
Abstract

Introduction
The Medical Aid (MA) program is part of South Korea’s social security system, providing national assistance to low-income households who cannot afford healthcare. 1 They have multiple chronic conditions with high healthcare needs 2 and low perceived health status and health-related quality of life (HRQOL). 3 Although the overarching goal of case management in the MA program is to enhance its beneficiaries’ HRQOL, 1 few studies have identified determinants of HRQOL in community-dwelling MA beneficiaries. Limited social support, unmet healthcare needs, uncontrolled pain, and low health literacy, sense of mastery, and perceived health status are expected to affect community-dwelling MA beneficiaries’ HRQOL. However, no studies have examined direct and indirect pathways among these factors and HRQOL. This cross-sectional study examined the associations between these factors and HRQOL in MA beneficiaries in South Korea, using a hypothesized model based on Predisposing, Reinforcing, and Enabling Constructs in Educational/Environmental Diagnosis and Evaluation (PRECEDE). 4
Methods
Study participants were MA beneficiaries aged over 19 years; we used quota sampling to evenly distribute samples by age, region, and sex. Trained data collectors visited 310 households from December 1 to 17, 2019. The sample included 302 participants who provided written informed consent and completed the survey. The survey consisted of 37 items in 8 domains: HRQOL, health status, pain, health behavior, sense of mastery, unmet healthcare needs, social support, and health literacy for health management. See the Online Appendix for more information about the measures used in this study.
We used path analysis with full information maximum likelihood adjusted for participants’ sex, age, education, marital status, household, and disability status. Model fit was evaluated using the following criteria for acceptable fit: χ2 test with P-value >.05, comparative-fit index (CFI) and Tucker–Lewis index (TLI) ≥0.95, root mean square error of approximation (RMSEA) ≤0.08. 5 The structural relationships among the constructs of the PRECEDE model were evaluated using the magnitude of standardized path coefficients and their significance. All analyses were performed using Stata 15 (StataCorp, College Station, USA). The Institutional Review Board of Inje University (INJE 2019-10-001-001) approved the study.
Results
Sample Characteristics
Among the 302 participants, 152 (50.3%) were male, and 171 (56.6%) were aged 50 years or older. While 68 participants (22.5%) were married, the rest were single (38.7%), divorced (24.5%), or widowed (14.2%); 156 participants (51.7%) lived alone. About half of the participants (49.3%) were at least high-school graduates; the majority (56.3%) were disabled.
Factors Associated With HRQOL
Path analysis revealed that the hypothesized model depicted in Figure 1a had unsatisfying goodness of fit (χ2 = 41.100, df = 13, P < .001, CFI = 0.947, TLI = 0.812, and RMSEA = 0.085). Several modifications were made based on the model indices and theoretical justifications. First, the path from health behavior to pain was insignificant and subsequently removed. Second, a new path from pain to health status was added, improving the model fit. Additionally, marital status and household size, which were adjusted, did not yield any significant paths to the endogenous variables and were subsequently removed. Lastly, a path from social support to health status was added. These modifications yielded the final model, displayed in Figure 1b, providing a good fit to the data (χ2 = 14.252, df = 9, P = .114, CFI = 0.990, TLI = 0.965, and RMSEA = 0.044).
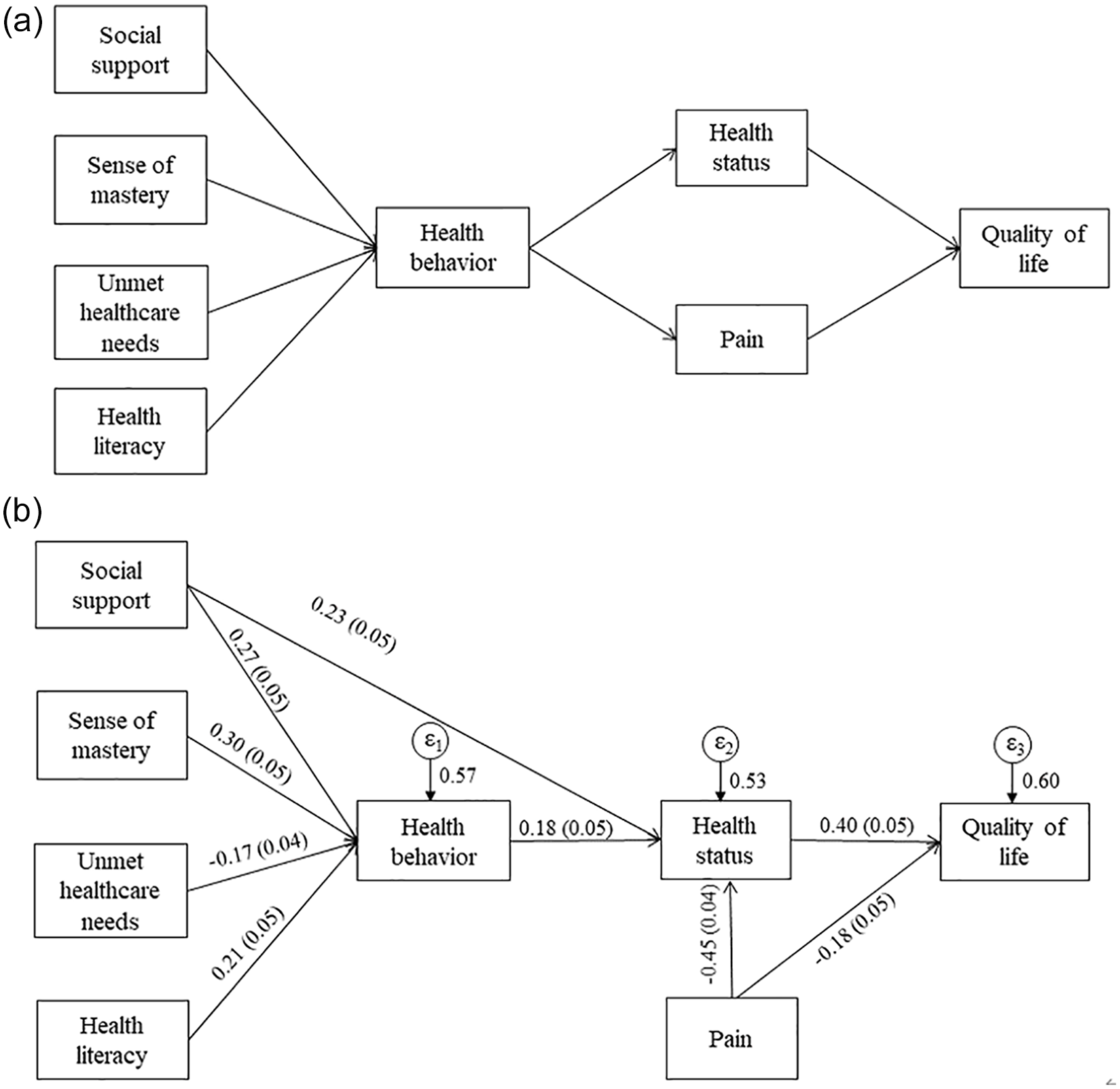
The hypothesized and final models. (a) The hypothesized model. (b) The final model from structural equation modeling. (a) Based on the PRECEDE model, Medical Aid beneficiaries’ sense of mastery and unmet healthcare needs (predisposing factors), social support (a reinforcing factor), and health literacy (an enabling factor) affect their health behaviors which in turn influence their perceived health status and pain. Beneficiaries’ health status and level of pain contribute to their health-related quality of life. (b) Numbers presented on each path are the standardized path coefficients (standard error). The model was adjusted for sex, age, education, and disability status. All exogenous variables were correlated; the correlations are not displayed for better visual presentation.
In the final model, a sense of mastery (β = 0.30, P < .001), health literacy (β = 0.21, P < .001), and social support (β = 0.23, P < .001) were positively associated with health behavior; unmet healthcare needs were negatively associated with health behavior (β = -0.17, P < .001). Health behavior was positively associated with health status (β = 0.18, P < .001), whereas pain did the opposite (β = -0.45, P < .001). Social support was directly associated with health status in addition to the paths through health behavior. Health status (β = 0.40, P < .001) and pain (β = -0.18, P < .001) were associated with HRQOL with opposite directions of effect.
Discussion
The findings suggest that social support, a sense of mastery, unmet healthcare needs, and health literacy are important considerations in implementing MA case management to promote health behavior and improve the health status and HRQOL of community-dwelling MA beneficiaries. Pain was not significantly associated with health behavior; rather, negatively associated with perceived health status and HRQOL. MA beneficiaries with chronic pain reported having pain regardless of their efforts for pain relief, 6 explaining the insignificant association between health behavior and pain in our study. As uncontrolled pain is an important factor associated with low HRQOL, developing effective pain management for these beneficiaries requires societal attention.
Limitations included a cross-sectional design that made it difficult to identify causal relationships between HRQOL and associated factors, the possibility of other potential factors associated with HRQOL, and non-probability sampling procedures that may limit the generalizability of the study findings.
Conclusion
Our findings call for multi-faceted interventions targeting social support, a sense of mastery, unmet healthcare needs, health literacy, and pain to improve the health status and HRQOL of MA beneficiaries. Case managers, healthcare providers, researchers, and other stakeholders should develop and test such interventions and translate the feasible and cost-effective interventions into practice. Furthermore, more advanced case management programs are necessary to coordinate health and social services based on beneficiaries’ unmet needs.
Supplemental Material
sj-docx-1-aph-10.1177_10105395221141783 – Supplemental material for Factors Associated With Health-Related Quality of Life Among Adults With Low Socioeconomic Status and Multiple Healthcare Needs: Using the PRECEDE Model
Supplemental material, sj-docx-1-aph-10.1177_10105395221141783 for Factors Associated With Health-Related Quality of Life Among Adults With Low Socioeconomic Status and Multiple Healthcare Needs: Using the PRECEDE Model by Jeonghyun Cho, Naixue Cui and Hyejin Kim in Asia Pacific Journal of Public Health
Footnotes
Acknowledgements
The authors thank the institution of Gallup Korea for collecting data and the MA beneficiaries who participated in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the National Research Foundation of Korea grant funded by the Korea Government (MSIT; 2017R1C1B1002693).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.