
Abstract

Introduction
The COVID-19 infection, caused by the novel coronavirus, has urged unprecedented global efforts to develop effective vaccines. Of many, an mRNA vaccine, the BNT162b2, targeting the spike protein of the virus, has been at the forefront of vaccination campaigns worldwide. The global COVID-19 vaccine administration approved by the US Food and Drug Administration (FDA) in December 2020 reported a downtrend of COVID-19 cases in 2021 and several hospitalizations and deaths associated with the disease. 1 In view of COVID-19 infection becoming an epidemic, necessitating critical strategies to mitigate disease spread and complications, understanding the nuances of vaccine-induced immunity becomes paramount in public health decision-making. 2 Our study aimed to elucidate the intricate dynamics of neutralizing antibodies (NAb) and S-receptor binding protein (SRBD) antibodies in individuals receiving the BNT162b2 vaccine. By examining antibody titers before and after vaccination and identifying factors influencing antibody levels, the study aimed to provide insights into the mechanisms underlying vaccine-induced immunity.
Our study aimed to determine the factors that may influence the concentrations of the two types of antibodies, neutralizing antibodies (NAb) and SRBD antibodies in individuals receiving the BNT162b2 vaccine. By examining antibody titers before and after vaccination and identifying factors influencing antibody levels, the report of this study hoped to create basic strategies for antibody assay testing to be used routinely in clinical practice.
Methods
The study was prospective in design, consisting of a cohort of 243 volunteered health care workers (HCWs) who received and completed the BNT162b2 vaccine between March and May 2021. After meeting eligibility criteria, participants were recruited from various clinical, laboratory, and administrative units, excluding those with autoimmune disease, malignancy, immunosuppressive, receiving steroids, or chemotherapy, and pregnant or breastfeeding were excused from the study. Data collected included demographic information, comorbidities, and history of COVID-19.
Sample Collections and Analysis
Blood samples were obtained before the vaccination (week 0), 2 weeks after the first dose (week 2), and 2 weeks after the second dose (week 5). A chemiluminescence immunoassay technique was employed to analyze NAb and SARS-CoV-2 spike receptor-binding domain (SRBD) IgG antibodies on the SNIBE Maglumi 800 analyzer.
Statistical Analysis
Statistical analysis was performed using IBM SPSS Statistic version 28, including descriptive analysis, repeated-measure ANOVA, and the correlation analysis to assess changes in antibody titers over time and their associations with demographic factors. A p < .05 [95% CI] was considered statistically significant.
Results
The study observed a significant increase in SRBD antibody titers following BNT162b2 vaccination, underscoring the vaccine’s ability to elicit a robust humoral immune response. Conversely, while NAb levels exhibited a trend of increase post-vaccination, the changes were not statistically significant (Figure 1).
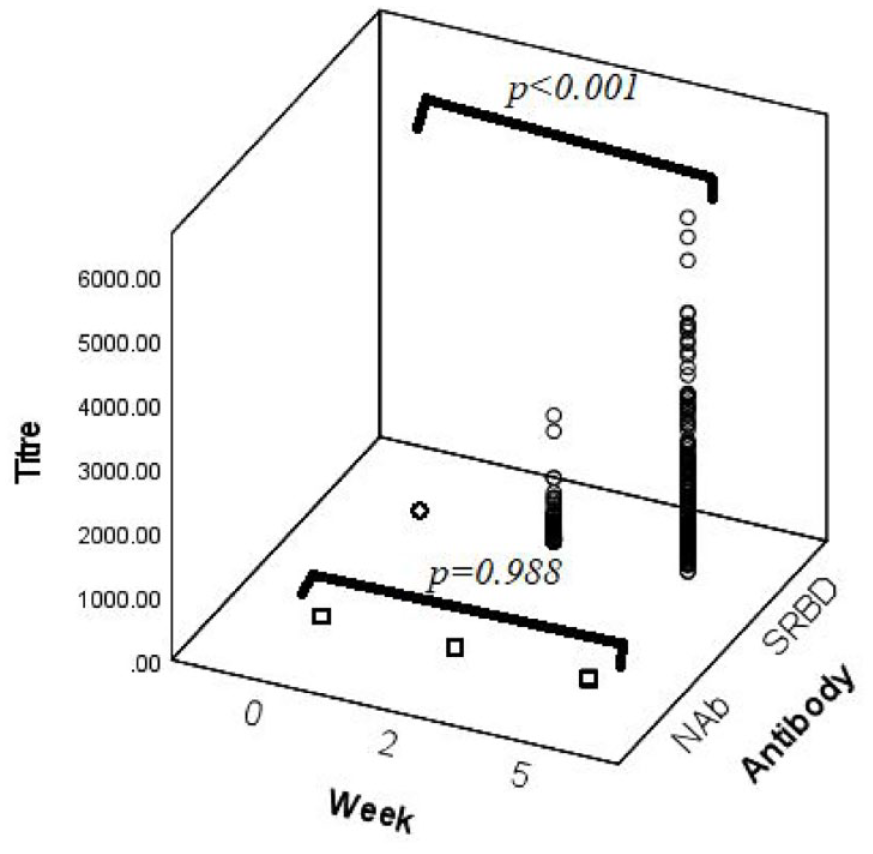
Neutralizing antibody and SRBD antibody titers across the week.
The Factors Affecting NAb and SRBD Antibody Titer
Despite variations in the spike of the titers, neither neutralizing antibody levels nor SRBD antibody levels display substantial correlations with age, gender, race, or comorbidities at any observed time point. These findings suggest that these demographic and health-related variables may not strongly influence the antibody responses measured by neutralizing and SRBD antibodies. While both NAb and SRBD antibody levels show significant differences between individuals with and without a history of COVID-19 at week 2 and week 5, the direction of the effect differs. For NAb, individuals with a history of COVID-19 have significantly higher levels at all time points. At the same time, for SRBD antibodies, significant differences are observed only at week 2 and week 5, with individuals with a history of COVID-19 showing higher levels than those without prior COVID-19 infection (Table 1). Additionally, body mass index (BMI) shows a significant positive correlation with neutralizing antibody levels at week 5, indicating higher BMI associated with higher antibody levels. In contrast, it offers a significant negative correlation with SRBD antibody levels at week 0, indicating higher BMI associated with lower antibody levels at this time point. No significant correlations with BMI were observed for SRBD antibody levels at week 2 and week 5 (Table 1).
Correlation of Neutralizing and SRBD Antibody With Other Parameters.

Pearson’s R correlation, r. bOne-way ANOVA, mean [95% CI]. cMean + SD [95% CI]. dp-value < .05. ep-value < .001.
Discussion
By characterizing the dynamics of NAb and SRBD antibodies, the study contributes to our understanding of the immune mechanisms underlying vaccine-induced protection. However, several critical questions warrant further investigation. Both neutralizing antibody and SRBD antibody levels share some common factors that do not significantly influence their levels. However, there are notable differences in the impact of a history of COVID-19 and BMI on these antibody types across the observed time points.
First, the observed discrepancy between NAb and SRBD antibody kinetics raises questions about the functional relevance of these antibodies in conferring protection against SARS-CoV-2 infection. While SRBD antibodies may play a role in blocking viral entry, the significance of NAb in neutralizing viral particles and preventing infection merits further elucidation. 3 Moreover, the observed correlation between prior infection and enhanced NAb titers post-vaccination highlights the potential alliance between natural and vaccine-induced immunity. This phenomenon of hybrid immunity, wherein previous infection enhances vaccine-induced immune responses, has important implications for understanding and harnessing immune memory in the context of vaccination. 4 However, the precise mechanisms underlying this phenomenon remain unclear.
Second, identifying BMI as a factor influencing antibody levels underscores the importance of considering host factors in vaccine response variability. The observed negative correlation between SRBD antibody titers and BMI suggests potential immunomodulatory effects of adipose tissue on vaccine-induced immune responses. The study in Scotland, involving 3.6 million individuals, reveals that vaccinated individuals with severe obesity face a 76% increased risk of hospitalization or death from COVID-19 compared with those without severe obesity. Additionally, individuals with severe obesity exhibit lower neutralizing antibody titers against SARS-CoV-2, suggesting accelerated waning of vaccine-induced immunity and highlighting the need for tailored vaccination strategies for this population. 5 However, the underlying mechanisms driving this association warrant further investigation, including the role of adipokines and inflammatory mediators in shaping vaccine immunogenicity.
Early evidence suggests that complete vaccination with several certified vaccines effectively prevents COVID-19 infections, ICU admissions, and deaths. 6 The COVID-19 vaccination program in Malaysia initially prioritized groups at the highest risk, such as the aging population and those with chronic illnesses, for booster doses. According to our study, addressing BMI as an additional selective criterion in vaccination strategies and health education can potentially optimize the health economy in navigating the COVID-19 epidemic.
Conclusion
In summary, the study provided valuable insights in refining vaccination strategies, bolstering immune protection, and alleviating the impact of COVID-19 on the economy and global health. Reporting the quantitative antibody titer estimations may help the COVID-19 vaccination policy ensure an adequate hybrid immune response to prevent severe SARS-COV-2 disease. The SRBD antibody is a potential marker for monitoring vaccine response, while the NAb is a potential marker for detecting recent infection. Measuring both NAb and SRBD will be the best approach in a comprehensive assessment of vaccine response.
Footnotes
Acknowledgements
We want to express our gratitude to Shenzen New Industries Biomedical Engineering Co., Ltd. (SNIBE) and Biomarketing Services (BMS) Sdn Bhd, represented by the BMS Project Manager, Madam Pang Lin Sin, and Application Specialists, Ms. Agnes Ng Foong Yi, and Mr. Ben See Choy Yoong, for continuously guiding us throughout the project.
Author Contributions
IAB and HO designed the study. IAB, MZCY, SO, MNAA, and IMM, performed sample method verification, sample analysis and extracting raw data for result analysis in the manuscript. IAB and AMN performed the statistical analysis. IAB prepared the draft. WMAWS, MMM, and HO revised and approved the manuscript for publication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study received in-kind funding and guidance from Shenzen New Industries Biomedical Engineering Co., Ltd. (SNIBE) and Biomarketing Services (BMS) Sdn Bhd.