
Abstract
While health literacy research in mainland China has gained increasing attention, most studies focus on adults. This study aimed to examine the mediating role of health literacy in the relationship between a range of upstream factors and health behaviors among Chinese secondary students. A cross-sectional study was conducted with 650 students in Years 7 to 9 from four secondary schools in Beijing. Based on an adapted health literacy framework from Manganello, a self-administered questionnaire was designed to collect information on upstream factors, health literacy, and health behaviors. Path analysis results showed that the proposed framework was mostly supported by empirical data after modification indices were examined and 3 direct paths were added. Students’ self-efficacy, social support, and school environment were associated with health literacy, which in turn predicted health behaviors. A holistic approach is needed to improve both adolescent health literacy and health behaviors for Chinese school-aged adolescents.
What We Already Know
Low health literacy is prevalent in Asia Pacific countries.
Improving health literacy at an early age is crucial to personal empowerment and results in better health outcomes.
There are few theory-driven empirical research studies regarding adolescent health literacy in mainland China.
What This Article Adds
Adolescent health literacy was observed as a mediator between a set of social-ecological factors (self-efficacy, social support, and school environment) and health behaviors.
The role of health literacy as a mediator of upstream factors differed according to the behavior under investigation.
Introduction
Health literacy is a key public health concept that represents an individual’s capacity to engage with health information successfully.1,2 It is a personal asset that enables an individual to take control of health determinants, and also a measurable outcome for national health. 3 As suggested in Nutbeam’s health promotion outcome model, 4 health literacy can be improved by a variety of health promotion actions including education and advocacy. Currently, low health literacy is common among adults in Asia Pacific countries, ranging from 28.2% in Myanmar to 92.7% in Laos. 5 Many countries have taken actions to improve health literacy and reduce health disparities at the community and national level. 1
In mainland China, the concept health literacy was first introduced in 2008 by the Department of Health through a public bulletin titled “Basic Knowledge and Skills of People’s Health Literacy.” 6 Since then, a number of studies have been conducted to examine health literacy and its impact, particularly among adults.7,8 But adolescent health literacy is also essential. First, low health literacy is prevalent in Chinese adolescents, ranging from 24% to 86%.9,10 Second, improving health literacy at an early age is crucial to personal empowerment and results in better health outcomes. 11 Health literacy interventions that target adolescents have already shown promising outcomes such as improved healthy behaviors and reduced personal stigma. 12
While previous research suggested health literacy as a mediator between upstream factors and health outcomes, most focused on socioeconomic status as a precursor and self-reported health status as an outcome.13,14 In addition, health literacy was primarily measured from a functional perspective (ie, basic health skills in reading and understanding) and the interactive and critical domains (eg, communication, evaluation skills) were not included. 4 There is limited theory-driven empirical research regarding the mediating role of adolescent health literacy in the relationship between upstream factors and health outcomes.9,10,15
In the field of adolescent health literacy, more than 20 theoretical models have been proposed. 16 Using a theoretical model can assist researchers in understanding what health literacy is and how it relates to its antecedents and health outcomes, which is essential for informing effective responses to low health literacy. In the present study, we used Manganello’s framework 11 as a guide to examine how health literacy was related to a range of upstream factors and health behaviors in Chinese school-aged adolescents.
Manganello’s framework postulates that health literacy mediates the relationship between a range of upstream factors and health outcomes. 11 Upstream factors such as interpersonal relationships predict adolescents’ health literacy, which in turn affects their health behaviors. We made several adaptations to the framework (see Appendix 1 for details, available online). In brief, we selected key elements within the framework to meet our research aim and target population.17,18 We did not include outcomes such as health costs and health service use because adolescents are dependent on their guardians for health care, which may result in self-report bias. Based on the adapted framework (see Figure 1A), we formulated 5 hypotheses:
Hypothesis 1: Sociodemographics would predict self-efficacy, health literacy, social support, and perceptions of school environment and community environment.
Hypothesis 2: Self-efficacy would predict health literacy.
Hypothesis 3: Social support would predict self-efficacy, health literacy, and health behaviors.
Hypothesis 4: Perceptions of school environment and community environment would predict self-efficacy, health literacy, and health behaviors.
Hypothesis 5: Health literacy would predict health behaviors.
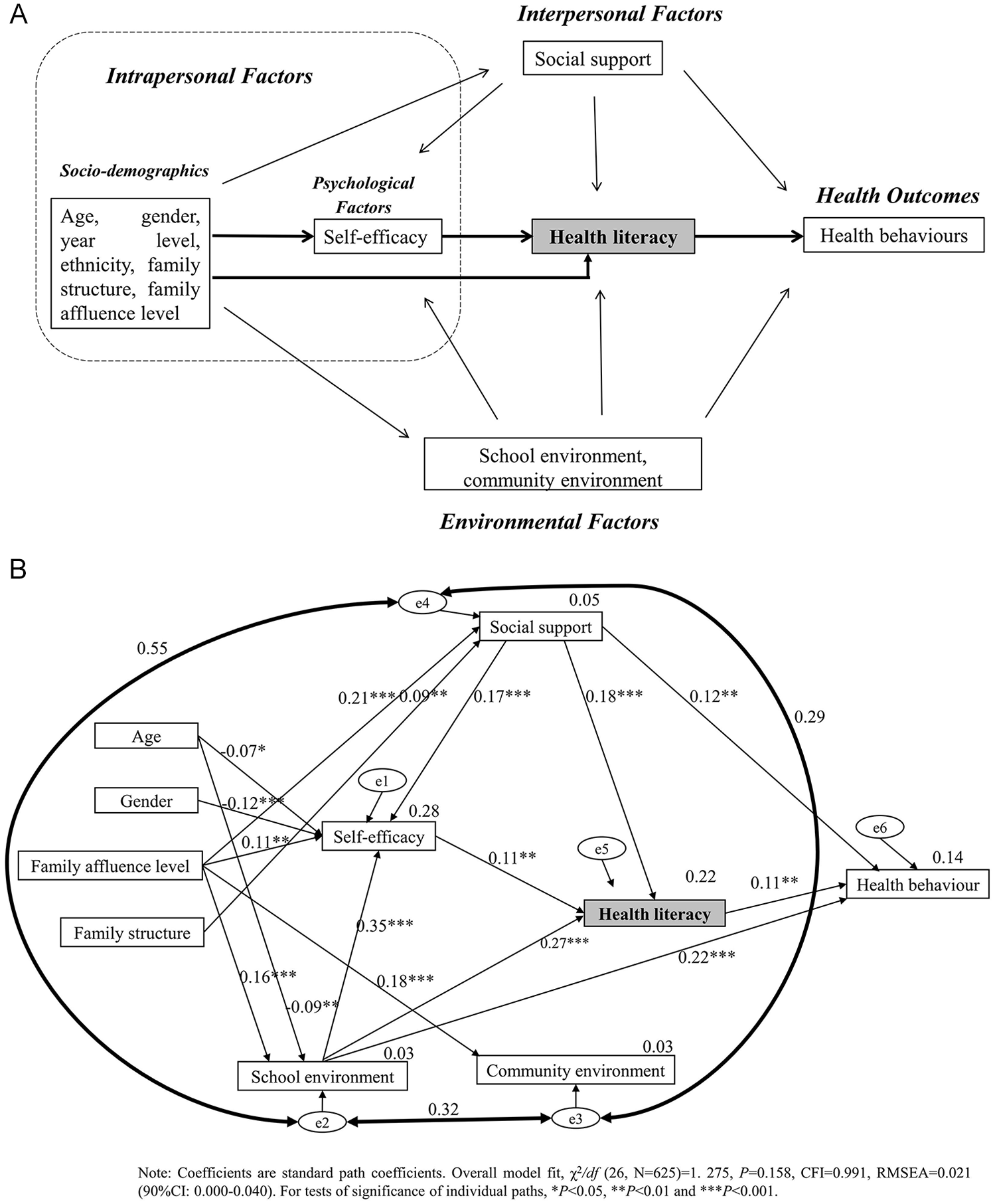
The pathway model linking adolescent health literacy to health behaviors, based on the adapted framework from Manganello.
Methods
Participants and Settings
A cross-sectional study was designed to recruit adolescents from secondary schools in two districts of Beijing, China, using convenience sampling. Two districts were selected according to their socioeconomic levels, one representing high and the other representing low. Based on our previous successful collaborations with schools in each district, 19 we selected two schools according to the appropriateness of survey timing (class time, class break time, or lunchtime). At each school, students in two whole classes (ranging from 20 to 35 students) from each of the year levels 7, 8, and 9 were invited to complete a self-administered questionnaire. This study was approved as “low-risk” research in Chinese secondary school settings. Passive, opt-out consent was obtained from both parents and students. Based on measurement theory, 20 the minimum sample size required was 400. Data collection was undertaken in November 2015.
Questionnaire
An English version questionnaire was first designed based on the adapted framework to collect information on health literacy, upstream factors, and health behaviors (see Appendix 2 for detailed measures, available online). The questionnaire was then translated into Chinese using a “translation, back-translation” technique. In total, there were 7 parts (You and Your Family, Your Personal Health, Your Health Behaviors, Your Literacy Skills, People in Your Life, Your School and Community, and Your Health Skills), with each part having 5 to 47 questions. A research investigator, rather than a teacher, was present during the completion of the survey to answer students’ questions. The average time to complete the survey was 25 minutes.
Intrapersonal Factors
Intrapersonal factors included sociodemographics and self-efficacy. Sociodemographics included age, gender (male or female), ethnicity (Han or ethnic minorities), year level (Years 7, 8, or 9), family structure (living with two biological parents or other living arrangements), and family affluence level measured by the Family Affluence Scale (low, medium, or high). 21 Personal self-efficacy was measured by the General Self-Efficacy Scale (GSES), 22 a 10-item scale that assesses personal belief in the ability to cope with a variety of life challenges. Respondents indicated their level of agreement on a 4-point scale (1 = not at all true, 4 = exactly true). The GSES total score range is 10 to 40, with higher scores indicating higher levels of self-efficacy.
Interpersonal Factors
Interpersonal factors were assessed using the Multidimen-sional Scale of Perceived Social Support (MSPSS), 23 a 12-item scale that measures an individual’s perceived support from family, friends, and significant others. Respondents answered each item on a 7-point Likert-type scale (1 = very strongly disagree, 7 = very strongly agree). The MSPSS total score range is 12 to 84, with higher scores reflecting higher levels of social support.
Environmental Factors
School environment was assessed by the School Environment Scale (SES), which is derived from the Communities That Care Youth Survey. 24 The SES comprises 10 items measuring students’ subjective feelings about opportunities and rewards for prosocial involvement at school. Respondents indicated their level of agreement with each statement on a 4-point Likert-type scale (1 = strongly disagree, 4 = strongly agree). The SES total score range is 10 to 40, with higher scores suggesting stronger bonds of attachment to school.
Community environment was assessed by the Community Environment Scale (CES), which measures respondents’ subjective feelings of their neighborhood environment such as cleanliness and safety. 25 The CES consists of nine items in three domains: neighborhood livability, neighborhood facilities, and traffic. Participants answered each item on a 5-point scale (1 = strongly disagree, 4 = strongly agree; 0 = do not know). The CES total score range is 0 to 36, with higher scores indicating a more livable and supportive community.
Health Literacy
Health literacy was assessed using the Chinese version 8-item Health Literacy Assessment Tool (HLAT-8) that measures an individual’s ability to access, understand, evaluate, and communicate health information in everyday life. 20 The HLAT-8 total score range is 0 to 37, with higher scores indicating higher levels of health literacy.
Health Behaviors
Health behaviors were measured by 5 items derived from previously well-established student health and well-being surveys. 26 They included the following: the frequency of breakfast eating (“During the past 7 days, how often did you have breakfast?” 1 = 0 days; 8 = 7 days), physical activity (“During the past 7 days, on how many days were you physically active for a total of at least 60 minutes per day?” 1 = 0 days; 8 = 7 days), cigarette smoking (“On how many occasions have you smoked cigarettes in the last 30 days?” 1 = never; 7 = 40 times or more), alcohol drinking (“On how many occasions have you drunk alcohol in the last 30 days?” 1 = never; 7 = 40 times or more), and teeth brushing (“How often do you brush your teeth?” 1 = never; 5 = more than once a day). The total score for health behaviors ranged from 5 to 35, with higher scores indicating more health-promoting behaviors.
Statistical Analysis
All statistical analyses were conducted using SPSS 22.0 (IBM Corp, 2013) and AMOS 23.0 (IBM Corp, 2015). Descriptive statistics (frequency/percentage, mean, median) were used to examine participants’ sociodemographics and each scale. Univariate analysis (t test, ANOVA [analysis of variance], nonparametric test) and correlation analysis (Pearson and Spearman correlation analysis) were conducted before path analysis, which was conducted using the maximum likelihood method. Model fit was examined with the relative χ2 goodness-of-fit statistic (χ2/df [degrees of freedom]), comparative fit index (CFI), Tucker and Lewis’s index of fit (TLI), and root mean error of approximation (RMSEA). An acceptable model fit was considered when the χ2/df statistic ≤3, CFI values ≥0.95, TLI values ≥0.95, and RMSEA values ≤0.08. 27
The individual mean substitution was conducted for nonresponse items in self-report scales. The percentages of missing items for the GSES, MSPSS, SES, CES, HLAT-8, and health behaviors ranged from 0.9% to 1.8%, 0.9% to 2.0%, 0.9% to 1.7%, 2.5% to 2.9%, 0.2% to 0.6%, and 0.2% to 0.5%, respectively. Data normality were assessed using skewness and kurtosis values. Results showed that only scores on self-efficacy, health literacy, and school environment were distributed normally, whereas scores on social support, community environment, and health behaviors showed nonnormal distribution.
Results
Participant Characteristics and Descriptive Statistics of Each Scale
In total, 650 students completed the survey, with only 11 students declining, a response rate of 98.3% (650/661). The mean age of participants was 13.42 ± 1.01 years (range = 11-17 years). The distributions of gender, year level, ethnicity, family structure, family affluence level, and descriptive statistics of each scale are shown in Table 1. In our sample, Cronbach’s α of each measurement scale ranged from 0.79 to 0.93, indicating satisfactory reliability.
Participants’ Sociodemographics and Descriptive Statistics of Measured Scales.
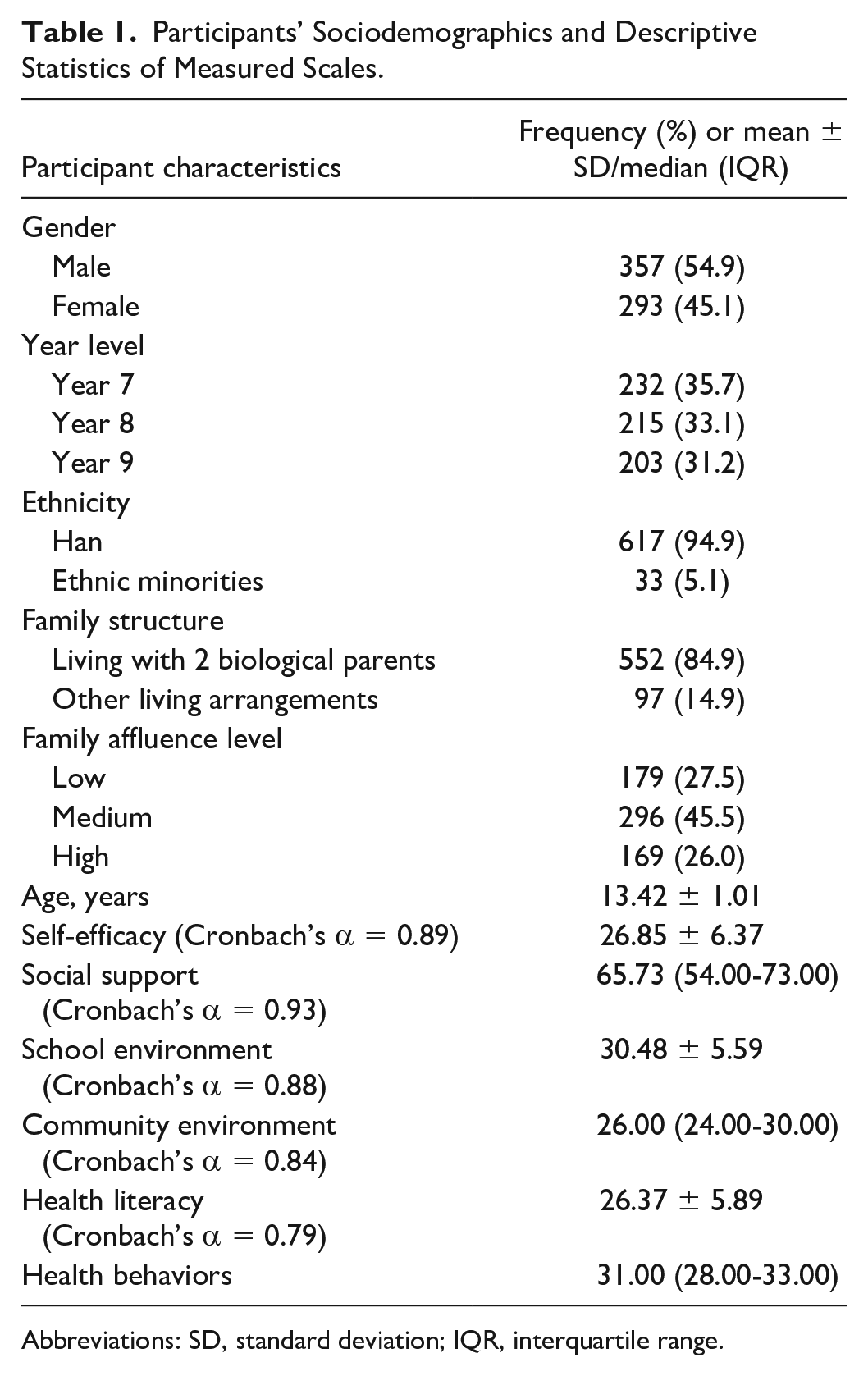
Abbreviations: SD, standard deviation; IQR, interquartile range.
Univariate and Correlation Analyses
Table 2 shows score differences in self-efficacy, social support, school environment, community environment, and health literacy by participant characteristics. Students were more likely to have high self-efficacy if they were male, came from lower year levels, lived with two parents, and came from high-affluence families. Likewise, students who lived with two parents and came from high-affluence families were more likely to have high scores on social support and school environment. Students with a high level of family affluence were more likely to have high scores on community environment and health literacy. Health literacy and health behaviors were positively correlated with self-efficacy, social support, school environment, and community environment (r = 0.25-0.43, P < .01; see Appendix 3, available online).
Univariate Analysis of Self-Efficacy, Social Support, School Environment, Community Environment, and Health Literacy by Participant Characteristics.
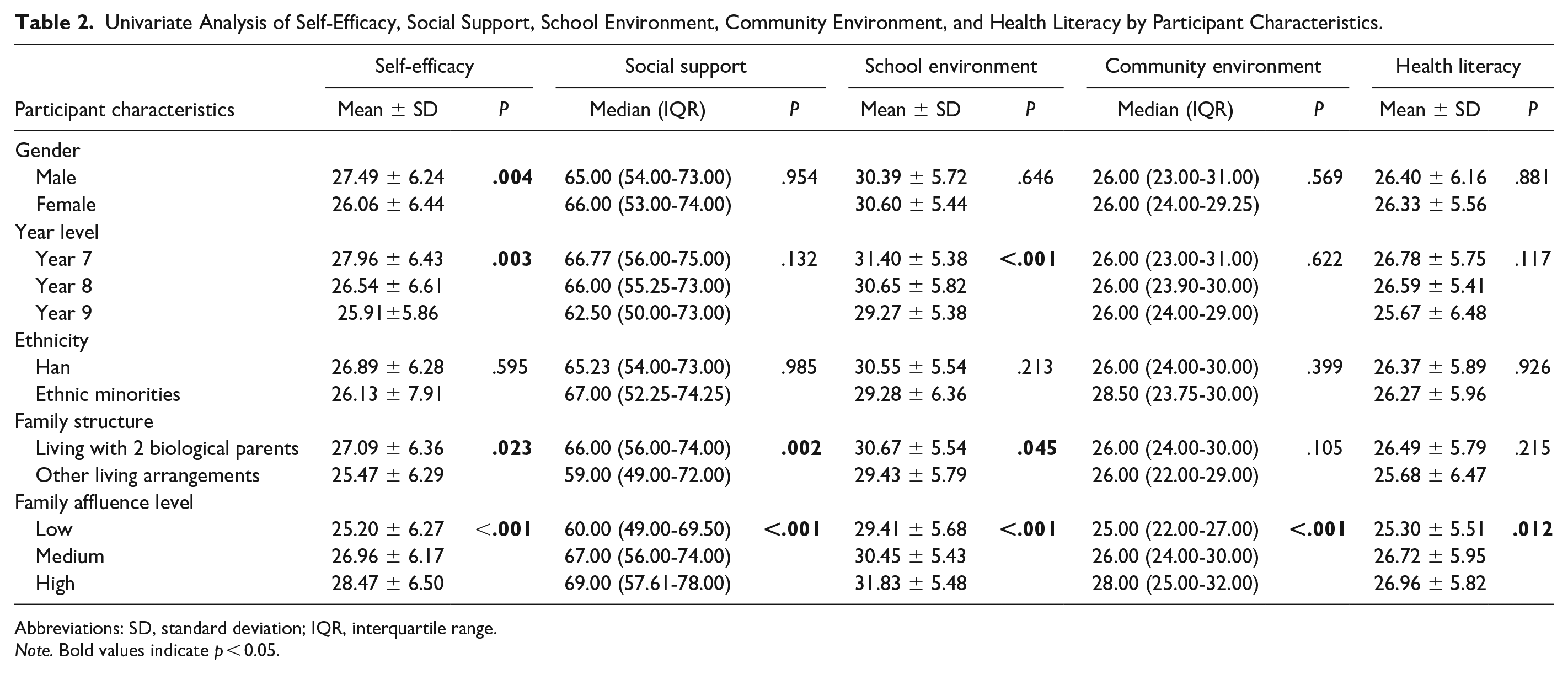
Abbreviations: SD, standard deviation; IQR, interquartile range.
Note. Bold values indicate p < 0.05.
Path Analysis
After univariate and correlation analyses, all significant independent variables related to health literacy or health behaviors were considered for next-step path analysis. The original path model demonstrated poor data fit: χ2/df (23, n = 625) = 14.163, P < .001, CFI = 0.630, TLI = 0.277, RMSEA = 0.145 (90% confidence interval [CI] = 0.131-0.159), but the path from health literacy to health behavior was significant (r = 0.11, P = .008). Examination of modification indices suggested that the model fit could be improved by connecting errors between social support and school environment, between school environment and community environment, and between social support and community environment (see Appendix 4, available online), represented by the bold, double-headed arrows in the trimmed model in Figure 1B. The final trimmed path model demonstrated excellent data fit: χ2/df (26, n = 625) = 1.275, P = .158, CFI = 0.991, TLI = 0.985, and RMSEA = 0.021 (90% CI = 0.000-0.040).
In the final trimmed path model, there were significant and direct paths from self-efficacy (r = 0.11, P = .007), social support (r = 0.18, P < .001), and school environment (r = 0.27, P < .001) to health literacy, and from health literacy (r = 0.11, P = .006) to health behavior. Additional significant paths are shown in Appendix 5 (available online). Based on the squared multiple correlation coefficients (r2), the final trimmed model explained 28% of the variance in self-efficacy, 22% of the variance in health literacy, and 14% of the variance in health behavior. Using the final trimmed path model, we also examined each type of health behavior (see Appendix 6, available online). Results showed that only the physical activity and teeth brushing path models were found to have a good fit for both overall model assessment and individual parameter estimation. There were significant paths from health literacy to physical activity (r = 0.14, P = .002) and teeth brushing (r = 0.10, P = .018), whereas paths from health literacy to breakfast eating (r < .01, P = .920), cigarette smoking (r = 0.01, P = .756), and alcohol drinking (r = 0.06, P = .187) were not significant.
Discussion
This cross-sectional study tested a path model linking health literacy to health behaviors among Beijing secondary school students. Most findings were consistent with our hypotheses: (1) sociodemographics predicted self-efficacy, social support, and perceptions of school and community environment but were not directly related to health literacy; (2) self-efficacy predicted health literacy; (3) social support predicted self-efficacy, health literacy, and health behaviors; (4) perceptions of school environment predicted self-efficacy, health literacy, and health behaviors; and (5) health literacy predicted health behaviors.
Our univariate analysis results showed that only the family affluence level was associated with health literacy. Unexpectedly, there was not a direct relationship between sociodemographics and health literacy in the path model. While previous studies suggest that health literacy is a mediator of the relationship between socioeconomic status and health outcomes,13,14,18 our findings were not consistent. One explanation is that we investigated health literacy in secondary students with a narrow age range and similar backgrounds (eg, socioeconomic status). More representative samples of adolescents are needed in future to examine the pathway from sociodemographics through health literacy to health outcomes. However, an indirect effect was observed through self-efficacy, social support, and school environment, suggesting that these are more proximal predictors of health literacy. While actions to improve upstream social determinants are important for long-term improvements to health, our findings suggest significant opportunities to improve health outcomes by addressing shorter-term factors such as personal self-efficacy.
This study extends what is known about the relationship between self-efficacy and health literacy in adolescents. Previous research suggested a pathway from health literacy through self-efficacy to health behaviors. 28 However, we found a pathway from self-efficacy via health literacy to health behaviors. The difference may be the result of the different populations assessed; much of the previous research focuses on patients with chronic diseases. 28 Due to frequent interactions with the medical system, patients with chronic diseases are more likely to have high self-efficacy to change unhealthy behaviors, provided they have adequate health literacy to follow medical advice. 28 By contrast, school-aged adolescents are relatively healthy and therefore less likely to have therapeutic motivations for changing unhealthy behaviors. In this case, the role of self-efficacy in predicting health behaviors might be not as influential as it is in patients with chronic diseases. Given the current study only used cross-sectional data, our findings are not definitive about the causal relationship between self-efficacy and health literacy. Further research is needed, using longitudinal cohorts to confirm this causal pathway.
We also found that students’ health literacy was influenced by self-efficacy, social support, and school environment. While the original model fit was not satisfactory, we made modifications based on the social-ecological framework, 17 which suggested that social support, school environment, and community environment all influenced students’ health literacy. Our findings indicate that intervening on adolescent health literacy should not rely on a single strategy but within a broader multipronged strategy. Specifically, we found that adolescent health literacy relied more on social support than on personal self-efficacy. Compared with adults, adolescents are more likely to seek support from peers and parents when addressing health issues. The school environment is another determinant because it is the primary place where students develop health literacy. 12 However, we did not find associations between community environment and health literacy or health behaviors. One possible reason is the limited community environment measurement used; it focuses on neighborhood livability and facilities (eg, parks, roads, and traffic lights), 25 and excludes social capital and socioeconomic status. There is a need to investigate other components of community environment and their impacts on health literacy.
Consistent with previous studies targeting adults,13,14 this study found that adolescent health literacy mediated relationships between upstream factors and health behaviors, albeit differentially. This suggests that increasing health literacy could be an effective strategy for improving healthy behaviors, which may, in turn, help reduce chronic disease risks. In the Asia Pacific region, noncommunicable diseases are the leading cause of disease burden, and major behavioral risk factors include inadequate physical activity, cigarette smoking, and alcohol drinking. 29 It is, therefore, important to combat noncommunicable diseases at an early age. 30 Specifically, we found a pathway from health literacy to physical activity and teeth brushing, respectively, but not to breakfast eating, cigarette smoking, and alcohol drinking. The difference in the mediating role of health literacy suggests that improving health literacy may have a varying effect on different health behaviors. Researchers may consider integrating health literacy as an effective component into their intervention strategies when they aim at improving students’ physical activity and teeth brushing.
Several study limitations should be noted. First, our findings are based on cross-sectional data. Further research using a longitudinal design is needed to confirm our findings. Second, convenience sampling may limit the generalizability of our findings. Our sample was recruited from secondary schools in a metropolitan city where the ability of subjects to access good education might be higher than the general population. There is a need to recruit more representative samples with diverse sociodemographic backgrounds. Third, we only used health behaviors as outcomes of interest. Future research may consider using other indicators such as patient-provider communication and health-related quality of life. Fourth, some measurement scales (e.g. community environment) were not validated in our samples. We only provided internal consistency for each scale. Finally, self-report bias may exist for health literacy and other measurement scales. Future research may consider using different formats of data collection to verify whether such measurement bias exists.
Conclusions
This cross-sectional study found that the proposed health literacy framework was mostly supported by the empirical data after modification indices were examined and three direct paths were added. Students’ self-efficacy, social support, and school environment were associated with health literacy, which in turn predicted health behaviors. In addition, the mediating effect of health literacy was found to vary, depending on the behavior under investigation. A holistic approach is needed for promoting students’ health literacy and health behaviors, which, in turn, help foster healthy lifestyles and reduce chronic disease risks.
Footnotes
Acknowledgements
We are grateful to the directors of the Health Care Institute of Primary and Secondary School in Xicheng District and Tongzhou District in Beijing, and we thank all the teachers and participants who were involved in the field study.
Authors’ Note
Data are not publicly accessible; for data access queries or requests please contact the corresponding author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Approval to conduct this research was granted by the University of Melbourne Human Research Ethics Sub-Committee (Ethics Number: 1442884) and the Peking University Health Science Centre Institutional Review Board (Ethics Number: IRB00001052-15024).