
Abstract
Predictors for coronavirus disease 2019 (COVID-19)-specific and non-COVID-19-specific deaths have not been extensively studied. This cohort study in Taiwan investigated predictors for COVID-19-specific and non-COVID-19-specific deaths among hospitalized patients with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection. From January to July 2022, 2196 COVID-19 patients at Taipei City Hospital were consecutively recruited in this cohort study. Among the 175 deceased COVID-19 patients, 147 (84.0%) and 28 (16.0%) had COVID-19-specific and non-COVID-19-specific deaths, respectively. After controlling for other covariates, multinomial logistic regressions showed that age ≥ 65 was significantly associated with higher risks for both COVID-19-specific, adjusted odds ratio (AOR) = 6.21; and non-COVID-19-specific deaths (AOR = 6.06). Fully vaccinated individuals (AOR = 0.50) and Paxlovid recipients (AOR = 0.45) had lower COVID-19-specific death risks, while comorbid cancer or end-stage renal disease patients faced higher risks of non-COVID-19-specific deaths. Our study findings suggest that vaccination and Paxlovid treatment are crucial for reducing SARS-CoV-2-specific mortalities, while comorbid patients need careful monitoring to reduce non-COVID-19-specific deaths.
What We Already Know
The coronavirus disease 2019 (COVID-19) pandemic has resulted in over 6.9 million deaths worldwide.
COVID-19 patients requiring hospitalization have higher mortality rates.
Males, presence of cancer, diabetes, end-stage renal disease, and hypertension were associated with a higher mortality risk in patients with COVID-19.
What This Article Adds?
This cohort study is the first to determine the predictors for COVID-19-specific and non-COVID-19-specific deaths.
Among all deceased patients infected with SARS-CoV-2, 84.0% had COVID-19-specific deaths.
Fully vaccinated patients and those receiving Paxlovid treatment had a lower risk of COVID-19-specific death, while comorbid patients with cancer, end-stage renal disease, or chronic obstructive pulmonary disease had a higher risk of non-COVID-19-specific deaths.
Introduction
The coronavirus disease 2019 (COVID-19) pandemic caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) spread globally since its discovery in 2020. 1 As of March 19, 2023, 760.3 million individuals had been infected with SARS-CoV-2, 2 with the death toll reaching 6.9 million. 2 However, the deaths reported to the World Health Organization are very likely underestimated, as many COVID-19-related deaths go unreported. 3
Although 81% of COVID-19 patients experience mild symptoms and have a lower mortality risk,4,5 those requiring hospitalization have higher mortality rates.6 -8 A previous Chinese study reported that the mortality rate in hospitalized patients with COVID-19 was 7.5%. 7 Furthermore, the mortality rate in patients with COVID-19 in the intensive care unit was up to 25.7%. 6
Previous reports showed that males, 9 presence of cancer,10,11 diabetes, 12 end-stage renal disease, 12 and hypertension 12 were associated with a higher mortality risk in patients with COVID-19. However, previous studies defined death as a patient who dies for any reason during treatment.9,10,12 Many patients with COVID-19, however, do not die of COVID-19 but rather of, for example, end-stage renal disease. Nonetheless, few studies on COVID-19 treatment outcomes distinguish COVID-specific mortality from other causes or non-COVID-specific mortality. To our knowledge, only one study determined the factors associated with COVID-19-specific and non-COVID-19-specific deaths in patients infected with SARS-CoV-2. 13 The study included 1283 patients in the United States from March to December 2020 and found that being non-Hispanic black and having a history of chronic health conditions were significantly associated with COVID-19-specific deaths. 13 However, in examining the factors associated with COVID-19-specific and non-COVID-19-specific deaths, the study potentially misclassified confirmed COVID-19-specific deaths due to limited COVID-19 testing available in the early pandemic in 2020. 13
This cohort study aimed to determine the factors associated with mortality to cause-specific death in hospitalized patients with COVID-19 in Taiwan and to inform the clinical management of patients infected with SARS-CoV-2.
Methods
Background Information
All COVID-19 cases in Taiwan must be reported to Taiwan’s Centers for Disease Control within 24 hours after laboratory confirmation. Patients infected with SARS-CoV-2 are required to be admitted to designated COVID-19 hospitals for treatment. 14
The Taipei City Hospital (TCH) is the largest of the designated hospitals in northern Taiwan. Here, patients with COVID-19 are cared for by specialized health care workers.
Study Participants
This cohort study enrolled patients diagnosed with COVID-19 admitted to the TCH between January 1 and July 31, 2022. The COVID-19 diagnoses were confirmed by real-time reverse transcription-polymerase chain reaction (RT-PCR). Patient follow-ups were conducted until discharge from the hospital, death, or August 31, 2022. This study linked the TCH COVID-19 data set to Taiwan’s death certificate database 15 to determine the cause of death of the study participants. In Taiwan, when a patient dies, the law demands that the patient’s death certificate be issued and registered by the physician in charge according to the International Classification of Diseases (ICD) 9 or 10. Trained medical registrars review and code all death certificates at the central office of the National Death Certification Registry. Therefore, the cause-of-death coding in Taiwan has been considered very accurate. 15
This study was approved by the Institutional Review Board of Taipei City Hospital (no. TCHIRB-10904014-E), and the requirement for informed consent was waived. All related procedures were performed in accordance with the relevant national and institutional guidelines and those stipulated in the Declaration of Helsinki.
Outcome Variables
Treatment outcomes were defined as COVID-19-specific and non-COVID-19-specific deaths, as determined by the death certificate database of Taiwan. 15
Covariates
The covariates entered in the core analyses included sociodemographic characteristics, COVID-19 vaccination status, comorbidities, COVID-19 severity, mode of oxygen therapy, and treatment regimens. The sociodemographic characteristics included age and sex. The COVID-19 vaccination status in study subjects was classified into unvaccinated, vaccinated with a single dose, and fully vaccinated (at least two doses of vaccination). Comorbidities included cancer, heart failure, diabetes, end-stage renal disease, and chronic obstructive pulmonary disease, determined based on the patient’s medical records. COVID-19 severity was classified as mild (SARS-CoV-2 infection not requiring supplemental oxygen), moderate (requiring supplemental oxygen but not severe status), and severe (requiring supplemental oxygen and including one of the following conditions: acute respiratory distress syndrome, septic shock, and intensive care unit admission). 14 The mode of oxygen therapy included high-flow nasal oxygen, bilevel positive airway pressure (BiPAP) ventilation, and mechanical ventilation. Treatment regimens for COVID-19 disease included tocilizumab, Paxlovid (nirmatrelvir/ritonavir), molnupiravir, and dexamethasone therapy.
Statistical Analyses
The demographic data of the study participants were analyzed. Continuous data are presented as mean (standard deviation [SD]), and one-way analysis of variance was used for intergroup comparisons. Categorical data were analyzed using Pearson’s χ2 test, as appropriate.
The crude association between patient characteristics and mortality was assessed by odds ratios (ORs) and the corresponding 95% confidence intervals (CIs). We then used multivariate analysis to identify the factors associated with mortality among patients with COVID-19 after adjusting for demographics, comorbidities, COVID-19 severity, mode of oxygen therapy, and treatment regimens. Furthermore, we used a multinomial logistic regression analysis to identify the factors associated with COVID-19-specific and non-COVID-19-specific deaths among patients infected with SARS-CoV-2. Adjusted ORs (AORs) with 95% CIs indicate the strength and direction of the association. All data management and analyses were performed using SAS 9.4 software (SAS Institute, Cary, NC, USA).
Results
Participant Selection
From January 1 through July 31, 2022, a total of 2518 SARS-CoV-2 infected patients admitted to the TCH were included in this cohort study. After excluding those aged <18 years (n = 322), the remaining 2196 patients were included in the analysis (Supplementary Figure 1). The overall mean (SD) age was 62.3 (22.9) years, 53.8% of the patients were men, and 8.0% died during hospitalization. Among the 175 deceased COVID-19 patients, 147 (84.0%) and 28 (16.0%) had COVID-19-specific and non-COVID-19-specific deaths, respectively.
Patients’ Characteristics According to Treatment Outcomes
Table 1 presents patient characteristics based on treatment outcomes. Compared to successfully treated patients, those with COVID-19-specific or non-COVID-19-specific deaths were older and had a higher proportion of comorbidities. Additionally, patients with COVID-19-specific and non-COVID-19-specific deaths were less likely to be fully vaccinated compared to those successfully treated. Regarding oxygen treatment, more patients with COVID-19-specific or non-COVID-19-specific deaths received oxygen treatment, including high-flow nasal oxygen, BiPAP, and mechanical ventilation. Patients with COVID-19-specific deaths had a higher proportion of receiving tocilizumab and dexamethasone treatment.
Patients’ Characteristics According to Treatment Outcome.
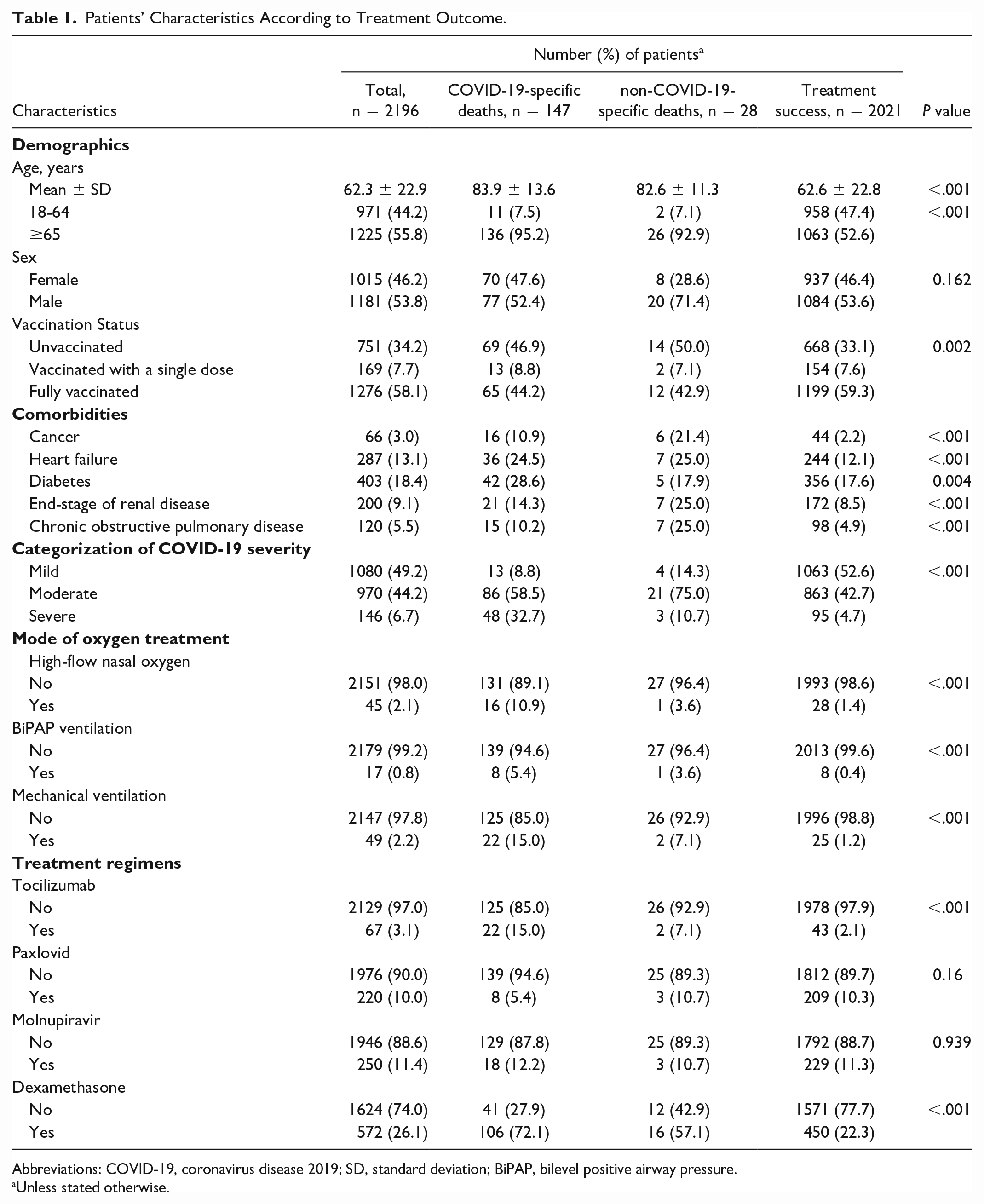
Abbreviations: COVID-19, coronavirus disease 2019; SD, standard deviation; BiPAP, bilevel positive airway pressure.
Unless stated otherwise.
Factors Related to Mortality in Patients With COVID-19
The univariate and multivariate analyses of factors associated with mortality in patients with COVID-19 are shown in Table 2. After adjusting for demographics, comorbidities, COVID-19 severity, mode of oxygen treatment, and treatment regimens, risk factors for mortality included age ≥65 years (AOR = 6.26; 95% CI [3.32, 11.79]), cancer (AOR = 5.10; 95% CI [2.75, 9.49]), moderate (AOR = 2.89; 95% CI [1.63, 5.13]) and severe COVID-19 infection (AOR = 6.05; 95% CI [2.86, 12.81]) (mild COVID-19 infection: reference), mechanical ventilation (AOR = 3.91; 95% CI [1.78, 8.59]), and receiving dexamethasone treatment (AOR = 2.64; 95% CI [1.78, 3.93]). Protective factors for mortality include being fully vaccinated (AOR = 0.49; 95% CI [0.34, 0.71]) and receiving Paxlovid treatment (AOR = 0.50; 95% CI [0.25, 1.00]).
Factors Associated With Mortality Among Patients With COVID-19 Requiring Supplemental Oxygen Therapy Based on Univariate and Multivariate Analyses.

<.05; ***<.001.
Abbreviations: COVID-19, coronavirus disease 2019; AOR, adjusted odds ratio; CI, confident interval; BiPAP, bilevel positive airway pressure.
Factors Associated With COVID-19-Specific and Non-COVID-19-Specific Mortality
We used multinomial logistic regression analysis to determine the risk factors associated with COVID-19-specific and non-COVID-19-specific mortality in infected patients. After adjusting for other covariates, age ≥65 years was associated with a higher risk of COVID-19-specific (AOR = 6.21; 95% CI [3.12, 12.35]) and non-COVID-19-specific deaths (AOR = 6.06; 95% CI [1.34, 27.34]) (Table 3). Regarding vaccination and treatment regimens, fully vaccinated patients (AOR = 0.50; 95% CI [0.33, 0.74]) and those receiving Paxlovid treatment (AOR = 0.45; 95% CI [0.20, 0.98]) had a lower risk of COVID-19-specific death. Furthermore, comorbid patients with cancer (AOR = 9.91; 95% CI [3.51, 27.98]), end-stage renal disease (AOR = 3.05; 95% CI [1.10, 8.41]), or chronic obstructive pulmonary disease (AOR = 2.94; 95% CI [1.08, 8.00]) had a higher risk of non-COVID-19-specific deaths during the hospitalization.
Multinomial Regression Analysis of Risk Factors of COVID-19-Specific and Non-COVID-19-Specific Deaths.
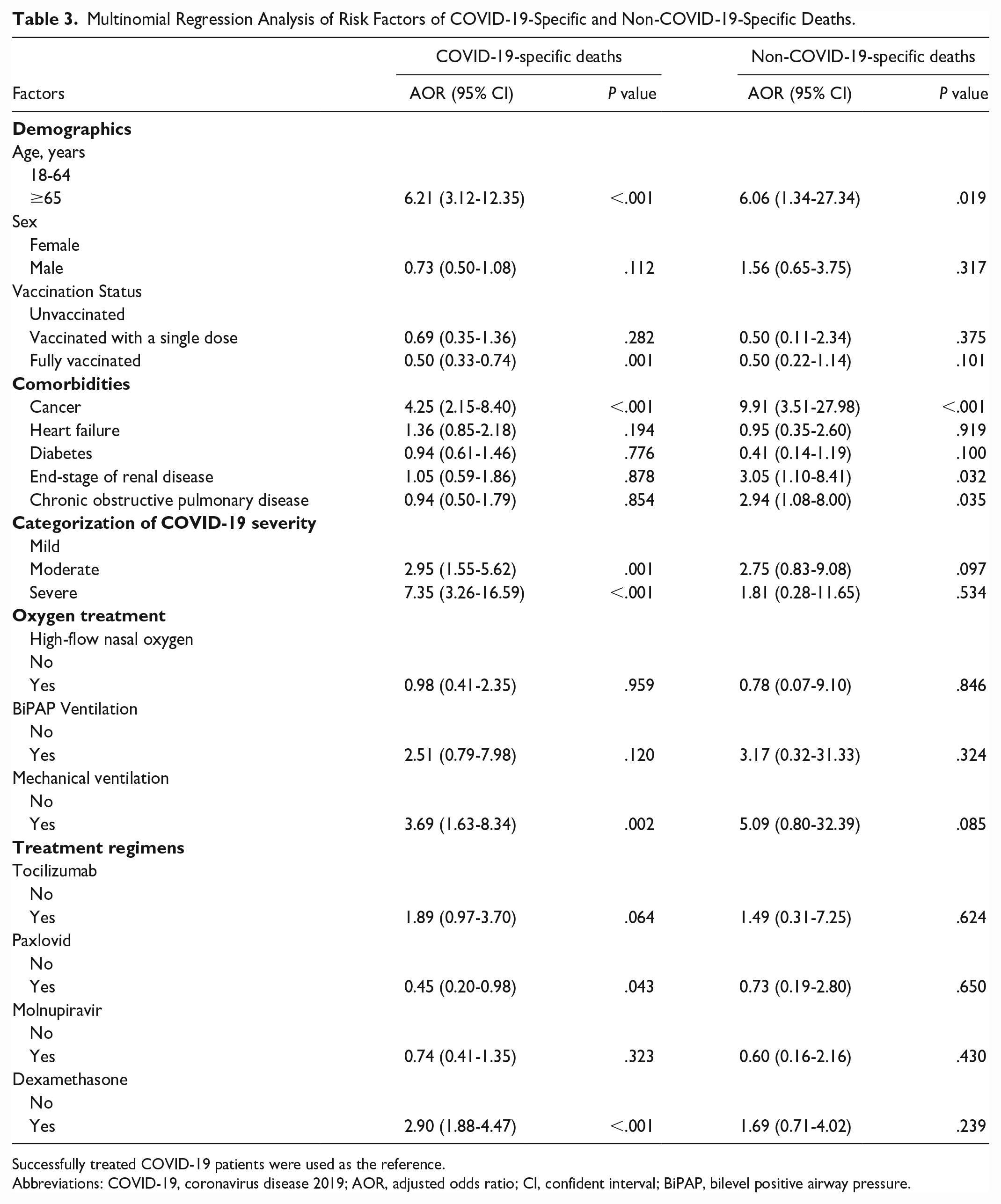
Successfully treated COVID-19 patients were used as the reference.
Abbreviations: COVID-19, coronavirus disease 2019; AOR, adjusted odds ratio; CI, confident interval; BiPAP, bilevel positive airway pressure.
Discussion
This cohort study found that the mortality rate was 8.0% among hospitalized COVID-19 patients. Of all deceased patients, 147 (84.0%) had COVID-19-specific deaths. After controlling for demographics, comorbidities, COVID-19 severity, and treatment regimens, age ≥65 years was associated with a higher risk of COVID-19-specific and non-COVID-19-specific deaths. Fully vaccinated patients and those receiving Paxlovid treatment had a lower risk of COVID-19-specific deaths, while comorbid patients with cancer, end-stage renal disease, or chronic obstructive pulmonary disease had a higher risk of non-COVID-19-specific deaths.
The mortality rate in this study was 8.0% among hospitalized COVID-19 patients, similar to 7.5% among hospitalized patients with COVID-19 in China. 7 Despite most COVID-19 patients did not require hospitalization because of mild symptoms and low mortality rate, 4 the death risk in hospitalized patients infected with SARS-CoV-2 was high. 7 Our findings suggest that hospitalized patients infected with SARS-CoV-2 require close monitoring and careful treatment during hospitalization.
This study showed that age ≥ 65 years was associated with a higher risk of COVID-19-specific and non-COVID-19-specific deaths. The age-associated decline of adaptive immunity against SARS-CoV-2 may account for the high death rate in older patients with COVID-19. A prior study found that aging was associated with defects in B- and T-cell immunity, which could inhibit the control of viral replication and increase mortality rates in patients with COVID-19. 16 Another study found that older rhesus monkey with SARS-CoV infection had stronger innate immune responses to infection than those of younger adults, which caused an increase in the differential expression of genes related to inflammation and severe illness. 17 Our findings suggest that older adults should be prioritized when implementing preventive measures.
We found that complete vaccination decreased the risk of COVID-19-specific mortality by 50%. Vaccines are the most important strategy for preventing SARS-CoV-2 infection. 18 Moreover, COVID-19 vaccines can elicit immune responses and induce the production of neutralizing antibodies, 19 which could reduce infection severity and mortality rates. In our cohort, 34.1% of COVID-19 patients were unvaccinated, which accounted for 69 (46.9%) COVID-19-specific deaths. With the higher mortality risk in unvaccinated patients, our findings suggest that vaccination is imperative in reducing COVID-19-specific mortalities.
Our findings revealed that using Paxlovid reduced the risk of COVID-19-specific mortality by 55%. Paxlovid is a SARS-CoV-2 protease inhibitor, 20 which could reduce viral replication and illness severity. A randomized control trial showed that using Paxlovid within 3 days of symptom onset could significantly reduce the risk of hospitalization by 89% in patients at risk of serious COVID-19 illness. 21 Our study findings suggest that the use of the Paxlovid regimen is important in reducing COVID-19-specific mortality, particularly for those aged ≥ 65 years and those with serious comorbidities.
To our knowledge, this cohort study is the first to determine the predictors for COVID-19-specific and non-COVID-19-specific deaths. Our study found that, of all deceased patients infected with SARS-CoV-2, 84.0% had COVID-19-specific deaths. Nevertheless, this study had several limitations. First, there might be important factors (e.g., obesity) associated with patient mortality that were not collected in this study. Second, since all study participants were Taiwanese, the generalizability of our findings might be limited and requires further verification in future studies of other non-Asian patient populations.
Conclusion
This cohort study found that, among all deceased patients infected with SARS-CoV-2, 84.0% were COVID-19-specific deaths. After controlling for demographics, comorbidities, COVID-19 severity, and treatment regimens, fully vaccinated patients and those receiving Paxlovid treatment had a lower risk of COVID-19-specific death, while comorbid patients with cancer, end-stage renal disease, or chronic obstructive pulmonary disease had a higher risk of non-COVID-19-specific deaths. Our findings suggest that COVID-19 vaccination and Paxlovid treatment are imperative to reduce SARS-CoV-2-specific mortality. Furthermore, comorbid patients with COVID-19 require close monitoring and careful treatment during hospitalization to reduce non-COVID-19-specific mortalities.
Supplemental Material
sj-doc-1-aph-10.1177_10105395241282634 – Supplemental material for Predictors for COVID-19-Specific and Non-COVID-19-Specific Deaths: A Cohort Study in Taiwan
Supplemental material, sj-doc-1-aph-10.1177_10105395241282634 for Predictors for COVID-19-Specific and Non-COVID-19-Specific Deaths: A Cohort Study in Taiwan by Shang-Yih Chan, Hsin-Hao Lai, Yun-Ju Lai, Chao-Ming Huang, Chu-Chieh Chen, Shen-Shong Chang, Yung-Feng Yen and Yi-Chun Chiu in Asia Pacific Journal of Public Health
Footnotes
Acknowledgements
The authors are grateful to the members of the Research Office for Health Data, Department of Education and Research, Taipei City Hospital, Taiwan for their valuable contributions in data management and statistical analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the grants from Department of Health, Taipei City Government, Taiwan (No. 11101-62-042; No. 11201-62-023; No. 11301-62-007). The funders had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.