
Abstract

Introduction
Globally, as of June 25, 2022, the cumulative number of cases reported is more than 550 million and the number of deaths exceeds 6 million. 1
The aim of current research was to study the anti-COVID-19 measures implemented in the Republic of Armenia (RA) and identify main barriers and challenges. Armenia is a landlocked low-middle-income country with limited recourses.
Materials and Methods
Following sources were used and analyzed:
- Official statistical data of the Ministry of Health (MoH) and other relevant authorities;
- Resolutions and decrees of the RA Government and Emergency Commandant;
- Official statements of the state authorities’ published through the mass and official social media;
- Official information provided by the state authorities per our request.
Results and Discussion
The first case of COVID-19 was detected in Armenia on January 3, 2020, with a citizen returned from Iran. According to the mass media statement of the Prime Minister, all necessary measures were taken to detect and isolate all contacted persons.
Considering the increased spread of the COVID-19 in Armenia, the Government declared state of emergency on March 16, 2020, which was then periodically extended. 2 Later, the legal State of Emergency was terminated and the RA Government Decree 1514-N on the introduction of quarantine in connection with COVID-19 entered into force, according to which quarantine was established and certain restrictions were applied throughout the RA from September 11, 2020. Since then, the Government was extending the quarantine every 6 months until June 20, 2022. 3
The MoH developed and adopted the guideline on surveillance, case investigation, and home care of COVID-19 uncomplicated and mild cases. The document stated preference for isolated COVID-19 patients in hospitals and specialized locations, but in case of limited capacities, primary health care physicians can manage patients with uncomplicated and mild forms of disease at home. The health status of the contact person should be monitored for 14 days. 4
With subsequent changes in the law, 5 amendments were made to the State of Emergency Decree which anticipated that the operators of the public electronic communication networks would transmit the data through Virtual Private Network to the e-Governance infrastructure implementation agency (Figure 1). These data would include information about persons being tested, infected, having symptoms of illness, sickness, treatment and their contacts, as well as the data necessary to determine the location of provided health service to isolated person (customer location), as well as phone numbers and those who had communication with particular individual (associated mobile number) up to 14 days ago.
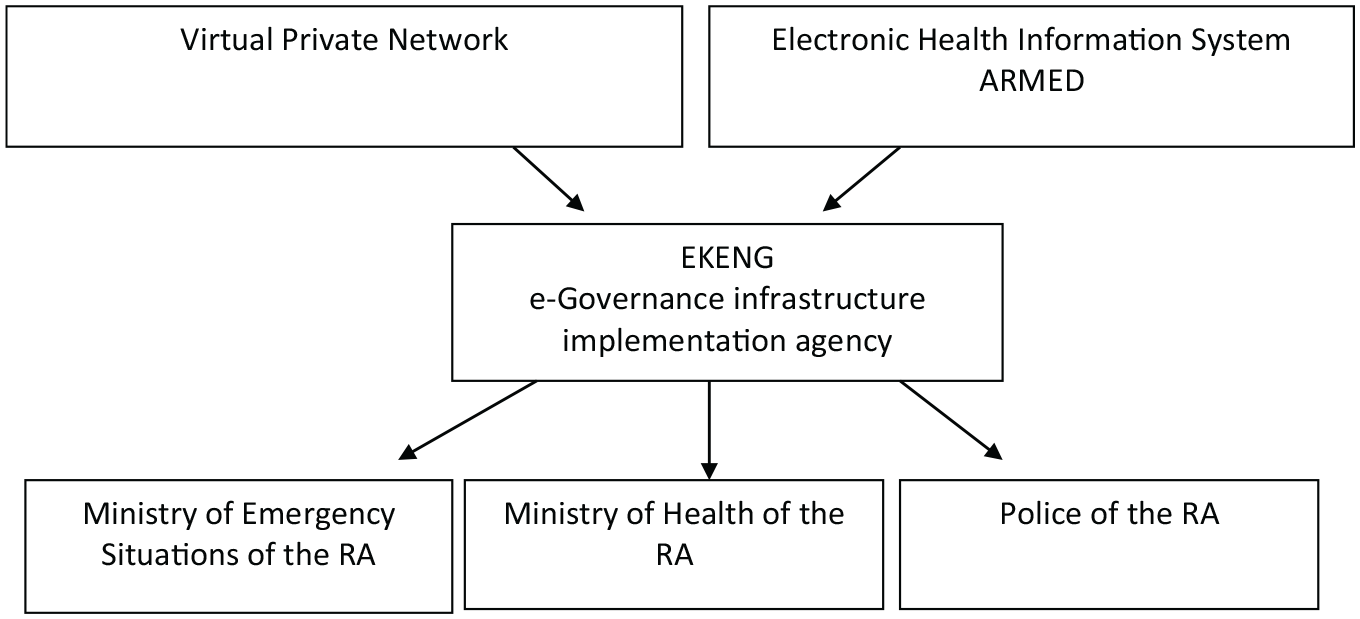
Organization of health information flow.
Based on the legal framework assessment, the process of contact tracing (CT) and their monitoring could be conditionally divided in two main stages: first—before the relevant amendments were made to the law On the Legal Regime of the State of Emergency, when the contact detection process was organized and carried out without the use of electronic communications and software; second—after the implementation of corresponding changes using electronic means of communication and software.
At the initial stage of the pandemic, efforts were made to detect and isolate (self-isolate) all contacts. Later, increasing number of cases and scarce human resources involved in the detection led to a sharp decrease in the effectiveness of this process, causing worsening of the epidemic situation. The use of special software appeared to be not effective. During operational period of special software (April 4, 2020-September 11, 2020), on average, the data of 67 infected persons were analyzed per day by the special software and the number of contacts identified was only 10. Consequently, one full-time operator processes an average data of only three infected persons per day and five operators identify only two contacts per day. In comparison, during the same period, there were 44 590 confirmed cases and the average daily number of cases was 277. 6 By matching the data obtained from the office of the Deputy Prime Minister with the actual one, we concluded that contacts of only one from four infected persons were processed by this special system, which is obviously far insufficient for effective CT particularly for COVID-19 control.
In addition, we found no data concerning relevant permits, knowledge, skills, and special trainings of responsible persons involved in CT and dealing with the personal data. No information was found about organization of any awareness programs and/or medical staff trainings prior to adoption of the regulations.
Conclusion and Recommendations
Contact tracing, along with testing and isolation, plays an important role in COVID-19 response. Effective implementation of the CT strategies could seriously limit the spread of the virus, number of new cases, and secondary attack rate and increase early detection of the new cases. The study indicates that despite the measures aimed at improving the COVID-19 management, due to some objective and subjective reasons, there were systematic gaps in the legal documents regulating the CT process. These gaps could seriously affect general efforts to combat COVID-19 in Armenia. The organization of the CT process using IT means also had questionable effectiveness in comparison with the efforts put for its development, practical implementation, and operation.
Still, despite the mass vaccination campaign started worldwide, effective implementation of the CT could add even more value for COVID-19 control, as with the increasing number of immunized population, there is a probability of reducing numbers of the new cases of the novel coronavirus, which creates opportunities for more effective detection of cases and CT.
Considering the abovementioned, several policy recommendations are made to revise and launch CT process. Particularly, needs assessment (human resources, equipment, supplies, and financing) for implementation of the effective CT strategy; development and implementation of the capacity-building plan; deep revision of the existing documents on CT, with special focus on specification of the actions, responsible persons, and control mechanisms; provision of the special trainings to all involved staff; establishment of the effective communication with the community has to be conducted.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work was supported by the Science Committee of RA, in the frames of the research project № 21T-3A090.
Ethics Approval
The study was approved by the Ethics Committee of Yerevan State Medical University and complied with Declaration of Helsinki principles.
Availability of Data and Materials
The data sets used in the current study may be available from the corresponding author on reasonable request.