
Abstract
Keywords
Introduction
Health care personnel (HCP) are at high risk for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) acquisition.1,2 Several studies have been conducted worldwide to determine the prevalence of SARS-CoV-2 antibodies among HCP, with geographic variation in results.1,3 These studies can help identify past infections and gauge the effectiveness of infection control strategies. 3 Pakistan crossed the first peak of the coronavirus disease-2019 (COVID-19) pandemic on June 14, 2020. 4 Through this study, we aimed to determine the seroprevalence of SARS-CoV-2 antibodies, estimate the burden of asymptomatic infections, and explore the association between SARS-CoV-2 antibody positivity, sex, designation, and a history of contact with COVID-19 among HCP at a health care system in Pakistan.
Methods
Shaukat Khanum Memorial Trust is a health care system in Pakistan, comprising two cancer hospitals. The institution adopted the World Health Organization guidelines for personal protective equipment, including universal masking, and limited the use of N-95 respirators to aerosol-generating procedures such as intubation and bronchoscopy during the COVID-19 pandemic. 5 Employees self-reporting fever, cough, shortness of breath, sore throat, chills, or anosmia, or those with household contacts with COVID-19 underwent nasopharyngeal polymerase chain reaction (PCR) testing. Infected HCP were excluded from work.
The Trust offered SARS-CoV-2 total antibody testing free of cost to employees (n = 3271) between July 29, 2020, and July 31, 2020. The test utilized an electro-chemiluminescence immunoassay to measure SARS-CoV-2 total antibodies, including immunoglobulin (Ig) G, IgM, and IgA (Roche Diagnostics International Ltd). We collected data on the following variables for employees who underwent antibody testing: age, sex, designation, and the results of prior COVID-19 PCR testing, if applicable. We telephonically contacted HCP with positive antibodies to administer a survey in September 2020, exploring a history of contact with a patient, family member, or coworker with known COVID-19, a history of symptoms compatible with COVID-19, and details of nasopharyngeal PCR testing for COVID-19 between March 1, 2020, and July 31, 2020. We obtained verbal consent for participation in the survey. We defined “clinical staff” as HCP with direct contact with patients, their body tissues, or biologic waste. We reported the mean and standard deviation for continuous variables, and frequencies and proportions for categorical variables. We calculated the unadjusted odds ratio (OR) and 95% confidence intervals (CI) for SARS-CoV-2 seropositivity by age, sex, and job description. We performed multivariate logistic regression to determine the OR and 95% CI of a positive serum antibody test for sex and job description when adjusted for age. Statistical analysis was performed using SPSS version 20. This study was approved by the institutional review board (IRB) at Shaukat Khanum Memorial Cancer Hospital and Research Center, Lahore (Study ID: IRB-20-28).
Results
A total of 2162 (66.1%) HCP underwent antibody testing. This included 631 (29.2%) females and 1142 (52.8%) clinical staff members, with a mean age of 34 ± 8.9 years (Table 1). Of the 857 (39.6%) employees who tested positive, 820 (95.7%) consented to participate in the survey (Table 2). Six hundred fifteen (75%) HCP reported a history of contact with an individual with COVID-19. Among the 529 HCP reporting a history of symptoms compatible with COVID-19, only 451 underwent PCR testing while symptomatic (Table 2). When adjusted for age, males had higher odds of testing positive for SARS-CoV-2 antibodies compared with females (OR = 1.68; 95% CI [1.37, 2.05]; P = .00) and clinical staff had higher odds of SARS-CoV-2 seropositivity compared with nonclinical staff (OR = 1.273; 95% CI [1.06, 1.53]; P = .01; Table 1). When adjusted for sex and designation, younger HCP did not have higher odds of testing positive for SARS-CoV-2 antibodies compared with older HCP (OR = 1.00; 95% CI [0.99, 1.01]; P = .60).
Characteristics of Employees Tested for SARS-CoV-2 Antibodies.
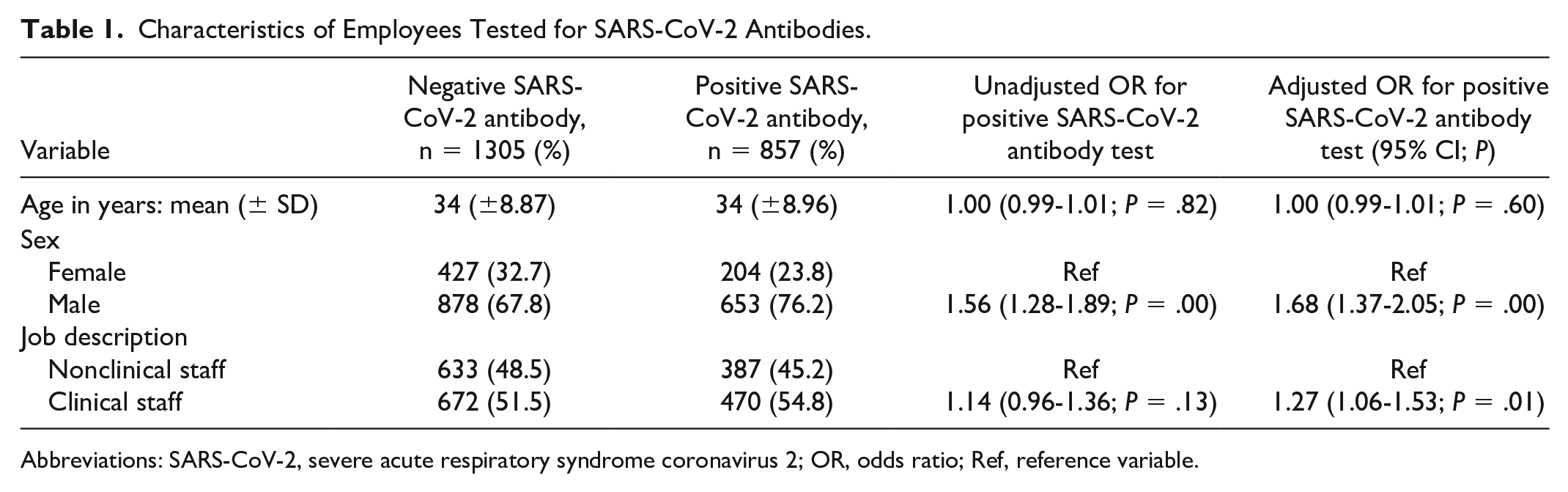
Abbreviations: SARS-CoV-2, severe acute respiratory syndrome coronavirus 2; OR, odds ratio; Ref, reference variable.
Characteristics of Survey Respondents.

Abbreviations: PCR, polymerase chain reaction; COVID-19, coronavirus disease-2019.
Discussion
We report a high seroprevalence of SARS-CoV-2 total antibodies (39.6%) among a large cohort of HCP (N = 2162) across a health care system. Our seropositivity rate is similar to a study evaluating samples from healthy blood donors in Pakistan in July 2020. 6 The lower seroprevalence of SARS-CoV-2 described in other geographical locations may represent a chronological artefact as testing performed earlier during the pandemic is likely to have yielded lower seropositivity rates. 7 Alternatively, this may be attributed to varied testing methods.3,7
Our results revealed higher odds of seropositivity among males compared with females. This has not been consistently reported in previous studies and should be explored further in our population.7,8 Prior studies present conflicting evidence on the risk of COVID-19 acquisition among HCP with direct contact with COVID-19 patients.1,3,9 In our study, we observed an association between SARS-CoV-2 serpositivity and patient contact.
Among our survey respondents, 83 (10.1%) did not seek testing despite symptoms suggestive of COVID-19. Barring units with a high incidence of COVID-19, our institutional strategy to test HCP heavily relied on self-reporting of symptoms compatible with the infection. Given the high infectivity of SARS-CoV-2, mandatory screening of symptoms for all employees at designated stations or through internet-based applications may be considered to improve reporting. A total of 272 (33.1%) survey participants denied a history of COVID-19 symptoms. This may represent the burden of asymptomatic infections within our HCP population. Asymptomatic infections play a crucial role in propagating the chain of COVID-19. 10 This highlights the importance of hospital-wide implementation of measures such as universal masking and physical distancing.
Our study is limited by its cross-sectional design, potentially introducing recall, and reporting bias into our results. Our projected rates of asymptomatic infections are not based on PCR testing, and must, therefore, be interpreted with caution.
In conclusion, the high rates of seroprevalence (39.6%) among HCP in our study mirrored those in the community. Males had higher odds than females and clinical staff had higher odds than nonclinical staff to test positive for SARS-CoV-2 antibodies. A high proportion of HCP likely had asymptomatic infections. Implementation of effective infection control measures and personal protective equipment guidelines is essential to protect HCP from COVID-19, minimizing the risk of contracting the infection from COVID-19 patients. Mandatory screening for symptoms and point-prevalence surveys may be considered to estimate the true burden of COVID-19 among HCP.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.