
Abstract
We examined whether baseline depression is associated with myocardial infarction (MI) within a 2-year period among middle-age and older adults in China and whether the association varies by sociodemographic characteristics. Two-year longitudinal data from a nationally representative sample of people aged 45+ years in China were analyzed (N = 15 226). MI within the 2-year period was coded dichotomously. Baseline depression, assessed by the 10-item Center for Epidemiological Studies Depression scale, was used as a dichotomous and a continuous variable. After adjusting for medical conditions, lifestyle, and sociodemographic characteristics, the odds of having an MI within the 2-year period were 46% greater for respondents with clinically significant depression at baseline than those without. There was a dose–response relationship between symptom severity and the probability of having an MI. The association did not vary by sociodemographic characteristics. Findings suggested that depression screening and treatment may reduce MI cases in China and beyond.
What We Already Know
Myocardial infarction (MI) cases have been rising in China.
Western studies have reported that depression increases the risk of MI in adults. Few prospective studies have investigated the link between depression and MI in Asia.
What This Article Adds
Depression is associated with an increased risk of MI within a 2-year period among Chinese adults aged 45 years and older.
The association between depression and MI does not vary by sociodemographic characteristics, suggesting that depression is a shared risk factor of MI across sociodemographic groups in China.
The tighter temporal relationship between depression and MI, the robustness of the findings, and the observation of the same relationship in China as in the West indicate that when there is depression the risk of MI is greater.
Introduction
Myocardial infarction (MI) is a leading cause of morbidity and mortality and one of the most expensive conditions during inpatient hospitalizations. Globally, about 15.9 million MIs occurred in 2015. 1 The World Bank estimated that MI cases will increase two to three times between 2010 (8.1 million) and 2030 (22.6 million) in China, due largely to changes in health behaviors. 2 The mortality rates of acute MI in China are rising at an alarming pace, particularly in rural areas.3,4 The hospitalization cost of acute MI has had an annual growth rate of 33.5% on average since 2004, straining resources across hospitals in China.3,4
Many studies have reported that depression is a risk factor for coronary heart disease (see reviews.)5-7 Studies that focus specifically on MI as the outcome are fewer. Two meta-analyses of prospective cohort studies, almost all of which were conducted in Western nations, suggest that about a 30% increased risk of MI is associated with depression.5,7 However, the extent to which the findings can be generalized to China is unclear. Some traditional Chinese practices, particularly diet that features vegetables and grains and the use of food therapy for self-care, may weaken the link between depression and MI. 8 Recent research suggests that diet and nutrition could modulate biological processes underlying depression. 9 In addition, car ownership per capita in China is much lower than in Western nations, 10 so Chinese citizens are likely to walk more in their daily life relative to their Western counterparts. Walking is good for both the body and mind. 11 However, traditional practices are changing in China. Since China’s economic reforms in the early 1980s, the Chinese have increased consumption of processed food with high-fat contents and decreased levels of physical activity. 12 In addition, depression is often unrecognized and untreated in China, meaning that adverse physiological effects of depression, if any, are likely not be ameliorated by psychological or drug interventions. 13 Moreover, it is challenging to access high-quality health care in China. 14 Many Chinese adults may not be aware of early symptoms of heart problems, which may increase their vulnerability to MI. The above considerations led us to examine the depression–MI association in China.
Prior prospective studies that examined the association between depression and risk of MI all had a relatively long follow-up period. For example, the most recent systematic review on this topic included 19 prospective studies that had follow-up periods ranging from 4.2 years to 37 years. 7 The same review suggests that studies with shorter periods of follow-up (<8 years) are more equivocal. Yet demonstrating that depression increases MI risk over shorter time periods will have important public health and clinical implications.
Western findings have suggested that men’s MI is more related to depression than women’s. 15 A reason suggested relates to health-seeking behavior—women are more likely than men to seek help for mental health concerns. 15 By the same token, individuals of different ages and socioeconomic status in China may differ in treatment-seeking behavior due to differences in mental health literacy and opportunities for mental health care. A better understanding of heterogeneity in the depression–MI association would inform intervention.
Using a prospective cohort design, this study tests the hypothesis that depression is associated with an increased risk of MI within a 2-year period among Chinese middle-aged and older adults. In addition, we explore whether the association varies by sociodemographic characteristics, including age, gender, and socioeconomic status. According to the Global Burden of Disease 2019 Study, death rates due to coronary heart disease; a condition that leads to MI would be increasing in many locations across South, East, and Southeastern Asia including China. 16 Our study will not only test the generalizability of Western findings in China but may also add insights into potential ways to reduce MI-related morbidity and mortality in many countries of the Asia-Pacific region.
Methods
Data and Sample
We used baseline and Wave 2 (2011 and 2013) data from the China Health and Retirement Longitudinal Study (CHARLS) for this analysis. 17 At Wave 2, close relatives of respondents who were deceased by Wave 2 were interviewed, providing data about the MI status before the respondents died. The CHARLS was modeled after the Health and Retirement Study (HRS) in the United States. 18 Using multistage clustering sampling, a national probability sample of community-dwelling adults aged 45 years and older and their spouses of any age were interviewed at their homes at baseline. The sampling method and research design of the CHARLS have been reported elsewhere. 17 All participants signed informed consent. CHARLS data can be accessed at http://charls.pku.edu.cn.
For this analysis, we restricted the sample to those aged 45 years and older at baseline. Of them, 14 787 were reinterviewed, 439 were deceased, and 1998 were lost at Wave 2. Our analyzed sample (N = 15 226) included baseline respondents who were reinterviewed and those who were deceased at Wave 2. Compared with the lost respondents, the analyzed sample was older and more likely to have low education, low household assets, and rural residence.
Variables and Measures
Myocardial Infarction within a 2-year period was dichotomously coded (1 = having MI between baseline and Wave 2, 0 = not). At the Wave 2 follow-up, respondents were asked about heart disease (“Have you been diagnosed by a doctor with heart attack, coronary heart disease, angina, congestive heart failure, or other heart problems?”) Those who responded yes were asked, “Since your last interview two years ago, have you had a heart attack?” and, if the answer was affirmative, “What was the date of your most recent heart attack?” Based on the answers provided, we grouped respondents into two categories: having experienced an MI between baseline and Wave 2 and not. Similar questions were asked in the exit interview for close relatives of deceased respondents.
Depression
The CHARLS included the 10-item Center for Epidemiological Studies Depression scale (CESD-10). After reverse-coding two items and then summing all items, the total score of the CESD-10 ranged from 0 to 30. Higher scores indicated more severe symptoms (Cronbach’s α = .80). A prior study suggests a cutoff point of 12 to identify those with clinically significant depression in Chinese older adults. 19 We used a dichotomously coded variable (clinically significant depression; 1 = yes, 0 = no) and a continuous variable (CESD-10 total score), measured at baseline, to examine the association between baseline depression and the risk of MI in the subsequent 2 years.
Covariates
Three sets of variables were selected as covariates based on the literature.20-22 They were all measured at baseline. The first set is sociodemographic characteristics including age (in years), gender (1 = men, 0 = women), educational level (illiterate, elementary, middle school, high school or more), residential area (1 = rural, 0 = urban), and household assets (low, medium, high). Household assets were assessed by a count of the following 13 items owned by the household: refrigerator, washing machine, television, computer, stereo system, camera, air conditioner, mobile phone, furniture, music instrument, valuable ornaments, precious metal, and valuable artistic work. The total count was divided into three equal parts to indicate high, medium, and low assets.
The second set of covariates is medical conditions. We controlled for baseline heart disease, stroke, hypertension, dyslipidemia, diabetes, and kidney disease. Each was coded dichotomously (1 = yes, 0 = no). The questions asking about diseases in CHARLS are standardized; for example, for hypertension, the question is, “Have you been diagnosed by a doctor with hypertension?” In addition, we controlled for disease burden, indicated by a count of seven other conditions (cancer, lung disease, liver disease, digestive disease, memory-related disease, arthritis, and asthma) that the respondents may have had.
The third set is lifestyle factors, including smoking, drinking, weight, and physical activity. Smoking was coded dichotomously (1 = currently smoking, 0 = not currently smoking). Drinking had three categories: no, light, and heavy drinking. Respondents who drank lesss than once a month were considered not drinking. Those who drank once a month or more were classified as heavy drining if they consumed five or more “standard” drinks in each occasion, or light drinknig if they did not. 23 Weight was coded dichotomously (1 = overweight or obese, 0 = not) based on body mass index (BMI ≥24 kg/m2 was classified as overweight or obese). For respondents missing BMI, waist circumference (>90 cm for men and >80 cm for women to indicate overweight/obese) was used instead. 24 Physical activity was coded in three categories: some physical activity (≥10 minutes a week on moderate or vigorous activities), no physical activity (<10 minutes a week), and missing. Only a random subsample (40%) was asked the physical activity questions. Those who were not asked the questions were classified as missing the data.
Statistical Analysis
We used logistic regression to examine the association between baseline depression and MI between baseline and Wave 2. We estimated three models. First, we entered baseline heart disease and sociodemographic characteristics as covariates. By controlling for baseline heart disease, we estimated the association between baseline depression and the risk of MI in the following 2 years, regardless of having heart disease or not prior to baseline. Other medical conditions and lifestyle factors were sequentially added to the second and final models. We used interaction terms (e.g., clinically significant Depression × gender) to test whether the association between depression and MI varies by each of the sociodemographic characteristics. Each interaction term was entered into the final model separately.
The analysis was weighted to adjust for sample selection at baseline and attrition due to loss at follow-up. The CHARLS research team provided the baseline weights. We calculated inverse probability weights for loss. Because some respondents were from the same household, robust standard errors for clustered data were used. Missing data for most study variables were modest (<7%). The three variables with the highest percentage of missing were depression (12.5%), weight (19.3%), and physical activity (60.3%; they were not asked about physical activity.) We conducted multiple imputation. Results reported in the following are based on 10 multiple-imputed replicates. Statistical significance was set at P < .05 (two-tailed). Stata 14 was used in all analyses. 25 To check the robustness of the findings, we conducted sensitivity analysis using (1) complete case (N = 10 587), (2) respondents without missing values on physical activity (N = 6047), and (3) three-category coding for smoking (currently smoking, quit smoking, and never smoke) and weight (obese, overweight, and normal; N = 15 226). The results of all the extra analyses are similar to what is reported here (see supplemental materials).
Results
Sample Characteristics
Table 1 presents both weighted and unweighted descriptive statistics of the study variables. On average, the weighted sample was aged about 60 years at baseline, with about 48% men. Slightly more than two thirds (66.3%) had elementary school or lower education, and 54% lived in rural areas. About 27% had clinically significant depression at baseline, and the mean CESD-10 score was 8.3 (SD = 6.2). Those with and without clinically significant depression were significantly different (P < .05) in all sociodemographic characteristics, lifestyle factors, and medical conditions.
Descriptive Statistics of Study Variables.
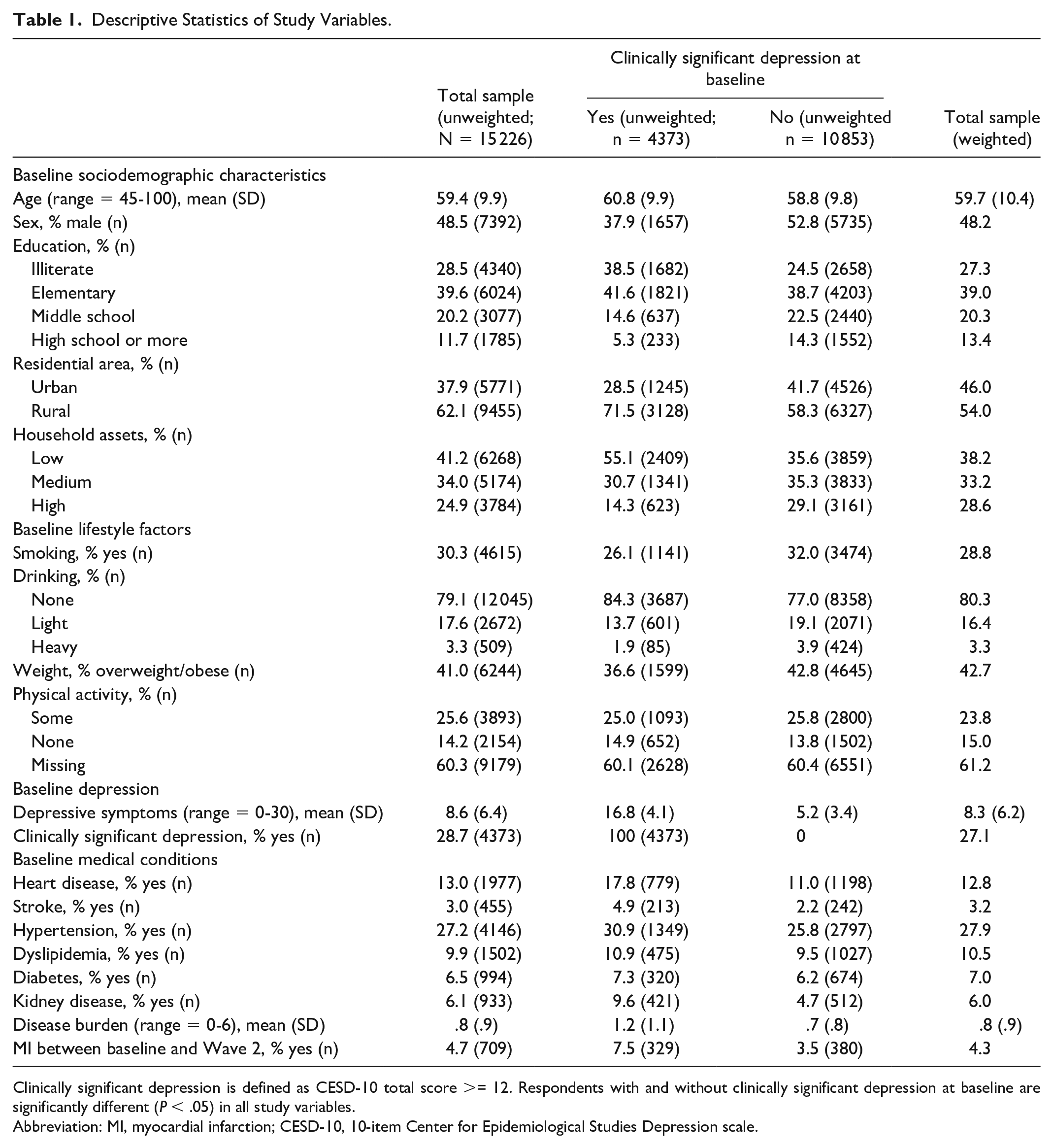
Clinically significant depression is defined as CESD-10 total score >= 12. Respondents with and without clinically significant depression at baseline are significantly different (P < .05) in all study variables.
Abbreviation: MI, myocardial infarction; CESD-10, 10-item Center for Epidemiological Studies Depression scale.
Associations of Depression and MI Within 2 Years
About 4.3% of the sample (weighted) had an MI between baseline and Wave 2, with a higher percentage among those with clinically significant depression (7.3%) than those without (3.2%). In the logistic regression model that adjusts for heart disease and sociodemographic characteristics (Model 1, Table 2), the odds of having an MI are 57% higher (OR = 1.57, 95% confidence interval [CI] [1.22, 2.01]) for respondents who had clinically significant depression at baseline than for respondents who did not. The odds ratio (OR = 1.45, 95% CI [1.12, 1.86]) is slightly reduced after controlling for other medical conditions (Model 2), but adding lifestyle factors as covariates does not change the estimates (Model 3). In the final model that controls for all covariates (Model 3, Table 2), having clinically significant depression at baseline is associated with 46% greater odds (OR = 1.46, 95% CI [1.13, 1.88]) of having an MI in the subsequent two years.
Logistic Regression Models Predicting MI Within a 2-Year Period (N = 15 226).
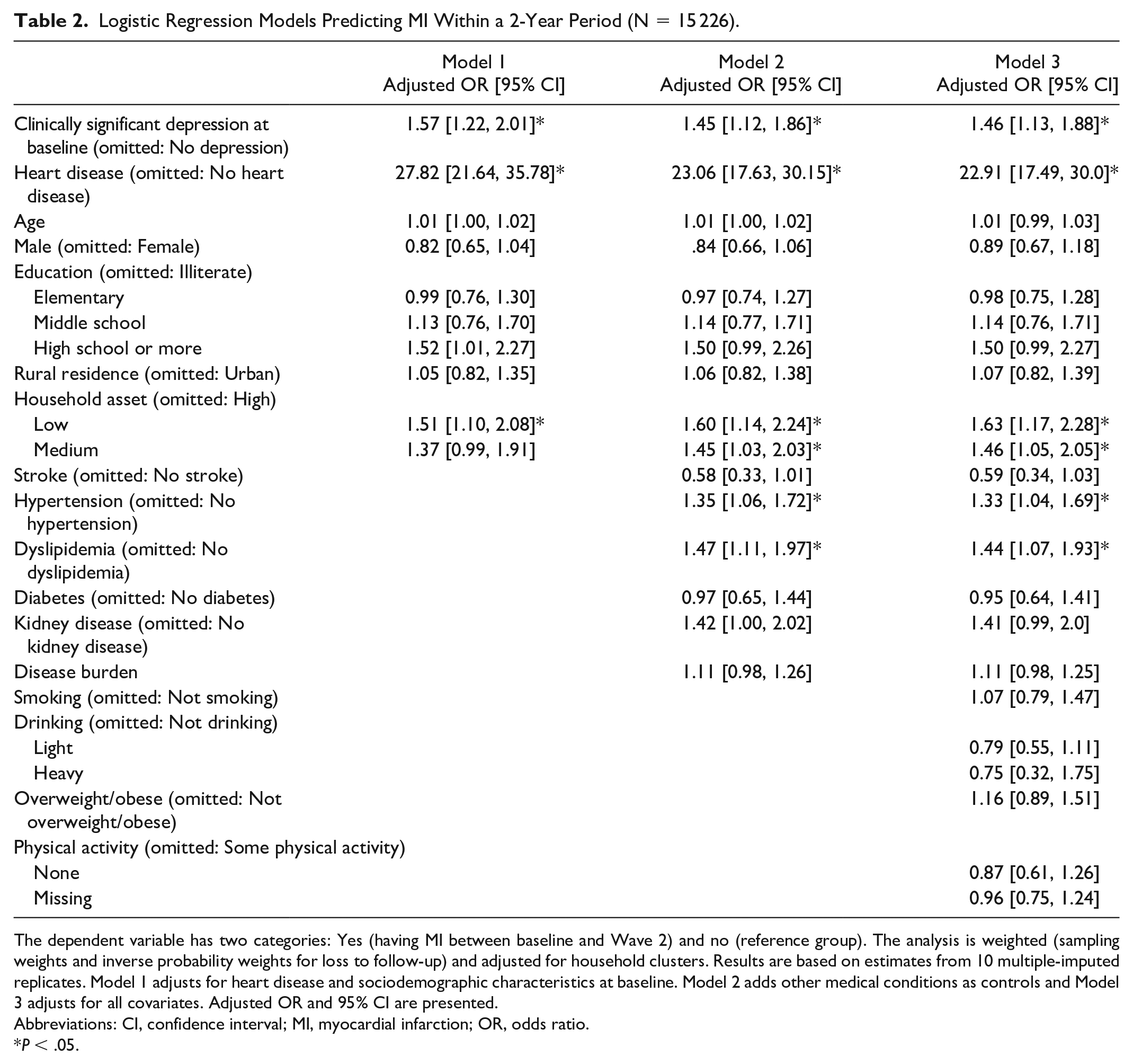
The dependent variable has two categories: Yes (having MI between baseline and Wave 2) and no (reference group). The analysis is weighted (sampling weights and inverse probability weights for loss to follow-up) and adjusted for household clusters. Results are based on estimates from 10 multiple-imputed replicates. Model 1 adjusts for heart disease and sociodemographic characteristics at baseline. Model 2 adds other medical conditions as controls and Model 3 adjusts for all covariates. Adjusted OR and 95% CI are presented.
Abbreviations: CI, confidence interval; MI, myocardial infarction; OR, odds ratio.
P < .05.
We also used depression as a continuous variable (CESD-10 total score) to estimate the logistic regression models described above. In the final model that adjusts for all covariates, the odds ratio of CESD-10 is 1.04 (95% CI [1.02, 1.06]). Based on this model, and using the marginal standardization method, 26 we plotted predicted probabilities of having an MI within a 2-year period by baseline CESD-10 scores (Figure 1). As shown, the probability gradually increases with more severe symptoms at baseline, approximating a dose–response relationship.
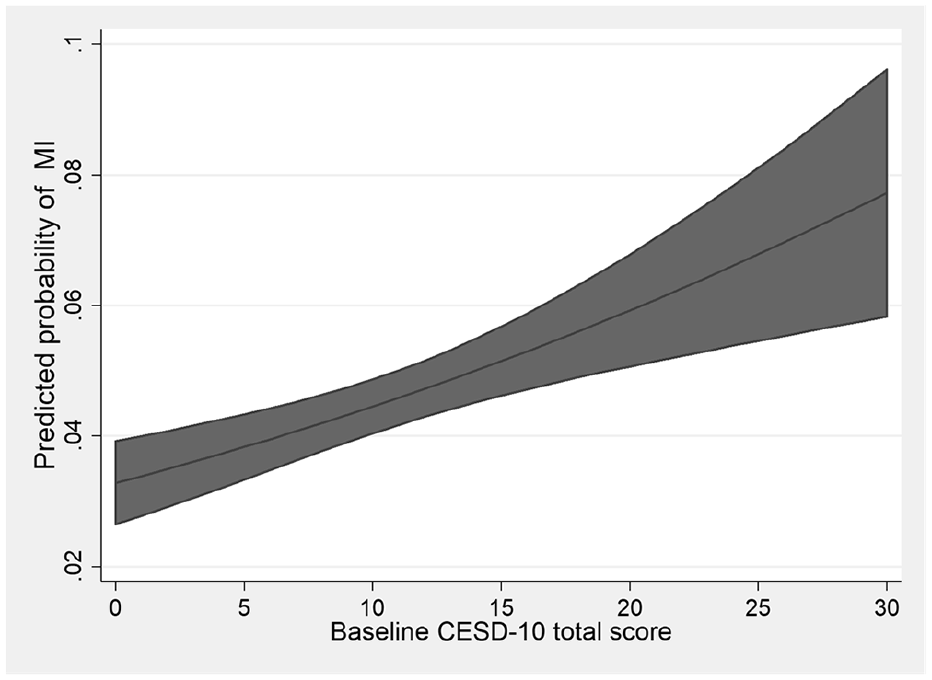
Predicted probabilities of having an MI, within a 2-year period, by baseline CESD-10 scores. Predicted probabilities are calculated using marginal standardization and based on a model adjusting for heart disease, other medical conditions, sociodemographic characteristics, and lifestyle factors at baseline.
We tested the interaction of depression and each of the sociodemographic characteristics (age, gender, education, rural/urban residence, and household assets) on follow-up MI. No significant interaction effects were detected.
Discussion
Using a prospective cohort design, we found that baseline depression, measured dichotomously as clinically significant depression and continuously to represent the severity of symptoms, is associated with risk of MI in the subsequent 2 years, even after controlling for a wide range of covariates. Our study is the first to report an association between depression and subsequent risks of MI in China. We are also the first to demonstrate an association between depression and the risk of MI over a relatively short period of time (2 years). We found no evidence that the association between depression and MI varies by sociodemographic characteristics, which suggests that depression is a shared risk factor of MI across sociodemographic groups in Chinese adults. The tighter temporal relationship between depression and MI, the robustness of the findings, and the observation of the same relationship in China as in the West reinforce the likelihood that when there is depression the risk of MI is greater.
How depression is linked to MI is not completely clear. Various mechanisms have been proposed. One is that depression is associated with pathophysiological changes that increase the risk of MI.15,27 These pathophysiological changes include alteration of the hypothalamic–pituitary–adrenal axis and sympathetic–adrenal–medullary system, activation of inflammatory processes, decreased heart variability, and increased platelet reactivity. Behavioral pathways, including depression leadng to poor medication adherence and health behaviors that increase the risk of MI, have also been suggested. 15 However, we do not find lifestyle factors to account for the association between depression and MI.
About 27% of our sample were classified to have clinically significant depression. This rate seems high, but it is comparable to the pool prevalence of depressive symptoms (23.6%) reported by a meta-analysis of studies that used screening scales to assess depression in Chinese older adults. 28 We used a cutoff point on a screening instrument to define clinically significant depression, which likely included those who did not meet the Diagnostic and Statistical Manual of Mental Disorders (DSM) criteria for a depression diagnosis. When using the CESD-10 as a continuous variable, we find that the probability of having an MI gradually increases with more severe symptoms. These findings suggest that, while severe depressive symptoms are associated with a greater risk of MI, even mild and subsyndromal depression matters and should be given attention.
Our findings have practical implications. Depression screening for middle-aged and older adults may help to identify those at risk of MI early. The utility of depression screening may be greater for China and other emerging economies where depression is on the rise but greatly under-recognized.13,29 If depression screening is integrated into routine health care practice, clinicians can use the depression screening data, and the history of medical conditions, particularly heart disease, to assess their patients’ risk of MI in the short term and develop treatment plans accordingly. The plan may include educating the patients and their families to recognize the warning signs of MI and take appropriate actions when symptoms are observed, as well as referring patients with clinically significant depression for further diagnosis and counseling. Such early interventions can potentially save lives, considering that MI often occurs at times not expected by the victims and prompt treatment of MI is a life-or-death matter. There have been initiatives to integrate depression screening and treatment in primary care clinics in rural China. 30 Such an integrated model may be applicable to many low-resource settings.
This study has several limitations. First, the MI measure may be biased as it is based on self-report. Respondents and their relatives may not accurately recall MI episodes. MIs with less intense symptoms may escape their awareness as well. We may have underestimated the relationship between depression and MI due to the reporting bias. Future research using medical records to assess MI would help to verify the findings. Second, we used a screening instrument to define clinically significant depression. Future studies should attempt to measure depression through clinical diagnosis as well as a standardized screening instrument, so as to discern how the two ways of measuring depression are related to the risk of MI. Third, we did not control for stressful events that can trigger both depression and MI, and hence could not rule out potential confounding effects. We also did not control for the duration and treatment of depression because the CHARLS did not collect such data. In an additional analysis, we controlled for whether the respondents were taking antidepressants, sleeping pills, or receiving any psychological or psychiatric treatment (1 = yes, 0 = no). Less than 1% of the sample gave an affirmative response. This additional analysis yielded the same results. The low treatment rate supports that depression is undertreated in China.
Conclusion
To conclude, using a prospective cohort design, we find that depression at baseline is associated with an increased risk of MI in the subsequent 2 years among Chinese adults aged 45 years and older. The association is robust and does not vary by sociodemographic characteristics. Our findings are consistent with those reported in developed Western countries. We add to the literature by demonstrating a tighter temporal relationship between depression and MI in China. The findings imply that early detection and treatment of depression may help to curb the rise of MI in China and beyond.
Supplemental Material
sj-docx-1-aph-10.1177_10105395221095331 – Supplemental material for Depression Is Associated With Myocardial Infarction Within a 2-Year Period Among Adults in China
Supplemental material, sj-docx-1-aph-10.1177_10105395221095331 for Depression Is Associated With Myocardial Infarction Within a 2-Year Period Among Adults in China by Lydia W. Li, Greta Jianjia Cheng, Hongwei Xu, Zhenmei Zhang, Jinyu Liu and Yeates Conwell in Asia Pacific Journal of Public Health
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Institute of Mental Heatlh at the National Institute of Health (R01 MH100298).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.