critically for important intellectual content. All authors read and approved the final manuscript as well as agreed to be accountable for all aspects of the work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The UNFPA Country Office for Bhutan funded the study. However, the funder had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.