
Abstract
Native Hawaiian and Pacific Islander (NHPI) adults bear a disproportionate burden of certain human papillomavirus (HPV)-associated cancers. In 2015, data from the National Health Interview Survey (NHIS) showed vaccination coverage among adults by racial and ethnic groups; however, coverage data for NHPI adults were unavailable. In this study, we estimated the initiation and completion of HPV vaccination and assessed the factors associated with vaccination among NHPI adults aged 18 to 26 years in the United States. We analyzed public data files from the 2014 NHPI NHIS (n = 1204). We specified sampling design parameters and fitted weighted logistic regression models to calculate the odds of HPV vaccine initiation. We developed a directed acyclic graph to identify a minimally sufficient set for adjustment and adjusted for insurance coverage (for education and ethnicity) and doctor visit (for insurance coverage, earnings, ethnicity, and sex). Overall, 24.9% and 11.5% of NHPI adults had initiated and completed the HPV vaccination series, respectively. Weighted logistic regression models elucidated that the odds of HPV vaccine initiation were higher for females (weighted odds ratio = 5.4; 95% confidence interval = 2.8-10.4) compared with males. Low vaccination coverage found among NHPI adults provides an opportunity for targeted programs to reduce the burden of HPV-associated cancers.
What We Already Know
Vaccination against human papillomavirus (HPV) is recommended for preventing certain genital and oropharyngeal cancers.
Data on HPV vaccination coverage and factors for Native Hawaiian and Pacific Islander (NHPI) adults are limited.
What This Article Adds
We estimated HPV vaccine initiation and completion among NHPI adults aged 18 to 26 years using a national survey.
HPV vaccine initiation (24.9%) and completion (11.5%) among NHPI adults were suboptimal.
To prevent HPV-associated cancers, efforts to improve HPV vaccine uptake among NHPI adults should be prioritized and strengthened.
Introduction
Human papillomavirus (HPV) infection is causally associated with cervical cancer and is etiologically linked to vaginal, vulvar, anal, penile, and oropharyngeal cancers. Native Hawaiian and Pacific Islander (NHPI) women suffer disproportionately from cervical cancer.1,2 From 1998 to 2002, age-adjusted incidence rates for cervical cancer were higher among Samoan (18.1 per 100 000 females) and Native Hawaiian women (12.3 per 100 000 females) than among non-Hispanic White women (8.1 per 100 000 females). 1 From 2013 to 2015, a considerably higher death rate for cervical cancer was observed among NHPI women in comparison with Asian women (9.0 vs 1.2 per 100 000 females). 2 For oropharyngeal cancer, mortality rates from 2013 to 2015 were highest in the NHPI population (8.3 per 100 000) compared with White (3.4 per 100 000) and Asian (2.3 per 100 000) populations. 3 Similarly, data from the Hawai’i Tumor Registry showed that Native Hawaiian men had a greater mortality rate per 100 000 than White men (5.1 vs. 3.9). 4 For other HPV-associated cancers, data for NHPI adults are often aggregated with Asian American adults concealing the diversity of these heterogeneous populations. 5
To prevent most HPV-associated cancers, vaccines have been available since 2006 in the United States (US). The HPV vaccine was first licensed for use in females during June 2006 and was recommended for routine vaccination of females aged 11 or 12 years and for those aged 13 through 26 years not previously vaccinated. 6 For males, the HPV vaccine was first licensed for use in 2009 and was recommended for routine vaccination of males aged 11 or 12 years and for those aged 13 through 21 years not previously vaccinated.7,8 In 2019, catch-up vaccination was recommended for all persons through age 26 years. 9 For adults aged 27 through 45 years, shared clinical decision-making is recommended for receiving the HPV vaccine. 9 In 2015, data from the National Health Interview Survey (NHIS) showed that the HPV vaccination coverage for female and male adults aged 19 to 26 years in the US was 41.6% and 10.1%, respectively. 10 HPV vaccination coverage was highest among White women (44.7%), followed by Black (38.0%), Asian (36.3%), and Hispanic (35.7%) women; however, coverage data for NHPI adults was unavailable in this study. 10
Previous studies focused on the NHPI population have estimated HPV vaccine uptake and factors among adolescents 11 and college students 12 but not adults. To address this research gap, we analyzed the 2014 NHPI NHIS, which is the latest national, publicly available data for this population. In this study, we aimed to (1) estimate HPV vaccine initiation and completion and (2) assess factors associated with HPV vaccine initiation among NHPI adults as this information is often needed to guide immunization policies and interventions, monitor progress, and improve vaccination rates.
Methods
Data
We analyzed public data files from the 2014 NHPI NHIS, the first and latest federal survey designed exclusively to measure the health of the civilian noninstitutionalized NHPI population of the US. Data were collected from February to November 2014 through face-to-face interviews with eligible NHPI participants in all 50 states and the District of Columbia. Information on the sample design, frame, and weights are provided in the survey description document. 13 As HPV vaccination data were only available for adults in NHPI NHIS, we restricted our analyses to adults aged 18 to 26 years (n = 1204). As the HPV vaccine became available for men in 2009 and recommended up to age 21 years, males only up to age 26 years in this data set would have had the opportunity to be vaccinated. Therefore, the upper age limit of 26 years was selected to include both males and females who would have been eligible to receive the HPV vaccine.
Measures
Our primary outcome of interest, HPV vaccine initiation, was defined as the reported receipt of at least 1 dose of the vaccine and was assessed through the survey question: “Have you ever received an HPV shot or vaccine?” 14 HPV vaccine completion was defined as the reported receipt of 3 doses of the vaccine and was assessed through the question: “How many HPV shots did you receive?” 9
Statistical Analysis
We fitted weighted logistic regression models to estimate the odds of HPV vaccine initiation by demographic (sex, ethnicity, and education) and health care (insurance coverage and “seen or talked to a doctor in the past 12 months”) factors. To assess confounding, we evaluated the relationship between the variables and outcome of interest and developed a causal diagram (directed acyclic graph or DAG; see Supplementary Material, available online) to identify a minimally sufficient set for adjustment. Based on the DAG, no adjustment was needed for sex, ethnicity, and education; thus, only unadjusted estimates are presented for these variables. On the other hand, we adjusted insurance coverage (for education and ethnicity) and doctor visit (for insurance coverage, earnings, ethnicity, and sex). For the weighted regression models, we report the size of the effect through unadjusted (for sex, ethnicity, and education variables) and adjusted (for insurance coverage and general doctor visit variables) weighted odds ratios and precision through 95% confidence intervals (CIs) around the estimates. We did not impute any missing values for our primary outcome variable but treated missing values as missing at random for Taylor series variance estimation. Sampling design parameters, such as stratification, clustering, and weighting, were specified using the proc survey logistic procedure in SAS (version 9.4; SAS Institute). All analyses were conducted from April to November 2020.
Ethics
As we used publicly available data, this study did not meet the criteria for human subjects research.
Results
As of 2014, 24.9% of NHPI adults aged 18 to 26 years had initiated the HPV vaccination series (Table 1). Furthermore, 11.5% of NHPI adults had completed the HPV vaccination series. By sex, 20% of adult NHPI females and 4.9% of adult NHPI males had initiated the vaccination series. Similarly, 9.4% and 2.1% of adult NHPI females and males reported completing the vaccine series, respectively. HPV vaccine initiation was higher among adults who were non-Hispanic or Latino (22.3%), had insurance coverage (19.7%), were never married (17.7%), earned less than $25 000 in the past year (15.8%), had seen a general doctor in the past year (14.3%), and had some college credits or an associate degree (13.1%).
Participant Characteristics, Overall and by Human Papillomavirus (HPV) Vaccine Initiation, Among Native Hawaiian and Pacific Islander (NHPI) Adults Aged 18 to 26 Years, NHPI National Health Interview Survey (NHIS), United States, 2014 13 .
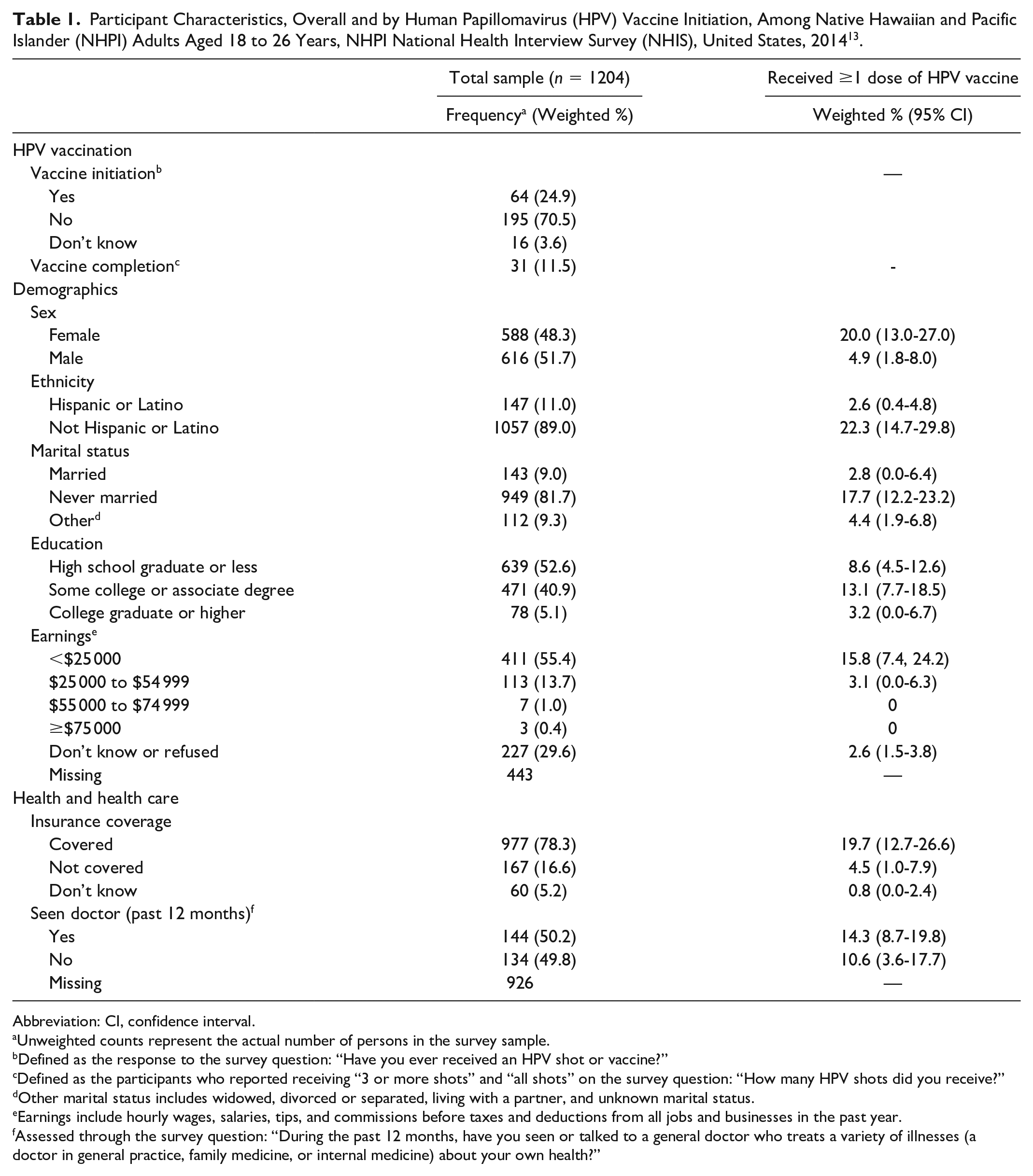
Abbreviation: CI, confidence interval.
Unweighted counts represent the actual number of persons in the survey sample.
Defined as the response to the survey question: “Have you ever received an HPV shot or vaccine?”
Defined as the participants who reported receiving “3 or more shots” and “all shots” on the survey question: “How many HPV shots did you receive?”
Other marital status includes widowed, divorced or separated, living with a partner, and unknown marital status.
Earnings include hourly wages, salaries, tips, and commissions before taxes and deductions from all jobs and businesses in the past year.
Assessed through the survey question: “During the past 12 months, have you seen or talked to a general doctor who treats a variety of illnesses (a doctor in general practice, family medicine, or internal medicine) about your own health?”
Unadjusted and adjusted weighted odds ratios for HPV vaccine initiation factors are presented in Table 2. The odds of HPV vaccine initiation are 5.4 (95% CI [2.8,10.4]) times higher for females compared with males. Other variables, including education, ethnicity, insurance coverage, and doctor visit, were not associated with HPV vaccine initiation.
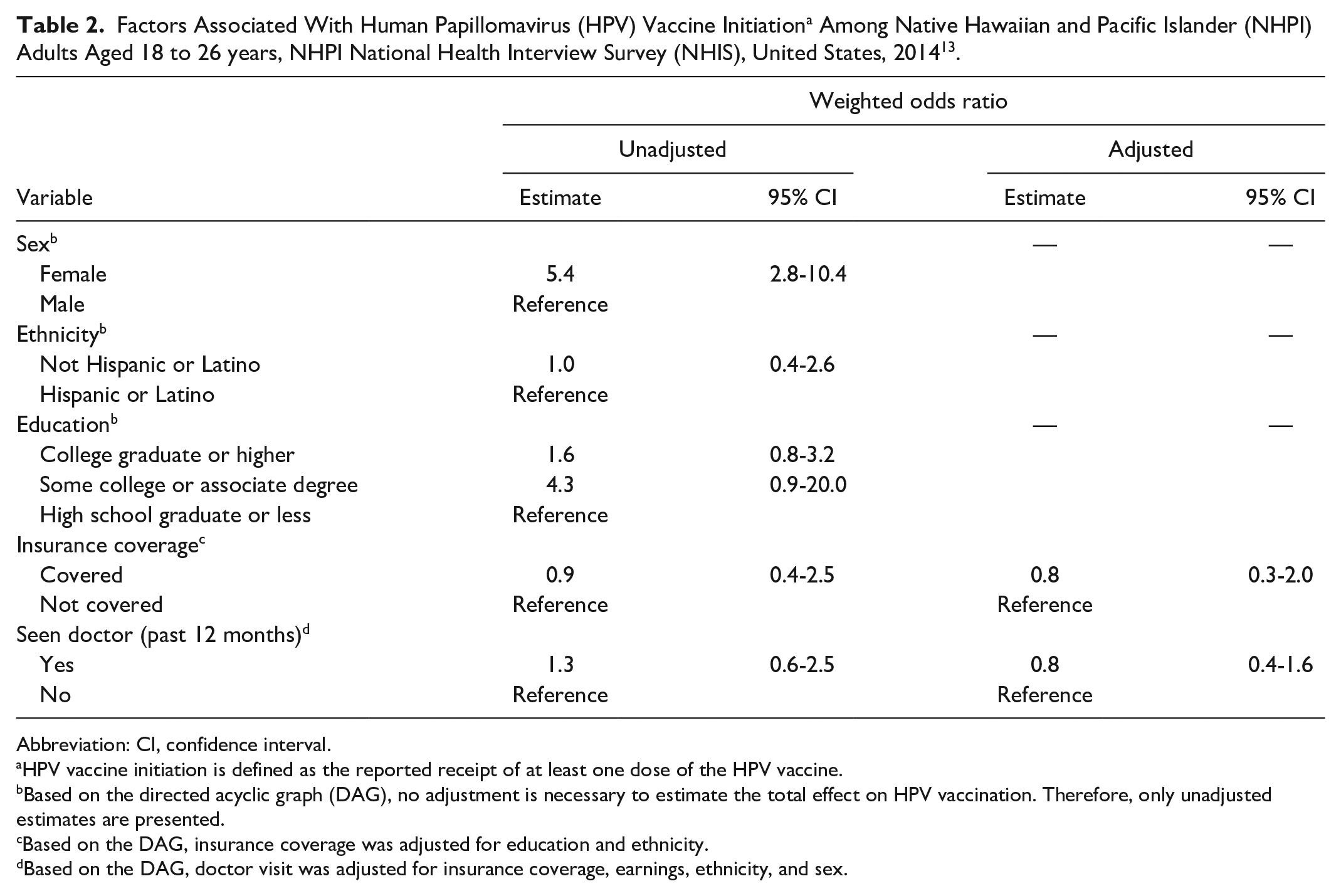
Abbreviation: CI, confidence interval.
HPV vaccine initiation is defined as the reported receipt of at least one dose of the HPV vaccine.
Based on the directed acyclic graph (DAG), no adjustment is necessary to estimate the total effect on HPV vaccination. Therefore, only unadjusted estimates are presented.
Based on the DAG, insurance coverage was adjusted for education and ethnicity.
Based on the DAG, doctor visit was adjusted for insurance coverage, earnings, ethnicity, and sex.
Discussion
The HPV vaccine has been available since 2006 and 2009 for female and male adults, respectively. However, our results indicate that HPV vaccine initiation and completion were suboptimal among NHPI adults surveyed in 2014. In our study, HPV vaccine initiation among adult NHPI females (20%) and males (4.9%) was much lower than that reported among adult US females (40.2%) and males (8.2%) in the 2014 NHIS. In the same survey, adult White (46.3%), Black (37.4%), Hispanic or Latino (28.1%), and Asian (22.8%) women reported a higher HPV vaccine initiation than adult NHPI women aged 18 to 26 years in our study. 15 Despite the low HPV vaccination coverage observed in 2014, we would expect coverage estimates to increase as more adolescents receive the HPV vaccine at the target age group and move into adulthood. For example, data from the National Immunization Survey–Teen (NIS-Teen) has shown a gradual increase in coverage for at least 1 dose of the HPV vaccine each year among adolescents aged 13 to 17 years: 2015 (56.1%), 16 2016 (60.4%), 17 2017 (65.5%), 18 2018 (68.1%), 19 and 2019 (71.5%). 20 The trend of increasing vaccination coverage annually was observed in both male and female adolescents. Although NIS-Teen reports HPV vaccination coverage by state, race, and ethnicity, data are not shown for NHPI adolescents.
Consistent with previous reports,15,21 we found a higher initiation of HPV vaccination among female adults in this study. In a population-based study among major ethnic groups in Hawaii, a higher uptake of the HPV vaccine was also reported in Native Hawaiian female adolescents aged 11 to 18 years than their male counterparts (58.6% vs. 41%). 22 Although we did not assess the reasons for low initiation in the present study, prior research in this population has identified some barriers and facilitators for HPV vaccination.22-24 For instance, studies have shown that lack of awareness 25 and knowledge 22 about the HPV vaccine among NHPI parents is a significant barrier, often impeding vaccine uptake. Furthermore, in an online survey of health care providers in Hawaii, 83% cited that lack of parent knowledge and understanding of HPV infection was a barrier to HPV vaccination. 26 Educational interventions culturally tailored toward the community may be needed to enhance knowledge about the virus and vaccine. For example, in the development of an educational brochure for the HPV vaccine, parents from Hawaii stated that the material should reflect the local population and include local faces and voices in the testimonials. 27 On the other hand, one of the most common reasons for vaccination in the NHPI population was physician recommendation.22,23 However, a survey conducted in 2012 found that only 71% of providers in Hawaii strongly recommended the HPV vaccine to adolescent girls, and only 57% strongly recommend the vaccine to adolescent boys. 28 Therefore, interventions to encourage physicians to recommend the HPV vaccine according to the current guidelines are needed.
Limitations
Our study has several limitations that merit consideration. First, in the absence of provider validation, our reported HPV vaccination initiation and completion might be over- or under-reported. Second, some differences in the initiation and completion of HPV vaccination observed by sex may be due to differences in vaccine licensure and recommendations. For instance, fewer physicians in Hawaii were strongly recommending the HPV vaccine to adolescent males than females. 28 Third, vaccination initiation estimates stratified by some demographic and health care characteristics may be unreliable due to small sample sizes. In addition, some survey responses used in our analyses may potentially suffer from recall bias and social desirability bias. Finally, although it is possible to estimate the HPV vaccination initiation and completion by detailed NHPI race groups (such as Samoan, Chamorro) through the restricted NHPI NHIS data files, our analyses were undertaken using the public use data files, which do not provide specific NHPI racial identity.
Conclusions
The low HPV vaccination initiation and completion found in this study signal the need for more evidence-based, culturally relevant immunization and cancer prevention interventions for NHPIs. Improving HPV vaccination rates is an essential step toward cancer prevention efforts, and failure to do so may increase the burden of preventable cancers among NHPIs and broaden disparities. Finally, there should be a collective and renewed focus on generating high-quality and timely data (such as this survey) and research to empower NHPI communities on their health.
Footnotes
Acknowledgements
The authors appreciate the assistance of Kathy Kyler (Staff Editor, Office of the Vice President for Research, University of Oklahoma Health Sciences Center) in preparing this manuscript for publication. The authors are grateful for the feedback from the reviewers.
Author’s Note
The analyses, interpretations, and conclusions are of the authors and not of the National Center for Health Statistics, which is responsible only for the initial data.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: SVG was supported by the Hudson Fellowship in Public Health sponsored by the Hudson College of Public Health at the University of Oklahoma Health Sciences Center. AEJ and SAM were supported by the National Institute on Minority Health and Health Disparities of the National Institutes of Health under Award Number R25MD011564. JEC was supported in part by the National Cancer Institute Cancer Center Support Grant P30CA225520 awarded to the University of Oklahoma Stephenson Cancer Center for the Biostatistics and Research Design Shared Resources. SC was partially supported by the National Institute of General Medical Sciences of the National Institutes of Health Grant 5U54GM104938-07. SC was also partially supported by the Oklahoma Shared Clinical and Translational Resources (U54GM104938) with an Institutional Development Award (IDeA) from the National Institute of General Medical Sciences. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.