
Abstract
The COVID-19 outbreak was declared a pandemic by the World Health Organization in March 2020 due to rapid intercontinental spread and high morbidity and mortality. Globally, the disease has had a major impact on human lives, including health, economic, employment, psychological, and overall well-being. The COVID-19, besides causing respiratory, neurological, and cardiovascular diseases, has had significant impact on mental health. Major mental health disorders, including depression, anxiety, and stress, have risen in parallel with increasing prevalence of COVID-19. Many population groups, including children, the elderly, those with chronic illnesses, and health care workers, have been affected. This review gives an overall assessment of the prevalence of COVID-19-associated psychological morbidity. In countries in the Asia-Pacific region, prevalence of depression ranged between 4.9% and 43.1%, anxiety from 7.0% to 43.0%, and stress from 3.4% to 35.7%. As COVID-19 continues to severely affect the psychosocial well-being of the population at large, countries have developed and revised policies, guidelines, and introduced new initiatives to curb mental health issues among their citizens. In the long run, pre-disaster preparedness is important to alleviate long-term post-pandemic psychiatric morbidity and to develop psychological resilience toward disasters and pandemic, alongside investment for better mental health coverage.
What We Already Know
The COVID-19 pandemic has negatively affected the health and well-being of the population in terms of both physical and mental health.
The implication of COVID-19 on mental health can be attributed to disruptions in daily living activities, fear of infections, and adverse economic impacts.
Behavioral and emotional issues such as substance abuse, domestic violence, and suicide has risen in the population.
What This Article Adds
Insight into the extent of 3 major mental health issues, namely, depression, anxiety, and stress, reported from the Asia-Pacific region.
Summary of the policies, programs, and guidelines developed to address the mental health burden during the pandemic.
Preventive measures such as pre-disaster preparedness and investment in health care are recommended to reduce the burden of disease in the future.
Introduction
On December 31, 2019, a cluster of atypical pneumonia cases was reported in Wuhan city, Hubei province in China. Later, it was ascertained that the disease was caused by a virus, the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), a novel strain of coronaviruses, whose genetic composition is 79% similar to the 2003 SARS-CoV. 1 The disease was later officially declared as the coronavirus disease 2019 (COVID-19). On January 30, 2020, the Director General of the World Health Organization (WHO) declared COVID-19 as a Public Health Emergency of International Concern (PHEIC), given that it had spread over to 20 countries within a month. 2 On March 11, 2020, the WHO declared the COVID-19 outbreak as a global pandemic, due to a 13-fold increment in the number of cases outside of China, affecting 114 countries with 118 000 cases reported. 3
As of May 2021, according to the WHO Coronavirus Disease (COVID-19) Dashboard, the total number of confirmed cases globally is over 150 million with more than 3.2 million deaths. 4 According to the COVID-19 Dashboard, countries in the Asia-Pacific region are the ones worst hit by the pandemic, especially the low- and middle-income countries. 5 South Asian countries, such as India, Pakistan, and Bangladesh, top the list in the number of confirmed cases in the Asia-Pacific region, followed by Southeast Asian countries such as the Philippines and Indonesia, with relatively high number of cumulative confirmed cases and cumulative number of deaths. 5 Factors such as under preparedness, fragile health care systems, and poor living conditions have been associated with the exponential increase in the number of COVID-19 cases in these countries. For example, in India, a large number of hospitals have limited resources especially where intensive care units are concerned. 5 In addition, poor living conditions have also exacerbated the COVID-19 infections. In the city of Mumbai, India, many people have been found living in slums and informal settlements. Many lack access to clean water, have poor knowledge of personal hygiene and of social distancing, all of which have contributed to the “multiplier effect,” leading to the spread of the disease at a much higher rate in the city. 5
The COVID-19 pandemic has far-ranging adverse impact on different aspects of human lives, including its impact on mental health and well-being. Mental health has always been an important, emerging, and pivotal public health issue that has affected the Asia-Pacific region due to its rapid development, contributing to increasing disability adjusted life years (DALYs), morbidity, and mortality.6,7 Some preliminary COVID-19 studies have shown an increase in symptoms of depression, anxiety, and stress in the population, stemming from stressful issues such as fear of infection, disruptions in daily activities, or fear of adverse economic impact. 8 For example, quarantine is associated with increased likelihood of mental health issues such as anger and stress. 9 In addition, a rise in risky or unhealthy behaviors such as substance abuse (i.e. increased alcohol consumption), increased online gambling, inability to cope with restriction in religious activity, and suicidal ideation have also been reported. 10 Furthermore, it has been reported that the SARS-CoV-2 might infect brain and trigger immune response that alter brain functions and mental health among patients with COVID-19. 11 Besides these, certain reports and data suggest that South Asian countries are underprepared for the increasing mental health burden due to COVID-19, given their limited mental health facilities and resources. 12
Given the rising number of cases, coupled with genetic mutations that increase the infectivity of the virus, it is expected that COVID-19 will have a prolonged mental health impact on the population, especially in the Asia-Pacific region. To curb this issue, numerous research bodies, governmental organizations as well as nongovernmental organizations (NGOs) have initiated various mental health researches. The findings from these researches have aided governmental organizations and national health departments to develop and implement policies and plans for mental health tailored specially for the pandemic.
The objective of this article is to discuss the major mental health issues that have impacted the Asia-Pacific region during the COVID-19 pandemic as well as the policies and plans developed to address these issues.
Method
Mental health issues in the Asia-Pacific region are multifaceted and complex. In this review, we focus on three major mental health issues: depression, anxiety, and stress. As the COVID-19 pandemic is a recent event, only research published in 2020 and 2021 has been reviewed. A literature search was undertaken using the PubMed, Web of Science, and Google Scholar databases using different permutations and combinations of the key words: “COVID-19,” “coronavirus disease,” “SARS-CoV-2,” and “psychology” or “depression” or “anxiety” or “stress” or “mental health” or “mental disorder” and “Asia” or “Pacific” or “China” or “Korea” or “Japan” or “Taiwan” or “Laos” or “Cambodia” or “Vietnam” or “Philippines” or “Malaysia” or “Singapore” or “Myanmar” or “Indonesia” or “Papua New Guinea” or “India” or “Bangladesh” or “Pakistan” or “Maldives” or “Nepal” or “Iran” and “policy” or “guideline” or “initiatives” or “manual” or “program.” Only English language articles published in 2020 or 2021 were reviewed. Further references were obtained from reports published by international organizations, especially the WHO and national government agencies such as national departments of health. Literatures, reports, and articles that were relevant are cited in this article.
Results
Three Main Mental Health Issues of the COVID-19 Pandemic
A mosaic of mental health and emotional issues have been reported as pivotal public health concerns in the Asia-Pacific region, due to the COVID-19 pandemic. Fear of infection, fear of death, social distancing, quarantine, misinformation (particularly the ones being spread through social media), as well as social and economic debacles have caused a mosaic of psychological and emotional distress. The three major mental health issues that have affected the global population during the COVID-19 pandemic are depression, anxiety, and stress, especially among young adults.8,13 Fear of infection and fear of falling ill due to COVID-19 has been lingering in the minds of people worldwide, in addition to the influx of COVID-19-related news and information garnered from both mainstream media as well as social media. 14 Recent studies have postulated that the fear of infection was highly associated with anxiety and stress and, to a lesser extent, depression. 14 However, the relationship between stress, anxiety, and depression has long been reported in scientific literature, that is, environmental stress associated with pathophysiology of depression and anxiety. 14 Besides that, depression, anxiety, and stress have also been associated with negative health behaviors such as smoking, substance abuse (ie, overconsumption of alcohol, drug abuse), physical inactivity, and suicidal ideation. 10
Depression
Several countries reported the prevalence of depression during COVID-19. In Australia, a population-based study reported prevalence of depression of 37.1%. 8 Among East Asian countries, Japan has the highest prevalence of depression (43.1%), followed by China (30.3%) and Hong Kong (19.0%).10,13 South Asian countries such as India and Nepal reported prevalence of 38.9% and 34.0%, respectively. 13 Southeast Asian countries such as Malaysia and Vietnam reported depression at the rate of 13.0% and 4.9%, respectively.15,16
Anxiety
Prevalence of anxiety has also been reported from several countries in the Asia-Pacific region. Among oriental Asian countries, China reported the highest prevalence of anxiety, which is 36.4%, followed by Japan (33.2%) and Hong Kong (14.0%).10,13 Australia reported a prevalence of 29.1%, while South Asian countries, such as India and Nepal, reported a prevalence of 43.0% and 31.0%, respectively.8,13 Meanwhile, Southeast Asian countries such as Malaysia and Vietnam reported prevalence of anxiety of 26.0% and 7.0%, respectively.15,16
Stress
The occurrence of stress was also reported to have risen alongside depression and anxiety during this pandemic. Several studies have reported the prevalence of stress in the Asia-Pacific region. Both India and China reported a high prevalence of stress, which are 35.7% and 32.1%, respectively. 13 Meanwhile, Australia reported a prevalence of 33.6%, whereas Malaysia reported 9.5%.8,15 Vietnam reported the lowest prevalence of stress in the region, which is 3.4%. 16 The detailed prevalence of depression, anxiety, and stress can be observed from Table 1.
Prevalence of Depression, Anxiety, and Stress in Selected Countries.
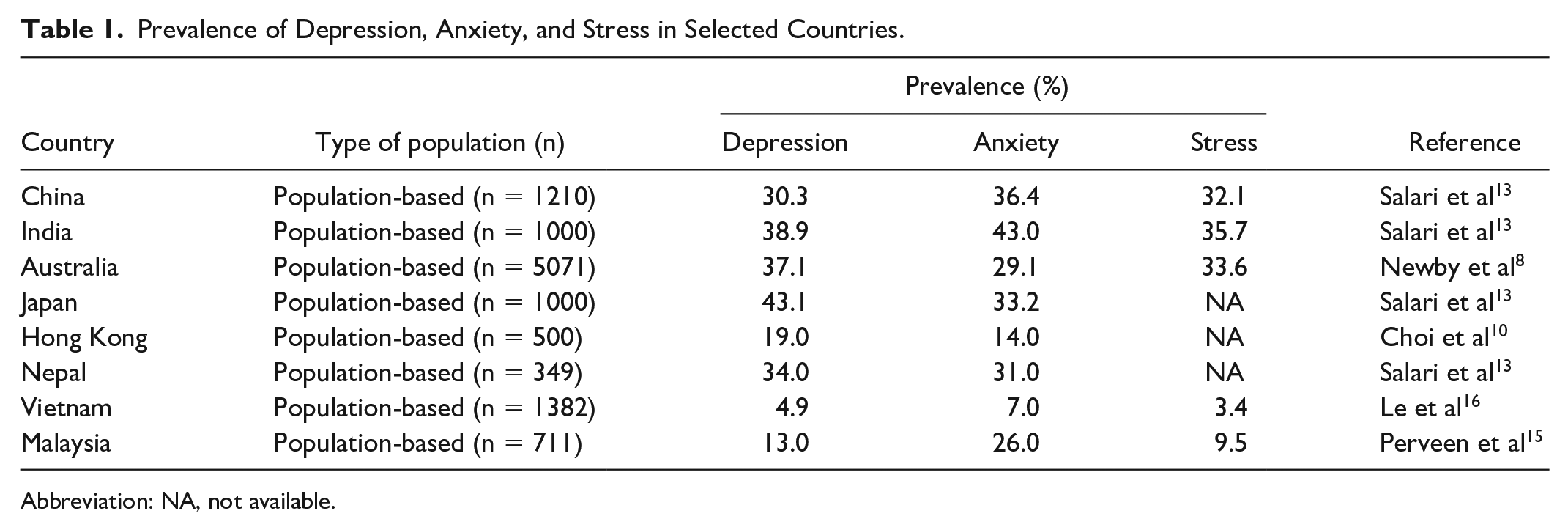
Abbreviation: NA, not available.
Policies and Programs to Combat Mental Health Issues During COVID-19 Crisis
The rapid publication of numerous research studies on the impact of COVID-19 on mental health in the Asia-Pacific region has carved a pathway for evidence-based policy decisions, preventive measures, treatment programs, and community support systems for those who are vulnerable and are at high risk of negative mental health outcome during this pandemic. Several countries in the region have come up with policies and programs that serve as a guide to various members of the community, as well as health care workers, to improve mental health in the region.
In Australia, the Department of Health has taken drastic measures to improve the mental health of its citizens. The country introduced an initiative called Better Access to Psychiatrists, Psychologists and General Practitioners through the Medicare Benefits Schedule (Better Access), with 10 individual Better Access psychological therapy sessions for those who are enduring mental health issues due to COVID-19. 17 From October 9, 2020, the government has added 10 additional subsidized psychological therapy sessions, which means each person would be eligible for 20 individual therapy sessions. In addition, the Better Access initiative that was initially only available to those residing in areas with restricted movement was made available to everyone, beginning October 9, 2020, to June 30, 2022. 17 Besides that, several mental health helplines such as Lifeline, Beyond Blue Coronavirus Mental Wellbeing Support Service, Translating and Interpreting Service (TIS National), Kids Helpline contact, and Suicide Call Back Service were also introduced to help its citizens cope with mental health issues. 17 All these helplines are available 24 hours a day, 7 days a week, whereby trained professionals will be available to receive calls and provide necessary services to those who are in need.
Meanwhile, in China, a national guideline on mental health intervention was published by China’s Joint Prevention and Control Mechanism of the State Council (China’s central authority in response to COVID-19).18,19 The guideline spelled out the roles and responsibilities of various stakeholders that are involved in the support system of the mental health intervention such as local government, mental health professionals, social work organizations, and community volunteers. The guideline identifies four different strata of people based on the level of stressors they experienced from COVID-19:
Level 1: patients with COVID-19 and frontline workers (both health care and non–health care workers),
Level 2: self-quarantined patients (both confirmed and suspected of COVID-19 infection),
Level 3: people who are related to Level 1 and Level 2 population, and
Level 4: people who are affected by the prevention and control practices in both epidemic and susceptible areas, as well as the general public.18,19
Given China’s large population and its ever-rising mental health burden due to COVID-19, collaborative intersectoral efforts by various stakeholders in combatting mental health problem is important. Besides, identification of different groups of people affected by mental health, based on their level of stressors, promotes efficacious and efficient response and treatment that could save time and resources.
India has also taken some drastic measures in addressing mental health issues during the pandemic. The Ministry of Health and Family Welfare has published a few guidelines in collaboration with the National Taskforce for the finalization, implementation, and monitoring of the psychosocial action plan for COVID-19 response. 20 Some of the notable guidelines include “Guidelines on Managing Mental Illness in Hospital Settings during COVID-19,” “Mental Health Matters . . . Let’s Talk,” “Caring for Health Care Warriors—Mental Health Support During COVID-19,” “Mental Health in the times of COVID-19 Pandemic—Guidance for General Medical and Specialised Mental Health Care Settings,” and a couple of other guidelines to address stigma, discrimination, as well as tobacco and alcohol-related issues during lockdowns. 21 In addition, the Ministry of Social Justice and Empowerment has established national psychosocial behavioral helpline to assist those in need. 20
In Malaysia, the Ministry of Health Malaysia has published a guideline titled “COVID-19 Mental Health Kit—In Hospital Setting and Quarantine Centre.” The guideline was developed for both patients and health care workers. The main objective of this guideline is to ameliorate anxiety and fear among four different types of patients, namely (1) patient who comes for COVID-19 screening, (2) patient who undergoes home quarantine, (3) person with acute respiratory infection and has epidemiological link with COVID-19 cases/clusters, and (4) COVID-19 patients. 22 This guideline also contains basic mental health screening for COVID-19 Person Under Investigation (PUI) and COVID-19 patients. This tool is to be utilized by the person in charge at each COVID-19 facility. Patients who score more than 3 will be referred to the Mental Health and Psychosocial Support Service (MHPSS) team of the respective hospital. 22 As for health care workers, this tool can be used during pre- and post-deployment briefing to boost their morale and motivation during this challenging time. Besides that, the Copenhagen Burnout Inventory is also to be incorporated to assess burnout among health care workers. Those found to be positive for burnout will be referred to psychiatrists, psychologists, or counselors. 22
Singapore too has responded to the pandemic, and came up with a guideline called the “Psychological Preparedness Toolkit for Healthcare Workers.” 23 The aim of the toolkit was to provide an overview of the tasks at frontline, which could be unfamiliar to health care workers from different levels of experience and care settings. The toolkit is categorized into 4 main sections: (1) expected emotional response, (2) changes in the work environment, (3) support measures, and (4) anticipated effects on mental health. 23 Uniquely, the toolkit provides pragmatic coping strategy against various mental health issues as well as advices that have been developed based on evidence and experience from previous health care workers who served in areas affected by COVID-19. 23 Besides that, Singapore’s health care workforce comprises a significant portion of the 300 000 Malaysians who cross the Malaysia-Singapore border on a daily basis. Since the annunciation of Malaysia-Singapore border lockdown, some of these workers have been stranded in a foreign country, facing dilemma such as alternative work and accommodation. Singapore addresses this problem and provides advice on utilization of social media and telecommunication to engage with their families in Malaysia. 23 Additionally, a psychometric assessment was incorporated to assess burnout among health care workers, called the Burnout Measure (short version). Its easy administration motivates for a routine mental health assessment. Moreover, the toolkit provides guidance for the supervisors in charge of particular health care settings, which facilitates in evaluating and identifying burnout and disengagement among health care workers. 23 Thus, the toolkit promotes timely actions and interventions to be taken for those who are at risk of mental health issues.
Given this acute period of COVID-19, as well as the co-occurrence of climate change and natural disasters, a network was formed in the Asia-Pacific region called the Asia Pacific Disaster Mental Health Network, which is supported by the WHO Thematic Platform for Health Emergency and Disaster Risk Management (Health EDRM).24-26 The network is open to all countries in the Asia-Pacific region, but currently, it is represented by representatives from Australia, Japan, China, Nepal, Sri Lanka, India, and the United States of America. The network, comprising experts who had worked with trauma-affected communities, as well as expertise in responding to health emergencies and natural disasters, formed this collaborative platform for policy and research development, in line with WHO Health EDRM’s priorities and its research network.24-26 The outcome of the network was the development of a regional disaster mental health agenda focused on current issues. The five priority areas that were focused on are the following: (1) strengthening community engagement and the integration of diverse perspectives in planning, implementing, and evaluating mental health and psychosocial response in disasters; (2) supporting and assessing the capacity of mental health systems to respond to disasters; (3) optimizing emerging technologies in mental health care; (4) understanding and responding appropriately to addressing the mental health impacts of climate change; and (5) prioritizing mental health and psychosocial support for high-risk groups. 24 With the rampant spread of COVID-19, it is expected that improved capacity for community and mental health services and strengthened community engagement could be forged to address the needs for improved mental health care delivery and policy during this pandemic (Table 2).
Policies and Plans to Address Mental Health Issues.
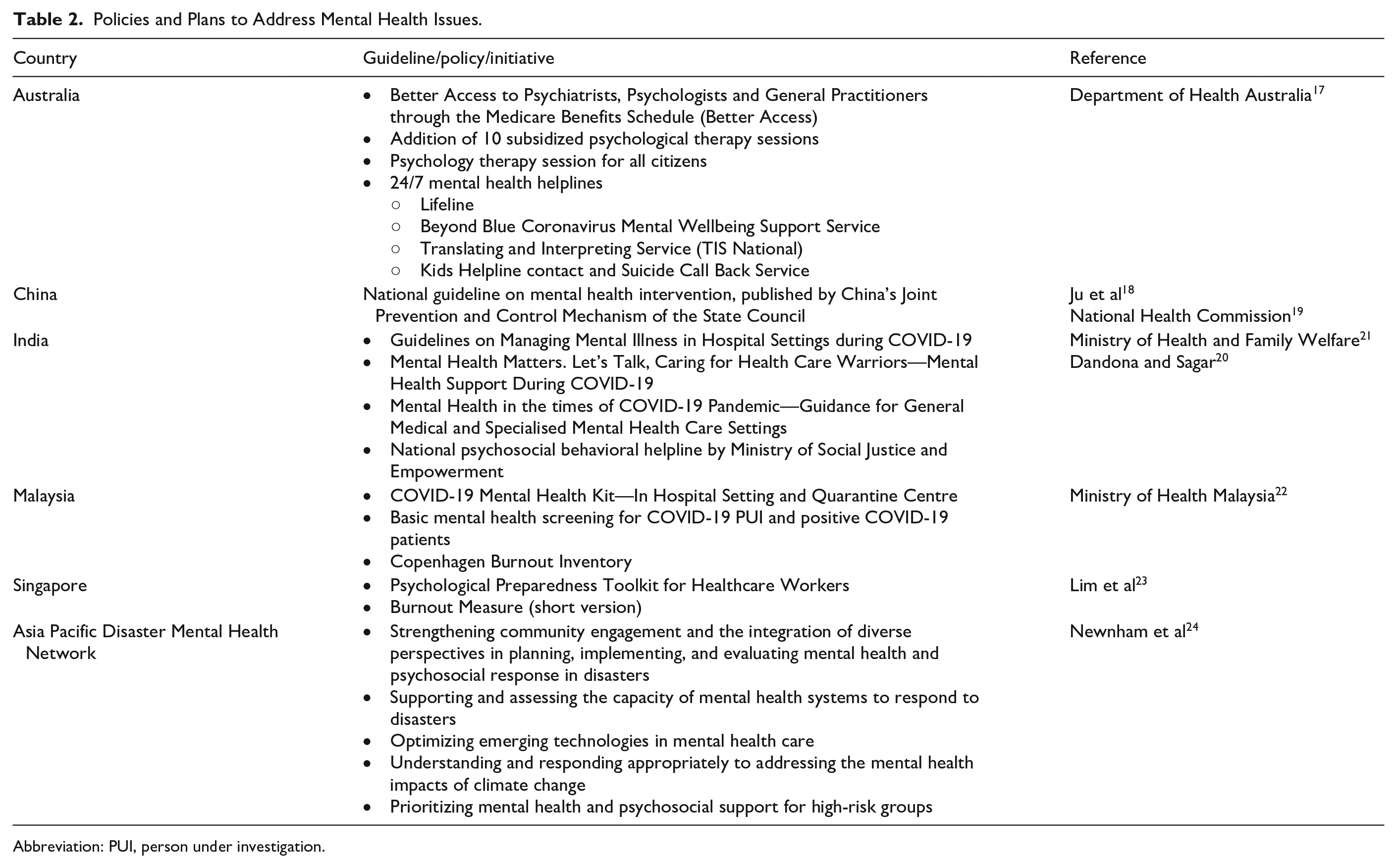
Abbreviation: PUI, person under investigation.
Discussion
The COVID-19 pandemic has caused significant mortality and morbidity worldwide. Besides adverse effect on physical health, it has also brought about deleterious impact on the quality of life and general well-being of the population. Previous studies and reports with regard to disasters or public health emergencies reveal that on the occurrence of a disaster, it will cause adverse effects on the mental health and well-being of the population. In addition, it can also cause long-term psychiatric morbidity. A study in India revealed that even 4.5 years after the tsunami in 2004, the prevalence of mental health issues was still high; anxiety (23.1%), depression (33.6%), and posttraumatic stress disorder (PTSD) at 70.9%. 27 In 2011, an earthquake in Japan, which caused a nuclear accident at the Fukushima Daiichi Nuclear Power Plant, led to massive evacuation within the 20 km radius, involving more than 121 000 residents. 28 The disaster, also called the Fukushima Daiichi accident and the Great East Japan Earthquake (GEJE), has caused significant psychological distress, depression, anxiety as well as symptoms of PTSD. 28 Evidently, these phenomena are not unique, as witnessed in the case of the COVID-19 pandemic, whereby the disaster has caused major mental health issues, namely, depression, anxiety, and stress.
A few months before the declaration of the COVID-19 as a worldwide pandemic, the World Health Organization had announced the five major mental disorders that contributed to the global burden of disease, namely, depression, schizophrenia, and other psychoses, dementia, bipolar disorder, and developmental disorders including autism. 29 In addition, countries in the Asia-Pacific region, including high-income countries, and in the Australasian region reported unstable and worsening conditions of these mental disorders, especially among males. 7 Therefore, with the exponential increasing cases and burden of disease from the COVID-19 pandemic, it is expected that the situation will worsen and amplify the global burden of disease of mental disorders, particularly in the Asia-Pacific region.
Low- and middle-income countries in the Asia-Pacific region have been hit hard by the COVID-19 burden of disease due to the resource-limited, underprepared, and fragile health care systems, as these countries were too focused on other health issues such as noncommunicable diseases and ageing, disregarding infectious diseases. 30 The COVID-19 pandemic is a tragic wake-up call for the improvement of health care systems in the Asia-Pacific region. It has brought about a paradigm shift in the mental health care and service delivery systems across countries, despite the heterogeneity in their social, political, and economic constructs. This can be observed by the various mental health policies, guidelines, and strategies that have been subsequently developed, as outlined earlier.17-23 Government officials and ministries have come up with various new and pragmatic guidelines and policies to address the mental health issues. Besides that, a concerted effort between government and NGOs was observed in certain countries to address the overwhelming burden of mental health issues, which has been compounded by the lack of manpower. In low- and middle-income countries, the NGOs and community health workers have been mobilized in facilitating the government and national health department to disseminate information, guidelines, and policies in hard-to-reach areas such as the urban informal settlements or slums.31,32 These organizations help in educating, communicating, and translating public health messages and information, that is, social distancing, personal hygiene, and isolation/quarantine procedures to these people.31,32 This shows the need for and the importance of collaborative effort among various groups of people in combatting mental health problems. The effort has to be augmented with a well-coordinated mental health taskforce, consisting of psychiatrists, psychologists, government agencies, NGOs, and philanthropists. This will help alleviate mental health issues in South Asian countries, as well as for the whole Asia-Pacific region. 12
As the aftermath of the pandemic would be long term, many countries are taking preventive steps for future public health emergencies, disasters, and pandemics. Pre-disaster social support helps alleviate post-disaster mental health problems and foster a better psychological resilience in the population. 33 A study by Sasaki and colleagues on the survivors of the Great East Japan earthquake and tsunami revealed that participants who received pre-disaster preparedness, such as instrumental and emotional support, were less likely to develop depressive symptoms compared with those who did not receive any form of pre-disaster preparedness. 33 Besides that, many countries in the Asia-Pacific region are investing in health by implementing universal health coverage. 34 As the COVID-19 pandemic has highlighted gaps and financial challenges in different health care systems from high- and low-income countries, immediate actions such as evidence gap mapping and consultation with stakeholders have been done to implement universal health coverage in the region.34,35 With this, a better mental health delivery system can be expected, especially during pandemics or disasters.
It has to be noted that this review has a number of limitations. First, the mental health issues associated with COVID-19 that have been published recently are based on cross-sectional study. Therefore, well-established population-based longitudinal studies are needed to establish the causal relationship between the COVID-19 pandemic and mental health impact. Second, the effectiveness of the policies, guidelines, and programs regarding mental health issues have not been available as yet. Therefore, future studies on the efficacy of the initiatives are warranted to improve the policies, guidelines, and programs to cater for the ever-changing mental health needs of the population.
Conclusion
The COVID-19 pandemic has caused adverse impact on the mental health of the global population, including those in the Asia Pacific region. Mental health issues such as depression, anxiety, and stress have become prevalent during this pandemic, and the impact is expected to be long-term post-pandemic. Government officials and national health departments in the Asia-Pacific region have established mental health policies, guidelines, and strategies that facilitate the mitigation of mental health issues. In the future, a better crisis and disaster preparedness and support program should be advocated and implemented as it is proven to cultivate psychosocial resilience toward disasters and public health emergencies, reducing mental health issues even after a disaster. Besides that, the health care systems in the region should also invest in universal health coverage, so that better health care can be served to everyone, regardless of their socioeconomic background.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.