
Abstract
The objective of this study was to investigate the association between adherence to healthy lifestyles (as measured by the healthy lifestyle index [HLI]) and depressive symptoms among staff members at a large national medical institution in Tokyo, Japan, during the coronavirus disease 2019 (COVID-19) pandemic. The study sample consisted of 1228 staff members aged between 21 and 73 years who participated in a cross-sectional survey conducted in July 2020. We constructed the HLI by assigning one point to each healthy lifestyle factor: normal body mass index, sufficient physical activity, non-smoking status, non-to-moderate alcohol consumption, and sufficient sleep duration. The multivariate adjusted odds ratios for depressive symptoms were 1.00 (reference), 0.71, 0.66, and 0.56 for participants with HLI scores of 0 to 2, 3, 4, and 5, respectively. The present study suggests the role of healthy lifestyles in mental health among hospital staff working during the pandemic.
What We Already Know
The COVID-19 pandemic has imposed a large psychological burden on health care workers.
Healthy lifestyles have been identified as a potential determinant of mental health.
What This Article Adds
This study provides essential evidence on the inverse association between adherence to healthy lifestyles and depressive symptoms in a population of hospital workers, including front-line health care workers, during the COVID-19 pandemic.
The finding of the study suggests the role of healthy lifestyles to prevent and manage mental health issues during the COVID-19 pandemic.
Introduction
The ongoing pandemic of coronavirus disease 2019 (COVID-19), which is caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), has had enormous psychological impacts among health care workers.1 -4 A meta-analysis by Salari et al. 4 reported that the prevalence of depression among front-line health care workers during the COVID-19 pandemic was 24.3%. Health care workers may be at a high risk of depression because of their exposure to stressors related to COVID-19-related work; for instance, working at the front-line, having direct contact with COVID-19 patients, and having an increased workload.3,5,6
Addressing mental health issues during the COVID-19 pandemic requires the investigation of potential contributing factors. Healthy lifestyles have been identified as a potential determinant of mental health. Previous studies have constructed a healthy lifestyle index (HLI; i.e., a single score incorporating various lifestyle factors) and investigated its association with depressive symptoms.7 -14 These studies found that adherence to a greater number of healthy lifestyle factors was associated with a lower prevalence or incidence of depressive symptoms, suggesting a dose-response relationship between healthy lifestyle factors and mental health issues.
The present study builds on previous studies by examining the association between adherence to healthy lifestyles and depressive symptoms among hospital staff including health care workers during the COVID-19 pandemic. While recent studies have focused mainly on the psychological impact of COVID-19 on health care workers,1 -3 the role of lifestyle factors in mental health has not yet been explored. In addition, pandemic-related restrictions on daily living and stressors related to working in the context of the COVID-19 pandemic may have affected the adoption of healthy lifestyle factors among health care workers. Examining the associations between healthy lifestyle factors and depressive symptoms in this population may generate evidence to support public health interventions to prevent and manage mental health issues during the pandemic.
The objective of this study was to clarify the association between adherence to healthy lifestyles and depressive symptoms among staff members of the National Center for Global Health and Medicine (NCGM) in Tokyo, Japan, a medical institution designated for the care of COVID-19 patients and associated research.
Methods
Study Design and Participants
Data for the present study were obtained from the first survey in July, 2020 (after the first wave of epidemic in Japan), of the NCGM Clinical Epidemiology Study on the SARS-CoV-2 antibody, an ongoing epidemiological study involving staff members at the NCGM. 15 The objective of the study was to investigate the prevalence and determinants of SARS-CoV-2 infection. On recruitment, participants were asked to complete an electronic questionnaire on sociodemographic factors, COVID-19-related work factors, lifestyle factors, and depressive symptoms.
Of 1579 staff members who were invited to the survey, 1228 agreed to participate in the survey (response rate = 77.8%). The participants consisted of 353 men and 875 women aged between 21 and 73 years. Written informed consent was obtained from all participants. The study protocol was approved by the NCGM Ethics Committee.
Construction of Healthy Lifestyle Index
We collected information on body mass index (BMI), leisure-time physical activity, smoking status, alcohol consumption, and sleep duration. Based on existing knowledge and recommendations, we classified participants into two groups: low-risk (adhering to a healthy lifestyle) and high- risk (not adhering to a healthy lifestyle).
Self-reported information on body weight and height was obtained via the electronic questionnaire, and BMI was calculated by dividing weight (kg) by the square of the height (m2). We defined the low-risk BMI group as individuals with normal BMI (18.5-24.9 kg/m2) and the high-risk group as underweight (<18.5 kg/m2) or overweight/obese (≥25 kg/m2) individuals. 16 For leisure-time physical activity, participants were asked to report the amount of time each week that they spent engaged in indoor physical activity (e.g., at home, in the gym), outdoor physical activity during the daytime, and outdoor physical activity in the morning, evening, or nighttime. In keeping with the physical activity standards for health promotion released by the Ministry of Health, Labour, and Welfare (MHLW), Japan, in 2013, 17 we defined the low-risk group as individuals who engaged in ≥60 minutes/week of leisure-time physical activity and the high-risk group as <60 minutes/week of leisure-time physical activity. For smoking status, we defined the low-risk group as non-smokers (i.e., smoking neither cigarettes nor heat-not-burn cigarettes) and the high-risk group as current smokers (i.e., smoking cigarettes and/or heat-not-burn cigarettes). 18 For alcohol consumption, we defined the low-risk group as those consuming ≤1 go/day of alcohol (go: a Japanese traditional unit [180 mL]) and the high-risk group as those with alcohol consumption of >1 go/day. These classifications were based on the national health promotion campaign “Health Japan 21” by the MHLW, 19 which suggests that approximately 20 g of ethanol per day (equivalent to 1 go/day of Japanese sake) can be considered moderate alcohol consumption. For sleep duration, we defined the high-risk group as those with short sleep duration (<6 hours/day) and the low-risk group as individuals with sleep duration of ≥6 hours/day. Sleep was included in the HLI because a meta-analysis of seven prospective studies showed a significant association between sleep duration and depression. 20 In the present study, we did not examine the effects of long sleep duration. Possible responses to the question on sleep duration were as follows: <4, 4 to 4.9, 5 to 5.9, 6 to 6.9, 7 to 7.9, or ≥8 hours/day. Further information on sleep duration ≥8 hours/day was unavailable.
For each healthy lifestyle factor, the low-risk group received a score of 1 and the high-risk group received a score of 0. We used these values to compute a composite score ranging from 0 to 5, with higher scores indicating adherence to a greater number of healthy lifestyle parameters (Supplemental Table 1, available online). Since only a small number of participants scored 0 (n = 0) or 1 (n = 21), participants with scores of 0 to 2 were merged into a single reference group. Therefore, the four HLI groups used in our final analyses consisted of individuals with scores corresponding to 0 to 2 (n = 157), 3 (n = 375), 4 (n = 493), and 5 (n = 203).
Assessment of Depressive Symptoms
Depressive symptoms were assessed using a case-finding instrument for depression. 21 The instrument consisted of two questions: “During the past month, have you often been bothered by feeling down or depressed?” (yes or no) and “During the past month, have you often been bothered by little interest or pleasure in doing things?” (yes or no). Previous studies in Japan have shown that this instrument has acceptable sensitivity (75% 22 and 87.9% 23 ) and specificity (88.2% 22 and 81.4% 23 ) for identifying depressive symptoms in participants answering “yes” to both questions. Therefore, participants who responded “yes” to both questions were regarded as having depressive symptoms in the present study.
Other Variables
Information on age (continuous), sex (male or female), and occupation (doctors, nurses, allied health care professional [i.e., health care workers other than doctors and nurses], administrative staff, researcher, or management) were obtained from the labor management office at the NCGM. The electronic questionnaire was used to collect information on the following covariates: living arrangements, comorbid conditions, and COVID-19-related work factors (working hours per day during the outbreak between late-March and mid-April 2020 and degree of possible exposure to SARS-CoV-2).
We grouped occupations into four categories: doctors, nurses, allied health care professionals, and others. Administrative staff, researchers, and management were merged into the “others” category because of the small number of participants for each occupation type. For living arrangements, responses on the number of cohabitants (living alone, living with 1 person, living with 2, 3, 4, or ≥5 people) were used to group participants into two categories: living alone or living with others. The presence of one or more comorbid conditions (yes or no) was based on whether the participant reported any of the following chronic disorders: diabetes, hypertension, chronic obstructive pulmonary disease, heart disease, cerebrovascular disease, cancer, or other chronic diseases. Self-reported working hours (≤6, 7, 8, 9, 10, 11, 12, 13, or ≥14 hours/day) were used to categorize participants into three groups: ≤8, 9 to 10, or ≥11 hours/day. To assess the degree of possible exposure to SARS-CoV-2, the following questions were asked: “Have you ever engaged in COVID-19-related work?” and “Did you engage in any work in which you were heavily exposed to SARS-CoV-2?” Participants were then grouped into three categories: low (those who did not engage in COVID-19-related work), moderate (those who engaged in COVID-19-related work, but with a low level of exposure to the virus), or high (those who engaged in COVID-19-related work with a high level of exposure to the virus).
Statistical Analysis
We determined the frequencies and means of the characteristics according to the HLI category. We then performed multiple logistic regression analysis and calculated the odds ratios (ORs) and corresponding 95% confidence intervals (CIs) for depressive symptoms. We adjusted for age (continuous), sex (male or female), and occupation (doctors, nurses, allied health care professionals, or others) in Model 1. In Model 2, we also adjusted for living arrangements (living alone or living with others) and comorbid conditions (yes or no). In Model 3, we further adjusted for working hours (≤8, 9-10, or ≥11 hours/day) and degree of possible exposure to SARS-CoV-2 (low, moderate, or high).
Additionally, we constructed alternative versions of the HLI in which we omitted one component from the original HLI and adjusted for the omitted component. This approach enabled us to estimate the impact of each component on the association between HLI score and depressive symptoms. Previous studies on this subject also conducted this analysis.7,14
Statistical significance was set as P for trend <0.05 (two-tailed). All statistical analyses were performed using SAS version 9.4 (SAS Institute).
Results
We identified 268 cases of depressive symptoms among 1228 participants (21.8%). Participant characteristics are presented in Table 1. In the present study, 71.3% of the participants were women. The proportions of doctors, nurses, allied health care professionals, and other occupations were 19.3%, 48.9%, 13.8%, and 18.0%, respectively. A total of 66.8% of the participants engaged in any COVID-19-related work.
Characteristics of the Study Participants (n = 1228).
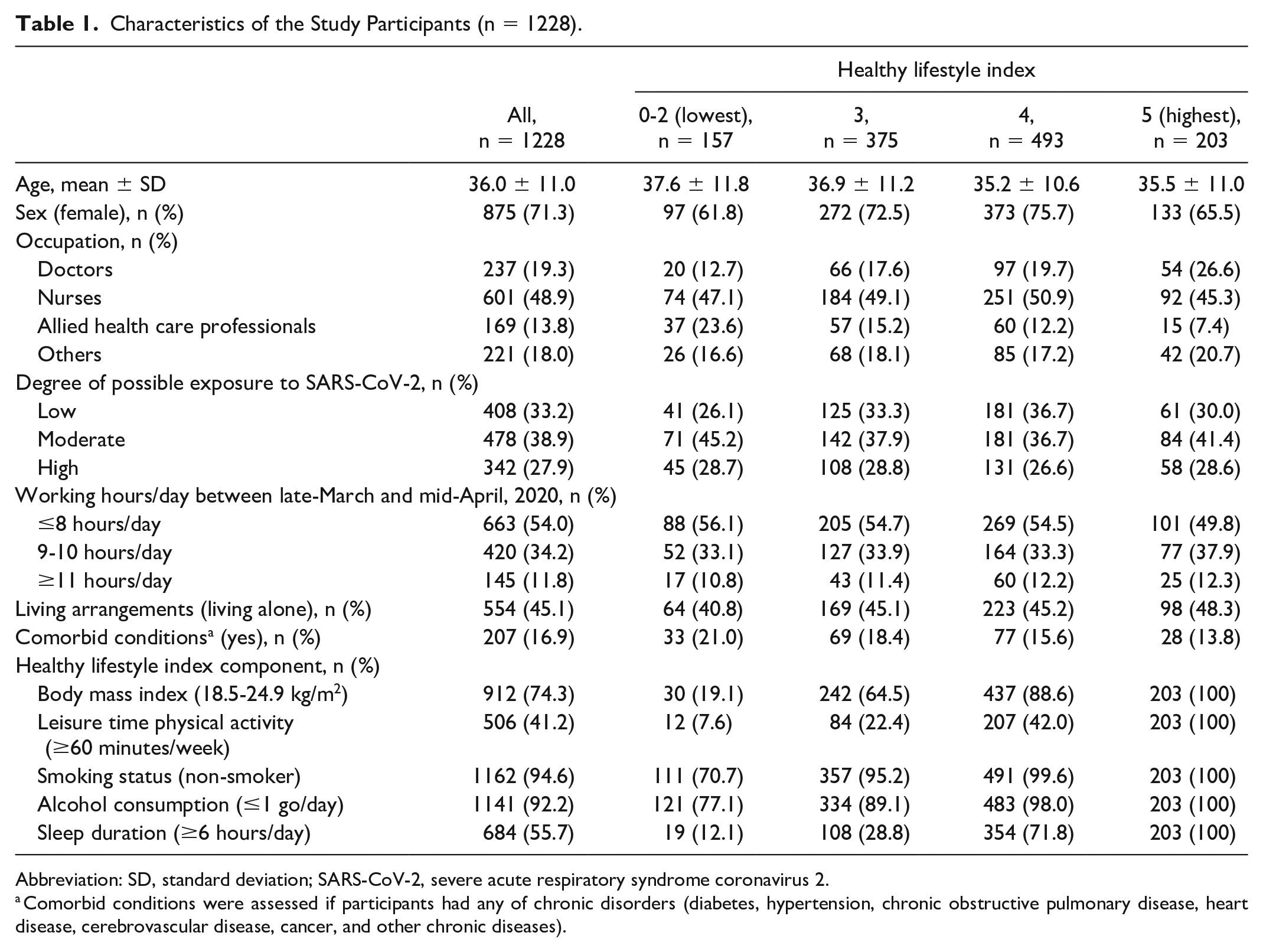
Abbreviation: SD, standard deviation; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2.
Comorbid conditions were assessed if participants had any of chronic disorders (diabetes, hypertension, chronic obstructive pulmonary disease, heart disease, cerebrovascular disease, cancer, and other chronic diseases).
We observed a significant association between HLI score and depressive symptoms (Table 2). In Model 1, the ORs (95% CI) for depressive symptoms were 1.00 (reference group), 0.73 (0.47, 1.13), 0.66 (0.43, 1.01), and 0.57 (0.34, 0.95) for participants with HLI score of 0 to 2, 3, 4, and 5, respectively (P for trend = 0.027). This association remained statistically significant after adjusting for living arrangements and comorbid conditions (Model 2). In Model 2, the ORs (95% CI) for the HLI categories, again in ascending order, were 1.00 (reference), 0.72 (0.46, 1.12), 0.67 (0.44, 1.03), and 0.55 (0.33, 0.93; P for trend = 0.031). After further adjustment for COVID-19-related work factors, the ORs (95% CI) were 1.00 (reference), 0.71 (0.46, 1.11), 0.66 (0.43, 1.01), and 0.56 (0.33, 0.94; P for trend = 0.032).
Odds Ratios and 95% Confidence Intervals of Depressive Symptoms According to the Healthy Lifestyle Index Categories.
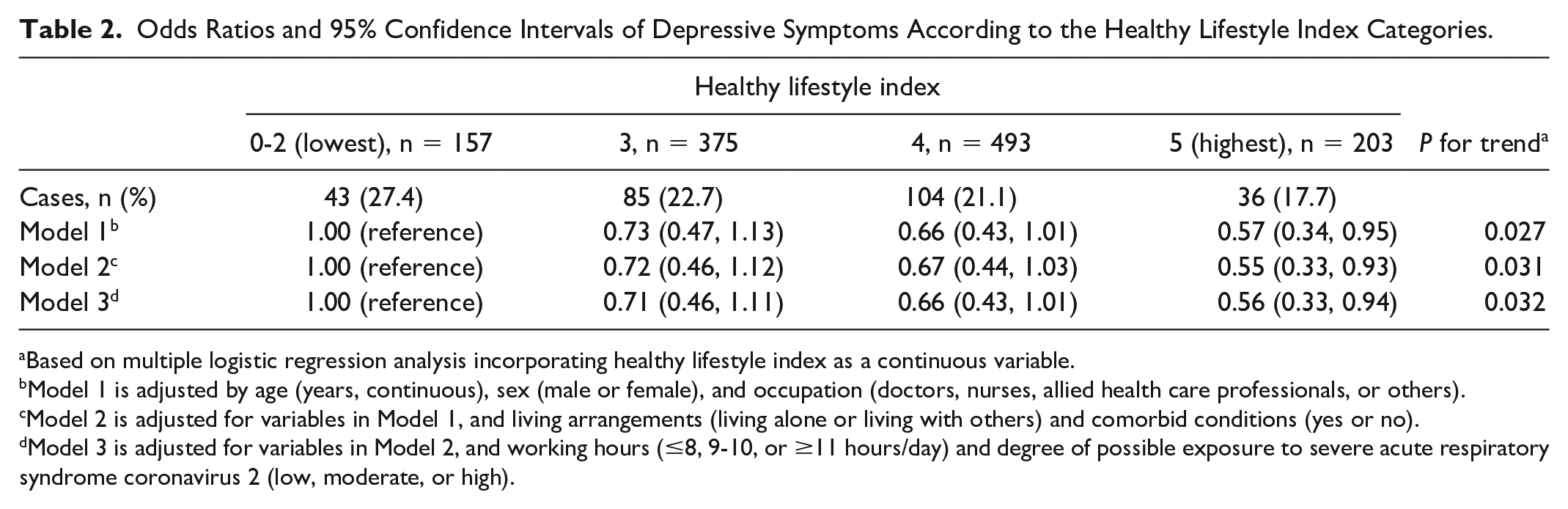
Based on multiple logistic regression analysis incorporating healthy lifestyle index as a continuous variable.
Model 1 is adjusted by age (years, continuous), sex (male or female), and occupation (doctors, nurses, allied health care professionals, or others).
Model 2 is adjusted for variables in Model 1, and living arrangements (living alone or living with others) and comorbid conditions (yes or no).
Model 3 is adjusted for variables in Model 2, and working hours (≤8, 9-10, or ≥11 hours/day) and degree of possible exposure to severe acute respiratory syndrome coronavirus 2 (low, moderate, or high).
Table 3 shows the results of the analysis in which we examined the impact of each HLI component on the association with depression symptoms. The association remained statistically significant when we omitted BMI (P for trend = 0.012), leisure-time physical activity (P for trend = 0.008), and alcohol consumption (P for trend = 0.058) from the HLI. The association became non-significant but did not change in direction when we omitted smoking status (P for trend = 0.052) and sleep duration (P for trend = 0.515) from the HLI. It is noteworthy that the decrease in the OR for depressive symptoms in the group with the highest HLI was attenuated when sleep duration was omitted from the HLI (OR = 0.70; 95% CI = 0.32, 1.53).
Odds Ratios and 95% Confidence Intervals of Depressive Symptoms According to the Alternative Healthy Lifestyle Index Categories.
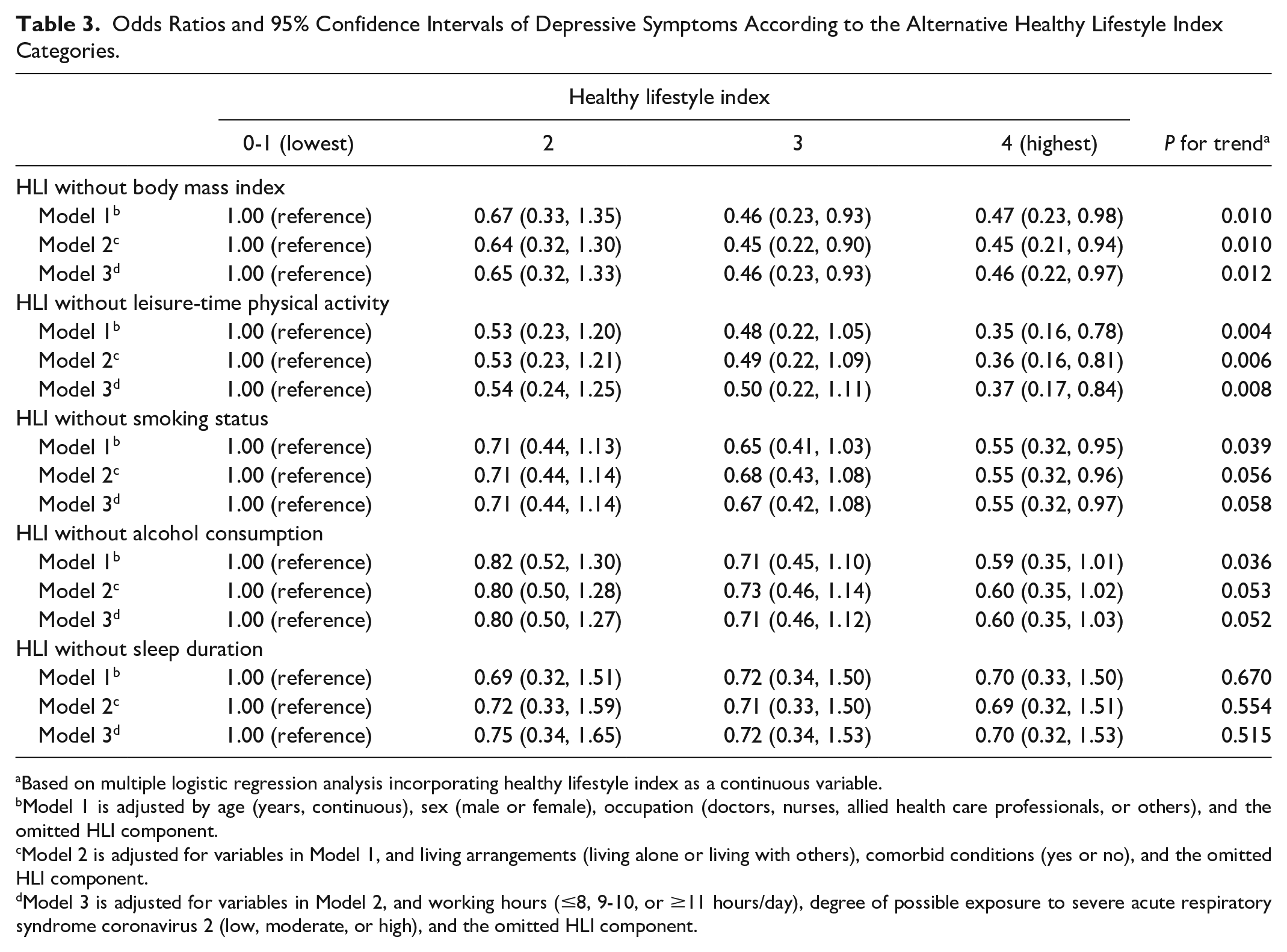
Based on multiple logistic regression analysis incorporating healthy lifestyle index as a continuous variable.
Model 1 is adjusted by age (years, continuous), sex (male or female), occupation (doctors, nurses, allied health care professionals, or others), and the omitted HLI component.
Model 2 is adjusted for variables in Model 1, and living arrangements (living alone or living with others), comorbid conditions (yes or no), and the omitted HLI component.
Model 3 is adjusted for variables in Model 2, and working hours (≤8, 9-10, or ≥11 hours/day), degree of possible exposure to severe acute respiratory syndrome coronavirus 2 (low, moderate, or high), and the omitted HLI component.
Discussion
The present study examined the cross-sectional association between adherence to healthy lifestyle factors and depressive symptoms among staff members in a large national medical institution in Tokyo, Japan, during the COVID-19 pandemic. We found an inverse association between healthy lifestyles and depressive symptoms.
Our findings were consistent with previous studies showing that healthy lifestyle factors play a significant role in mental health in adults,7,9 -12 elderly men, 8 college students, 13 or working population. 14 These studies computed HLI scores using the information on selected lifestyle factors (e.g., BMI, smoking status, alcohol consumption, physical activity, diet, and sleep) and found that higher HLI scores were associated with a lower prevalence or incidence of depressive symptoms. Our study confirmed the findings of previous studies and expanded on them by demonstrating that the association was also present in a population of hospital workers, including front-line health care workers, during the COVID-19 pandemic. We found that the association was significant even after adjusting for COVID-19-related work factors that have been linked to mental health issues.3,5,6 This suggests that adherence to multiple healthy lifestyle factors has a protective effect on the mental health of hospital staff working during the pandemic.
When we investigated the impact of each HLI factor on the association between HLI score and depressive symptoms, we found that the association became non-significant when sleep duration was omitted from the HLI. In addition, the decrease in the OR for depressive symptoms in the highest HLI-score group was attenuated. This suggests that sleep duration is an important contributor to the HLI score and its association with depressive symptoms. This finding is consistent with a previous study that found that sleep duration also contributed to this association. 14 Given that studies have shown that sleep problems (e.g., short sleep duration, poor sleep quality, and sleep disturbance) and mental health issues are prevalent during this pandemic, especially among health care workers,2,24,25 good-quality sleep may be a particularly important lifestyle factor to consider when attempting to prevent depressive symptoms during the COVID-19 pandemic.
Pandemic-related restrictions on daily living, such as social distancing, stay-at-home orders, and restrictions of travels and social gatherings, may have an impact on health-related lifestyle factors. For example, Stanton et al. 26 documented negative changes in health-related lifestyles in Australia: 48.9% of participants reported being less physically active than usual, 40.7% sleeping more poorly than usual, 26.6% reported drinking more than usual, and 6.9% reported smoking more than usual since the onset of the COVID-19 pandemic. They found that these changes were significantly associated with a higher prevalence of depression. Ma et al. 27 also found the association between lifestyle changes (e.g., decreased physical activity, increased alcohol consumption, increased smoking, and increased/decreased body weight) and mental distress in a nationwide cross-sectional survey in China during the COVID-19 pandemic. Special attention should be paid to the role of healthy lifestyle factors in reducing the psychological burden during this critical period. The present study provides evidence suggesting that a healthy lifestyle may reduce depressive symptoms in hospital workers during the COVID-19 pandemic.
The present study had several limitations. First, the cross-sectional design prevented us from determining the direction of the association and inferring causality. We thus could not establish a temporal relationship between lifestyle and depressive symptoms. Second, information on the components of the HLI (e.g., height, weight, alcohol consumption, time engaged in leisure-time physical activity) were self-reported and subject to recall bias. Third, the present study had limited information about diet (e.g., information on fruit and vegetable consumption), and, unlike some studies, we did not incorporate diet into the HLI. Fourth, we did not have information about the intensity of leisure-time physical activity and could not incorporate this into our assessments of physical activity level. Finally, we used a two-question case-finding instrument for depression to determine whether depressive symptoms were present. Although this instrument has been validated and shown to have high sensitivity and specificity, we might have introduced misclassification bias.
In conclusion, this cross-sectional study provides evidence of an association between healthy lifestyle behaviors and depressive symptoms. This finding has important public health implications and may inform the prevention and control of depressive symptoms during the COVID-19 pandemic.
Supplemental Material
sj-pdf-1-aph-10.1177_10105395211007604 – Supplemental material for Association Between Adherence to Healthy Lifestyles and Depressive Symptoms Among Japanese Hospital Workers During the COVID-19 Pandemic
Supplemental material, sj-pdf-1-aph-10.1177_10105395211007604 for Association Between Adherence to Healthy Lifestyles and Depressive Symptoms Among Japanese Hospital Workers During the COVID-19 Pandemic by Ami Fukunaga, Yosuke Inoue, Shohei Yamamoto, Takako Miki, Akiko Nanri, Hironori Ishiwari, Masamichi Ishii, Kengo Miyo, Maki Konishi, Norio Ohmagari and Tetsuya Mizoue in Asia Pacific Journal of Public Health
Footnotes
Acknowledgements
The authors appreciate study participants and staff members of NCGM who supported the study and have been working for the COVID-19 pandemic.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by NCGM COVID-19 Gift Fund and Japan Health Research Promotion Bureau Research Fund (2020-B-09).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.