
Abstract
Obesity prevalence has increased in low- and middle-income countries (LMICs) over the past several decades, with generally greater occurrence among adult females compared with males. Gendered variation in health behaviors, such as substance use, may play a role in how differences in obesity, body size, and composition manifest in association with sex. This study examines sex-moderated relationships of tobacco smoking and kava consumption with body composition and obesity among 301 Ni-Vanuatu (local self-identification meaning “of Vanuatu”) adults. Data collected included self-reported frequency of substance use as well as anthropometric measurements to assess body mass, composition, and obesity. Tobacco and kava use were associated with reduced measurements of body mass and adiposity in males, and kava use was associated with some elevated measurements of body mass and hip circumference in females. Kava use was also negatively associated with obesity based on waist-to-height ratio among males. These results have implications for evaluation and future research on substance control programs in this population.
What We Already Know
Obesity prevalence is increasing in low- and middle-income countries (LMICs) and is generally greater in prevalence among adult females compared with males.
Tobacco use is negatively associated with body mass index (BMI) and BMI-based obesity, and is generally more common among men than women in LMICs. Substances may also interact differently with sex-associated physiologies to influence body mass and composition.
The relationship of kava consumption with body mass, composition, and obesity has been understudied.
What This Article Adds
In this sample from Vanuatu, tobacco use and kava consumption were associated with some measurements of body mass, composition, and obesity and many of these relationships were moderated by sex.
Substance use may play a role in the sex-associated obesity disparity in Vanuatu, but more research is needed to evaluate causality and potential interactions with other health behaviors.
The findings suggest that additional research is needed on whether substance control programs have implications for overweight and obesity in LMICs like Vanuatu.
Introduction
Economic development and globalization have contributed to a rapid increase in obesity prevalence in low- and middle-income countries (LMICs) over the past several decades, with an overall larger proportion of the burden borne by adult females as compared with adult males. 1 The “nutrition transition” model explains the increase in obesity prevalence as a result of changes in diet and physical activity patterns due to forces including urbanization and industrialization of food processes and has been supported across multiple LMICs. 2 However, these factors do not adequately explain the male-female obesity disparity. Suggested contributors to the disparity in the literature include factors associated with gender inequality (e.g., early life adversity contributing to a thrifty phenotype in girls, elevated psychological distress, or food insecurity in women) that may manifest as sex-associated variation, as well as sex-associated differences in propensities for body fatness related to the evolution of different reproductive strategies.3,4 Gendered variations in health behaviors, such as consumption of substances like tobacco that can influence weight gain and body fat deposition, may also play a role.
Tobacco use has increased in tandem with obesity prevalence in LMICs; the World Health Organization (WHO) 5 estimates that between 2000 and 2015, the number of smokers in LMICs increased by 33 million individuals. In 2015, the prevalence of tobacco smoking was estimated at 32.2% among men and 2.6% among women in this group of countries, inversely mirroring the sex-associated obesity disparity. 5 Tobacco use has been associated with reduced body mass index (BMI) and reduced risk of BMI-based obesity in multiple studies.6-8 Data on relationships between tobacco use and measurements of central adiposity/obesity are mixed, however.9-11 While no studies have directly interrogated the question of whether tobacco use contributes to male-female obesity disparities in LMICs, some authors have shown that these relationships do vary by sex.11,12 Pathways between tobacco use and body mass and composition may include influences of nicotine on appetite control 13 and metabolic regulation, 14 although it is unclear why the impacts of nicotine on these systems may differ in association with sex.
We have worked in the Republic of Vanuatu, an LMIC in the South Pacific, on social and behavioral risk factors for obesity during economic development since 2007. We have consistently found elevated prevalence of obesity in adult females as compared with males in areas more heavily impacted by factors associated with economic development, including urbanization and tourism.15,16 We have also found elevated tobacco use among men as compared with women. 17 This population also offers the opportunity to observe sex-associated relationships between another substance, kava, and variation in body composition and obesity prevalence. Kava (Piper methysticum) is a root crop native to the South Pacific that is used to produce a nonalcoholic beverage with intoxicant effects. 18 Documented physical and psychological effects of kava drinking include an immediate numbing of the tongue/mouth, feelings of relaxation and social affability, and reduced anxiety. 18 Although kava is used medicinally in the Pacific and is advertised as an herbal supplement in many countries, long-term use is also connected to dermatological conditions and liver toxicity. 19 Consumption of kava as both a ceremonial and recreational drink is widespread across the South Pacific, including in the Republic of Vanuatu, and has traditionally been more prevalent in men. 18 Its relationship to body composition and obesity risk has been little explored and merits further investigation. The objective of this study was to examine relationships between tobacco use and kava consumption with body mass, body composition, and obesity and to determine whether these relationships were moderated by sex. The study tested multiple measurements of body composition, given that substance use might impact location of fat deposition (e.g., centrally vs peripherally). The findings suggested implications for evaluation and research on substance control programs given potential interactions with weight management, as well as understanding the male/female obesity disparity in LMICs like Vanuatu.
Methods
Study Population and Sampling
The Republic of Vanuatu is an island nation in the South Pacific. The majority of Melanesian population are spread across 63 inhabited islands that vary in level of economic development. Data for this study were collected between June and August 2017 in two villages on two islands: Anelcauhat on Aneityum and Erakor on Efate. Anelcauhat is a rural village with access to tourists who visit off-shore “Mystery Island.” Erakor is a peri-urban village located 7 km from Port Vila, the urban capital of Vanuatu. At the time of the 2016 Vanuatu Mini Census, the population of Aneityum was 1402 and Efate was 83 989. 20
The study was approved by the Binghamton University IRB and the Vanuatu Ministry of Health before commencing. Participants were recruited via household-level convenience sampling methods. The research team visited households, explained the purpose of the survey, and verbally consented adult (aged 18 years and older) volunteers into the study. The research team comprised trained research assistants from Binghamton University and the local villages. A total of 367 adults took part in the study (148 males, 219 females). Analyzed here are results from 301 adults after removal of 8 individuals who did not permanently reside on the target islands, 10 pregnant females, 31 lactating females, and 17 individuals with incomplete anthropometric measurements.
Behavioral Survey
Participants were administered a sociobehavioral survey in Bislama, the lingua franca of Vanuatu. The survey was translated with the assistance of local research assistants and the Ministry of Health. Participants were asked to self-report their sex, and we use terms “male” and “female” to report our results here, given that we are reporting physiological outcomes. However, we acknowledge that our results are not reducible to the biology of sex alone. Data collected relevant to this study also included participant age and self-reported consumption patterns of tobacco and kava. These were coded as “regular use” if the participant reported that they consumed the substance and/or engaged in consumption at least once per week, with a dummy variable (regular user = 1, nonuser = 0) used in analyses.
Anthropometric Measurements and Obesity
Participants underwent multiple anthropometric measurements to assess body size, composition, and obesity. The variety of measurements used was necessary because substances like tobacco may influence different patterns of fat deposition at sites across the body. Participants were able to voluntarily refuse any measurement. All measurements were taken using standard guidelines outlined in the work by Lohman et al. 21 Participants wore light tropical clothing and removed shoes for height and weight measurements. Standing height was measured to the nearest 10th of a centimeter using a portable anthropometer. Weight was measured nearest 10th of a kilogram using an Omron Body Composition Monitor (Omron HBF-510W; Omron Healthcare Inc., Bannockburn, IL, USA) and in some cases (due to equipment malfunction) a digital commercial bathroom scale (there were no significant differences between the mean weight measurements taken by the different scales in the overall sample). Triceps, subscapular, suprailiac, and anterior thigh skinfold thicknesses were taken with a Lange skinfold caliper three times in millimeters, with the mean of the three measurements used in analyses. Skinfolds were used to calculate sum of four skinfolds (SSF) which is used in the analyses. Waist and hip circumferences were taken in centimeters using a flexible measuring tape. Waist circumference was taken at the midline (mid-point between the highest point of the iliac crest and the last floating rib) according to WHO guidelines. 22
A subsample of participants (n = 291) underwent leg-to-leg bioelectrical impedance analysis for percent body fat and percent visceral fat. Analyses presented here were from 243 individuals, after removal of individuals as described under “study population and sampling.” These were measured using the aforementioned Omron Body Composition Monitor and calculated using Omron’s proprietary formulas. Fewer participants underwent these measurements because of equipment malfunction in the field; this is reflected in different sample sizes in the data analysis.
Body mass index (BMI), a measure of overall body size but not composition, was calculated as weight (kg)/height (cm) 2 . Subscapular-to-triceps ratio (STR), a measure of body fat deposition on the trunk relative to the limbs, was calculated as subscapular skinfold (mm)/triceps skinfold (mm). Waist-to-height ratio (WHtR) was calculated as waist circumferences (cm)/height (cm). Waist-to-hip ratio (WHR) was calculated as waist circumference (cm)/hip circumference (cm). Both indices include waist circumference, but WHtR indicates size of the abdomen relative to the size of the body, and WHR provides information about relative fat distribution on the waist compared with the hips. 23
The WHO 24 cutoffs for obesity were used for BMI (BMI ≥30 kg/m2), waist circumference (class II obesity ≥102 cm for males, ≥88 cm for females), and percent body fat (>25% for males, >35% for females). The obesity cutoff used for WHtR were measurements >0.5. 23
Statistical Analyses
Descriptive analyses included comparisons of tobacco and kava use and obesity prevalence by island and sex; statistical significance was assessed using logistic regression. Other descriptive analysis included comparisons of mean anthropometric measurements and indices by island and sex, and statistical significance was assessed using analysis of variance.
Relationships between substance use (predictor of interest) and linear anthropometric measurements and indices (dependent variables) were analyzed using separate linear regression analyses for each anthropometric characteristic. Models were assessed for regression assumptions, and in some cases (visceral fat and BMI), the model residuals were not normally distributed. These models were run again with the dependent variables log-transformed, but this did not change the nature of results. Thus, the untransformed data were used in the presented analysis. Unique R 2 was calculated as a measure of effect size in these models.
Relationships between substance use (predictor of interest) and obesity (dependent variable) were analyzed using logistic regression analysis, and odds ratio (OR) was calculated as a measure of effect size. All of the initial linear and logistic regression models included age, sex, and island of residence as controls.
We also tested sex moderation of relationships through interaction terms between sex and substance use in both the linear and logistic regression models, and interactions significant at P ≤ .05 were analyzed in sex-disaggregated models. Age and island of residence were included as controls in these models.
Analyses were conducted using SPSS 26.0, and P < .05 was the accepted level of statistical significance. Note that tables in the results present only the effects of substance use (tobacco or kava) on the measurements of body size, composition, and obesity; full models with all covariates are presented in Supplemental Information.
Results
Baseline Substance Use, Body Composition, and Obesity Patterns by Island and Sex
Mean age of the sample was 41.77 ± 15.56 years, with no significant differences by island or sex. Table 1 shows baseline substance use, body size and composition, and obesity patterns by island and sex. Regular use of both tobacco and kava were significantly more common among males than females. There were no major statistically significant differences in tobacco and kava use between islands. The data showed a general pattern of elevated body fatness and obesity prevalence among females as compared with males. Body size and fatness were generally similar between islands, and no measurements of obesity were significantly different between islands.
Baseline Unadjusted Sample Descriptive Characteristics by Sex and Island.
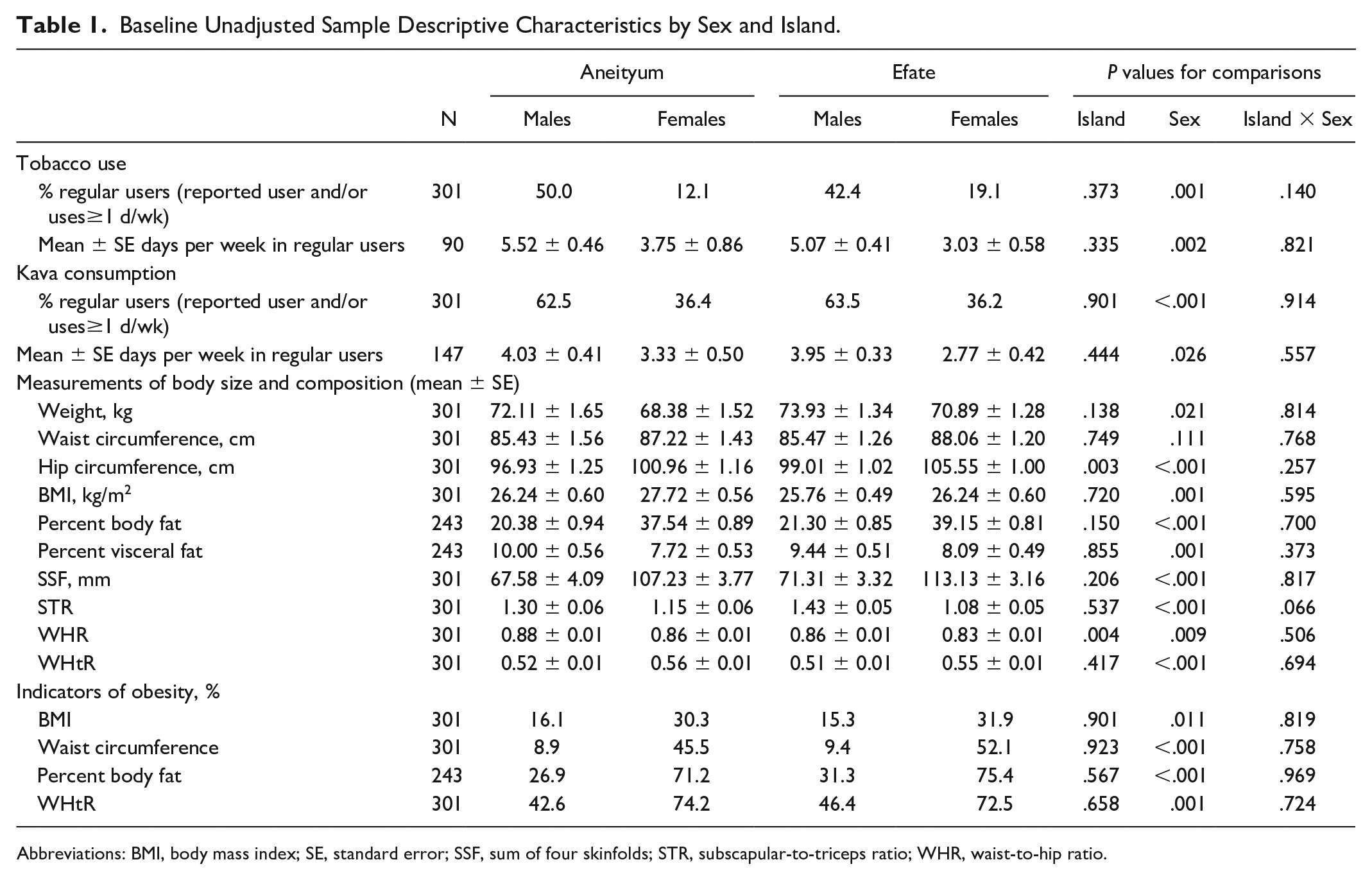
Abbreviations: BMI, body mass index; SE, standard error; SSF, sum of four skinfolds; STR, subscapular-to-triceps ratio; WHR, waist-to-hip ratio.
Relationship of Tobacco Use to Body Composition and Obesity Risk
In models controlling for age, island of residence, and sex, tobacco use was negatively and significantly associated with waist circumference (B = −2.93, P < .05), BMI (B= −1.17, P < .05), percent body fat (B = −2.58, P < .01), percent visceral fat (B = −1.49, P < .01), SSF (B = −9.06, P < .05), and WHtR (B = −0.02, P < .05) (full analysis shown in Supplemental Appendix 1). We detected significant interactions between tobacco use and sex on weight, waist circumference, hip circumference, percent body fat, percent visceral fat, and WHtR (Table 2, model 2). Effect sizes in these models were small. In sex-disaggregated models (Table 3), regular tobacco use explained between 3.1% and 8.6% of the variance in weight, waist circumference, percent body fat, percent visceral fat, SSF, and WHtR in males and was significantly and negatively associated with each of these measures. No measures of body size or fatness were significantly associated with tobacco use in females. Full models showing all covariates are available in Supplemental Appendices 1 and 2.
Linear Regressions of Tobacco and Kava Use on Measurements of Body Size and Composition for Models With Significant Sex × Substance Interactions.
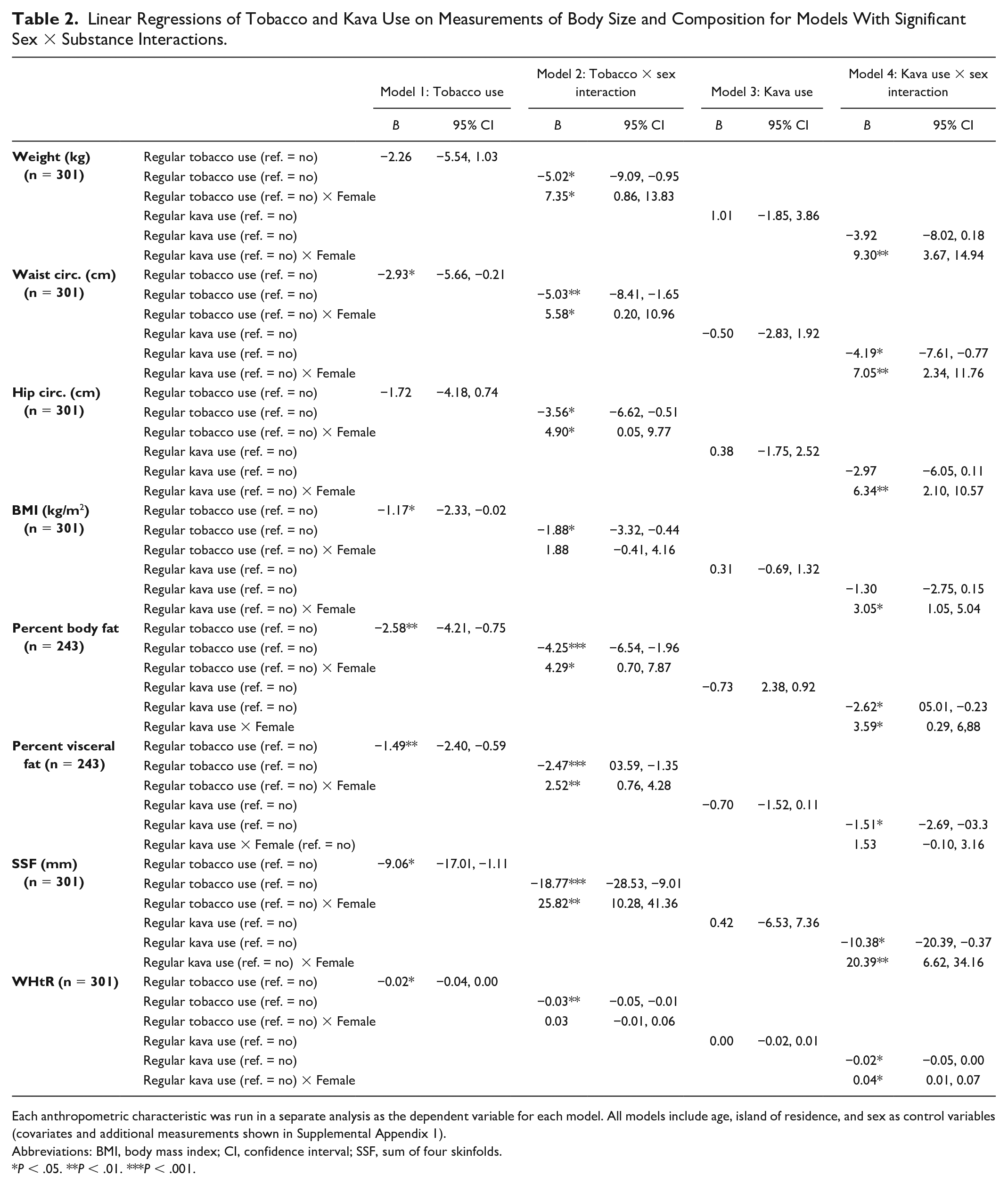
Each anthropometric characteristic was run in a separate analysis as the dependent variable for each model. All models include age, island of residence, and sex as control variables (covariates and additional measurements shown in Supplemental Appendix 1).
Abbreviations: BMI, body mass index; CI, confidence interval; SSF, sum of four skinfolds.
P < .05. **P < .01. ***P < .001.
Sex-Disaggregated Linear Regression Analysis of Variables With Significant Sex × Substance Interactions From Table 2.
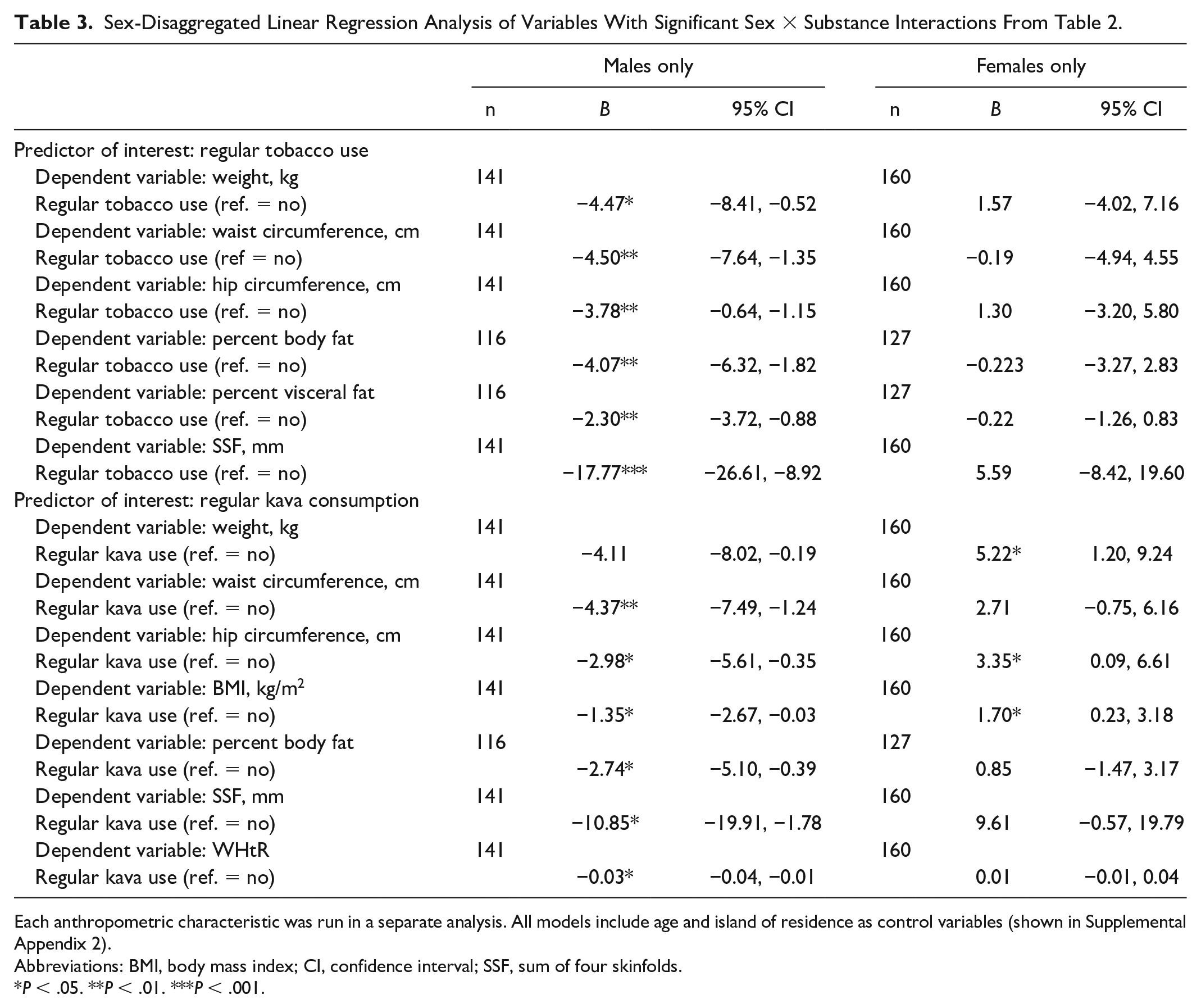
Each anthropometric characteristic was run in a separate analysis. All models include age and island of residence as control variables (shown in Supplemental Appendix 2).
Abbreviations: BMI, body mass index; CI, confidence interval; SSF, sum of four skinfolds.
P < .05. **P < .01. ***P < .001.
Regular tobacco use was negatively associated with obesity based on percent body fat (OR = 0.45, 95% confidence interval [CI] [0.23, 0.88], P < .05) and WHtR (OR = 0.27, 95% CI [0.14, 0.52], P < .001). There was no evidence of a statistically significant interaction between tobacco use and sex on any indicator of obesity. The full models are available in Supplemental Appendix 3.
Relationship of Kava Consumption to Body Composition and Obesity Risk
In models controlling for age, island of residence, and sex, regular kava consumption was not associated with any measurement on its own (Supplemental Appendix 1). We found evidence of an interaction between sex and kava consumption on weight, waist circumference, hip circumference, BMI, percent body fat, SSF, and WHtR (Table 2, model 4). In sex-disaggregated models among males, kava consumption was negatively associated with weight, waist and hip circumferences, BMI, percent body fat, SSF, and WHtR (Table 3). Kava consumption explained between 2.7% and 3.5% of the variance in these models. Among females, kava consumption was significantly positively associated with weight, hip circumference, and BMI. Kava consumption explained between 2.3% and 4.0% of the variance in these models (Table 3). Full models showing all covariates are available in Supplemental Appendices 1 and 2.
On its own, although there was a trend indicating that kava use was negatively associated with obesity, the models were not significant (Supplemental Appendix 3). We found evidence of an interaction between kava consumption × female sex on obesity based on WHtR (OR = 6.97, 95% CI [2.02, 24.05], P < .01). In sex-disaggregated models, kava consumption significantly predicted reduced odds of obesity based on WHtR among males (OR = 0.17, 95% CI [0.06, 0.46], P < .01), with no significant relationship among females (OR = 1.60, 95% CI [0.69, 3.74]). Tables showing logistic regression models are available in Supplemental Appendices 3 and 4.
Discussion
Summary
Obesity was more common among females than males in our sample, and in contrast, tobacco use and kava consumption were more common among males than females. In general, we found evidence of a negative relationship between tobacco use and measurements of body mass and central adiposity among males, but not females, in this sample. Tobacco use was also negatively associated with obesity based on WHtR and percent body fat, with no significant indications of sex moderation. We also found a pattern of negative association between kava consumption and measurements of body size and fatness among males, with the opposite or no trend found in females. Kava consumption was also negatively associated with WHtR-based obesity among males. Limitations to these findings include that we have not quantified dosage of tobacco or kava; it is possible that males consume more in one sitting than females given that traditionally; the practice of kava consumption has been dominated by men. 18 There may also be socioeconomic confounders in these relationships that were not possible to assess in this sample. Socioeconomic status is difficult to measure in Vanuatu, and based on our ethnographic field experience, we note that many individuals have limited or inconsistent interaction with the cash economy. In addition, households may grow tobacco and kava in their gardens, so access may not be dependent on income. Other limitations are elaborated in the discussion below. Overall, however, we have found evidence of sex-moderated relationships between kava and especially tobacco use and body mass, as well as overall and anthropometric site-specific adiposity, and obesity. These effects are larger among males than females, and we suggest substance use may contribute to some of the sex-associated variation in body mass, composition, and obesity observed in Vanuatu, pending future longitudinal research.
Tobacco Use, Body Measurements, and Obesity Risk
We found a statistically significant negative relationship between tobacco use and BMI, which is consistent with findings in other diverse populations where tobacco use is associated with reduced BMI and BMI-based obesity risk.6-8 As well as a negative association between weight and tobacco use among men. We also report a negative association between obesity based on percent body fat and WHtR (a measure of central obesity). Population-based studies are inconsistent on the relationship between tobacco use and central adiposity/obesity,9-11 partially due to inadequate understanding of confounders across diverse populations. 25 Potential confounders may include other health behaviors, such as physical activity or dietary patterns, that may covary with substance use. In contrast to our findings, multiple studies show a positive relationship between tobacco use/smoking and central adiposity/obesity. For example, Garcia-Alavarez et al 26 showed a positive relationship between smoking and central body fatness in males in Spain, and Akbartabartoori et al 12 reported that cigarette smoking was linked to elevated central adiposity in females in Scotland. Altogether, our data indicate that tobacco use in this sample is associated with reduced body size as well as reduced central adiposity in males, given that we did not find significant relationships with STR, a measure of body fatness on the limbs relative to the trunk, or hip circumference. More research is needed to determine whether this is a widespread pattern among Melanesians and/or Pacific islanders, perhaps due to culturally specific interactions between tobacco use and other health behaviors such as physical activity, diet, and use of other substances like kava.
Why tobacco use is largely related to reduced indicators of body size and adiposity in males in this sample and not females is unclear. Nicotine in tobacco is a known appetite suppressant that alters eating/feeding behaviors through multiple mechanisms, 27 although the effect of nicotine on males and females should presumably be the same. We noted that male users reported using tobacco more frequently than female users, which could indicate a larger dosage. It is also possible that our method of quantifying smoking frequency (i.e., days per week) is inadequate to capture an accurate reflection of dosage of active ingredients like nicotine, or that men and women use different sources of tobacco (e.g., homegrown vs purchased cigarettes) which may impact nicotine exposure. We also noted before that dosage might differ based on gendered consumption behaviors. In addition, body fat is elevated in females as compared with males generally, likely related to the energetic costs associated with gestation and lactation.3,4 It is possible that relationships between substance use and body size and fat deposition may be masked in bodies with a larger proportion of adipose tissue. Future research should include quantification of chronic nicotine exposure, such as through measurement of cotinine in biological samples, and longitudinal data collection, to illuminate causation. This will also help address other confounders such as second-hand exposure or exposure through skin contact when processing homegrown tobacco.
Other studies have shown different interactions between tobacco use and body weight/composition in males and females, consistent with conclusions by Lv et al. 11 that the “buffering” effect of tobacco against weight gain is often stronger in males than females. It is unclear whether this is an effect of sex (e.g., interactions between nicotine and sex-associated/metabolic hormones) and/or gender (e.g., smoking is associated with different health behaviors in men and women), although some studies indicate that smoking effects endocrine function in females. 28 In addition, other health behaviors that vary between men and women (such as dietary or physical activity patterns) may covary with substance use, and the social acceptability of tobacco use may be gendered, influencing the overall frequency of smoking and dosage of intake that may be reflected in sex-associated differences. Overall, the relationship between tobacco use, sex/gender, and body composition/obesity is complicated, and more research with additional control variables are needed across diverse populations.
Kava Use, Body Composition, and Obesity Risk
We found some evidence of a relationship between kava use and body mass, adiposity, and obesity moderated by sex in our sample from Vanuatu, with different relationships in males (negative) and females (positive or no relationship). Very little is known about the relationship between kava use and body composition, and more research among larger samples is needed to understand potential interactions between kava and use of other substances. 29 In an Aboriginal Australian population, Clough et al. 29 reported that heavy kava use was negatively associated with triceps and subscapular skinfold thicknesses, BMI, and percent body fat, generally consistent with our results among males, although the analyses did not consider males and females separately. The study also examined biomarkers of metabolic syndrome and found that kava use was predictive of elevated low-density lipoprotein and total cholesterol. 28 An earlier study conducted in the same region by Mathews et al. 30 reported that 20% of kava users were underweight, and that kava use was associated with reduced appetite. However, these studies did not address concordance between tobacco and kava use. We have anecdotally observed in Vanuatu that smoking occurs most frequently in kava bars in Vanuatu rather than at home or other settings. Our quantitative data supported this observation; in this sample, 25.9% of regular kava drinkers also reported regular smoking, while only 3.9% of nondrinkers reported regular smoking (P < .001). It is thus possible that the observed association between kava use and body composition in males is actually due to the effects of tobacco. A larger sample of individuals who smoke independently of kava use, and vice versa, is necessary to meaningfully parse this relationship. In addition, this supposition did not explain why we observed a positive relationship between kava use and some measurements in females. We have observed during field work that kava drinkers also consume snack foods, such as raw sugarcane, following kava consumption, which may contribute to our observed results. However, this does not explain the inverse relationship observed in males. Finally, we also observed that kava use was associated with reduced odds of obesity based on WHtR among males, but not females. No other published studies that we are aware of have examined the relationship of kava consumption to obesity, but this finding is consistent with demonstrated relationships between kava and body size/composition.
Conclusion
Many of the relationships we have found among tobacco use and kava consumption with measurements of body mass, composition, and obesity are moderated by sex in our sample of Melanesian adults from Vanuatu, and future longitudinal research can illuminate whether these relationships contribute even small effects to the male/female obesity disparity. Tobacco use is predictive of lower weight and body fatness among males in our sample, with no apparent relationships among females. Kava consumption is predictive of lower body mass and fatness among males, but some elevated measurements among females. We have found some evidence that consumption of these substances is negatively associated with obesity. More studies are necessary to investigate potential interactions among factors including substance use and other health behaviors and mechanisms through which these behaviors impact sex-associated physiological outcomes. Research on whether substance use is causally related to body size and composition in this population is needed due to potential implications for substance use programs and messaging regarding weight management.
Supplemental Material
sj-pdf-1-aph-10.1177_10105395221108593 – Supplemental material for Relationships of Tobacco Use and Kava Consumption to Sex-Associated Variation in Body Composition and Obesity Risk in Melanesian Adults From Vanuatu
Supplemental material, sj-pdf-1-aph-10.1177_10105395221108593 for Relationships of Tobacco Use and Kava Consumption to Sex-Associated Variation in Body Composition and Obesity Risk in Melanesian Adults From Vanuatu by Kathryn M. Olszowy, Amanda B. Roome, Elisabeth Standard, Len Tarivonda, George Taleo and Kelsey N. Dancause in Asia Pacific Journal of Public Health
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a Post-PhD Research Grant from the Wenner-Gren Foundation for Anthropological Research.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.