
Abstract
Leptospirosis and enteric fever are prevalent tropical acute bacterial febrile illnesses in Kelantan, Malaysia, that exhibit overlapping features and shared transmission dynamics, yet their spatial relationship remains understudied. This study aimed to analyze their spatial distribution, investigating potential interactions and intersecting patterns. A total of 212 laboratory-confirmed cases of enteric fever and 1106 of leptospirosis between 2016 and 2022, were retrieved from the national e-Notifikasi registry. Point pattern analysis revealed clustering of both diseases in the northern region, but leptospirosis was predominant in the south, exhibiting higher spatial risk. Seven co-infection cases were identified in overlapping hotspot areas. Spatial dependence between the diseases was identified within 4 km distance on average, with varying patterns over time and regions. Recognizing spatial dependence has implications for accurate diagnosis, timely intervention, and tailored public health strategies. The findings underscore the need for multi-disease interventions to address shared risk factors and co-infections in similar geographical contexts.
What We Already Know
Leptospirosis and enteric fever are common causes of acute febrile illness in tropical regions, including Kelantan, Malaysia.
Misdiagnosis is prevalent for both diseases due to limited rapid diagnostic tests.
Despite sharing risk factors and transmission dynamics, there is a lack of understanding regarding the spatial relationship between leptospirosis and enteric fever in Kelantan.
What This Article Adds
The study provides a comprehensive analysis of the spatial distribution of laboratory-confirmed cases of leptospirosis and enteric fever in Kelantan over the period 2016-2022.
The research uncovers significant spatial clustering and interactions between the two diseases, shedding light on their dynamic patterns over time and across regions.
The identification of distinct clusters and the observed spatial interdependence between leptospirosis and enteric fever contributes crucial information for developing targeted and effective disease control and prevention strategies.
Introduction
Leptospirosis and enteric fever are commonly reported as bacterial causes of acute undifferentiated febrile illness in tropical and subtropical regions.1,2 Leptospirosis is a neglected zoonotic disease caused by pathogenic Leptospira interrogans spirochaetes of the genus Leptospira often observed in tropical countries, with epidemic potentials that are often precipitated by disasters or extreme weather. 3 Bacterial transmission to humans occurs through direct contact with infected animal urine, reproductive fluid, blood, or tissue, or, more frequently, through exposure to a contaminated environment including consumption of contaminated food or water. 4 Over 1.03 million leptospirosis cases and 58, 900 deaths are reported worldwide yearly with a case-fatality ratio of 6.9%. 3
Enteric fever refers to both typhoid and paratyphoid fever that is caused by Salmonella enterica serovar typhi (S. typhi) and paratyphi (S. paratyphi). 5 Enteric fever is contracted by ingesting water or food contaminated with the feces of an acutely infected or convalescent individual, or a person with chronic, asymptomatic carriage within the immediate environment. 5 The global incidence rate of enteric fever was estimated to be 197.8 (95% CI: 172.0, 226.2) and highest in Southeast Asia at 219.8 (95% CI: 192.9, 249.1) per 100,000 person-years in 2017 with over 14.3 million cases were reported throughout that year. 6 In Southeast Asia, leptospirosis was the primary cause of undifferentiated fever among outpatients with a prevalence of 12.1%, while enteric fever was estimated to have an overall prevalence of around 4%. 1
Infectious diseases often exhibit distinct patterns when observed at a local level. 7 The distribution of enteric fever and leptospirosis greatly varies depending on the geographical location affected by various factors, and some of these may overlap between these two diseases.8,9 Common factors that favor the transmission of enteric fever and leptospirosis include rapid urbanization, high population density and household size leading to crowding, poor water and sanitation initiatives, food and water contamination, living near water bodies like lakes and rivers, along with climate changes, heavy rainfall, natural disasters such as flood and drought, as well as hot and humid weather.10,11 Despite the implementation of various public health measures, enteric fever and leptospirosis remain endemic, highlighting the ongoing challenges in controlling and preventing these diseases in Kelantan.11,12
Comparing the spatial pattern of enteric fever to leptospirosis can reveal the common underlying factors that contribute to the spread of the diseases as well as identify the potential interactions or co-infections between the diseases. This study aimed to characterize the spatial distribution and to examine the spatial variations between enteric fever and leptospirosis that can provide valuable information in understanding the epidemiology and transmission dynamics of these diseases, which can guide public health strategies for disease prevention and control.
Methods
Study Area
This was a retrospective cohort study conducted in Kelantan, Malaysia, covering all 10 districts and 66 subdistricts. Kelantan, situated in northeastern Malaysia, is bordered by Thailand to the north and the South China Sea coastline to the east. The average population density in this state is 119 people per square kilometer, with an average household of 4.9, making it the highest in Malaysia. 13 Approximately 44.1% of the population resides in urban areas. 14 Kelantan had the lowest coverage of pipe water supply at home in Malaysia at 67.8% leading their citizens to resort to other sources of untreated water mainly dug and tube well water, gravitational feed water system, and river water.13,15
Data Source and Variables
The National Communicable Disease Control Information System (CDCIS) e-Notifikasi infectious disease registry was utilized to extract laboratory-confirmed cases of enteric fever and leptospirosis registered with the Kelantan State Health Department. This registry is part of Malaysia’s online passive surveillance system for mandatory notifiable diseases that include both diseases. Symptomatic cases of enteric fever that had Salmonella typhi or paratyphi isolated from blood, stool, or other clinical specimens were considered to be laboratory-confirmed cases. 16 Confirmed leptospirosis cases are the symptomatic cases that were laboratory confirmed with any one of the following—microscopic Agglutination Test (MAT) for single serum specimen—titer ≥ 1:400 while for paired sera—four-fold or greater rise in titer; positive polymerase chain reaction (PCR) or positive culture for pathogenic Leptospira; or demonstration of Leptospira in tissues using immunohistochemical staining (e.g. in post-mortem cases). 16 The cases’ coordinates were obtained using a handheld GPS device and recorded in the e-Notifikasi system in the WGS84 coordinate reference system (CRS). Each registered case in the database was assigned a spatial point, and additional information such as age, gender, date of onset and notification, case classification, and laboratory results was included. The study excluded those residing outside the state or located beyond its boundaries. The mid-year population data for all subdistricts in Kelantan from 2016 to 2022 according to gender that was projected based on the 2010 and 2022 censuses were obtained from the Department of Statistics Malaysia (DOSM). Geospatial population data were retrieved as a shapefile projected using the Kertau Rectified Skewed Orthomorphic (RSO) Malaya meter (m) CRS that served as the base map for disease mapping.
Statistical Analysis
Cases were characterized using descriptive statistics. Categorical data were summarized as frequency counts and percentages. Points are marked with factors with each point representing a category of diagnosis—either enteric fever or leptospirosis, and the spatial interaction between the diseases was assessed using multitype point pattern analysis. Kernel density estimation (KDE) was applied using the spatstat package to estimate the probability density function (PDF) of each disease. 17 KDE is a non-parametric method that smooths observed data points to estimate density. 18 To assess the spatial relationship between two diseases using KDE, we compared high-density areas for each disease to identify regions with similar or differing concentrations, revealing patterns of spatial overlap or segregation. Exploratory analysis including likelihood cross-validation, Cronie and van Lieshout’s criterion, Scott’s rule of thumb, and sigma at 5, 10, and 20 km, was performed to select appropriate bandwidth.18 -20 Spatial clustering for each disease was also assessed by the average nearest neighbor (ANN) distance analysis and nearest neighbor index (NNI) from the spatialEco package. 21 The NNI is expressed as the ratio of the observed distance divided by the expected distance; an index less than 1 indicates clustering and greater than 1 suggests dispersion. 21 Multitype point pattern analyses included multitype nearest neighbor distributions function Gij, multitype Ripleys’s cross K-function Kij (r), and L-function Lij (r) which are the bivariate extensions of Gest(), Kest(), and Lest() function from the spatstat package. 17 The bivariate Ripley’s K-function counted the number of neighboring leptospirosis cases found within a given distance of each case of enteric fever while the bivariate L-function quantifies the expected number of points of one type within a distance r of each point of the other type, adjusted for the intensity of the two-point processes. 22 These functions assessed the spatial relationship between two event points under the null hypothesis of spatial independence. 17 If the functions show values significantly above the expected levels measured under the assumption of a Poisson process, it indicates clustering of one type of point around the other, reflecting a positive spatial association between the two-point processes. 17 Monte Carlo simulations were used to generate confidence envelopes for the observed functions. Any observed value exceeding the upper bound of the envelope suggests significant clustering of one disease relative to the other. 17 We estimated the spatially varying probability of a case being leptospirosis versus enteric fever using kernel smoothing (Kelsall and Diggle method) from the spatstat package, with resulting maps highlighting regions of varying probabilities for leptospirosis compared with enteric fever. 17
Ethical Approval
This study adhered to the Helsinki Declaration and Malaysia Good Clinical Practice guidelines. Ethical approval was granted by the Human Research and Ethics Committee, Universiti Sains Malaysia (JEPeM) under ID USM/JEPeM/22110718. The study was registered with the National Medical Research Register (NMRR ID-22-02749-XAA) and received additional approval from the National Institute of Health’s Medical Review and Ethical Committee (MREC).
Results
A total of 212 enteric fever cases (typhoid = 205, paratyphoid A =1, paratyphoid B=5, paratyphoid C=1) and 1106 leptospirosis cases that were laboratory confirmed and notified to the e-Notifikasi online system between 2016 and 2022 were included in the analysis. Enteric fever and leptospirosis exhibit differences in age distribution, with enteric fever affecting the younger population (Supplementary Table 1). Leptospirosis consistently had a higher number of cases and incidence compared with enteric fever throughout the years, but the trends were similar to enteric fever (Supplementary Figure 1). Both diseases have generally been on a decreasing trend over the years, with some fluctuations in the year 2018 and notable increments in the year 2022.
Enteric fever cases were spread across 53 subdistricts between 2016 and 2022, whereas all 66 subdistricts have reported at least one laboratory-confirmed case of leptospirosis between 2016 and 2022 (Supplementary Figure 2). The cases were similarly distributed in the northern region for both diseases; however, leptospirosis cases were relatively more prominent in the southern region, especially in the subdistricts of Gua Musang and Kuala Krai districts. Overall, enteric fever exhibited a more consistent spread across the northern region over the years, while leptospirosis shows more variability in its geographical distribution with a significant increase in cases of both diseases in 2022.
Nearest Neighbor Distance Analysis
Enteric fever cases were clustered from 2016 to 2019, with NNI values <1 (Supplementary Table 2), though ANN distances gradually increased. During the COVID-19 pandemic (2020-2021), cases became significantly dispersed but clustered again in 2022 with a shorter ANN distance (3.567 km). Leptospirosis cases showed significant clustering with varying intensities, except during the pandemic (2020-2021), when NNI values approached 1, indicating dispersion (P = .597). The highest clustering occurred in 2016, with the lowest NNI (0.597) and the most negative Z score (–14.632). Overall, leptospirosis demonstrated greater clustering than enteric fever, as evidenced by lower ANN values and more negative Z scores.
Hotspot Analysis Using KDE
Figure 1 depicts KDE hotspot maps for enteric fever and leptospirosis based on automated bandwidths. The distribution of hotspots for leptospirosis is more localized and shows greater year-to-year variation compared with enteric fever, which has a more consistent and widespread pattern of hotspots, particularly in the northern region. During earlier years, areas in the northern region exhibited significantly higher KDE values. However, more hotspots were emerging toward the southeastern and southern regions in recent years. The study identified overlapping hotspots of enteric fever and leptospirosis particularly in northern areas, including seven cases of co-infection mostly originating from these areas (Figure 1). We analyzed disease incidence and population density at the subdistrict level to account for population effect. Bivariate Lee’s L tests found no significant correlation, and KDE identified disease hotspots independent of population density.
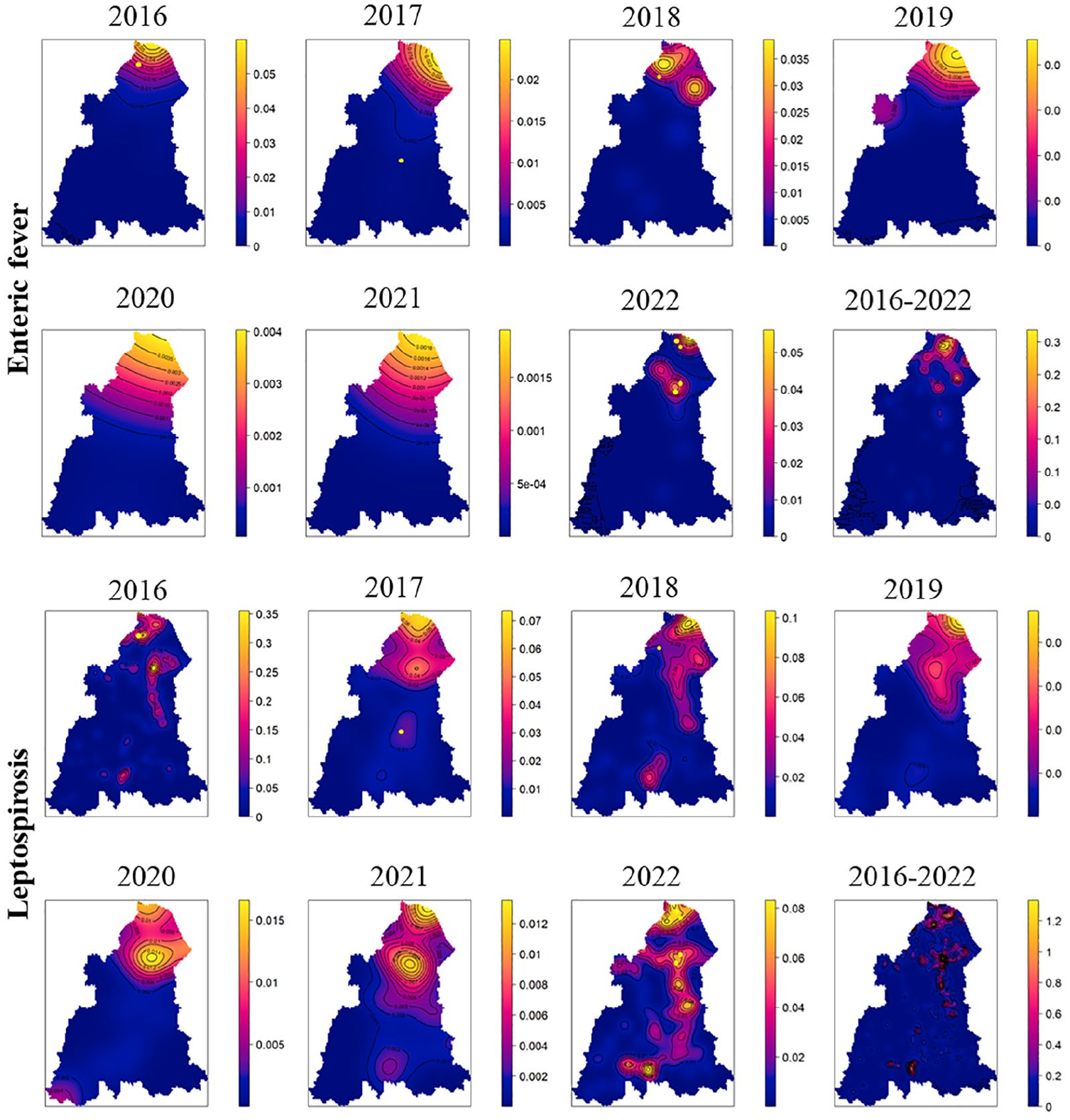
Kernel density estimation (KDE) heatmaps of enteric fever and leptospirosis cases in Kelantan using likelihood cross-validation bandwidth selection, 2016-2022. The heatmaps reveal overlapping areas of high density for both diseases, indicating regions with spatial convergence and potential co-occurrence of cases. Seven cases of co-infection were identified from the area of higher density of cases denoted by yellow dots; one case in the years 2016, 2017, and 2018, respectively, and four cases in 2022.
Multitype (Bivariate) Point Pattern Analysis
Multitype point pattern analyses using distance-based methods were applied to analyze the spatial interactions between enteric fever and leptospirosis cases. The bivariate K and L-function denoted that the empirical values
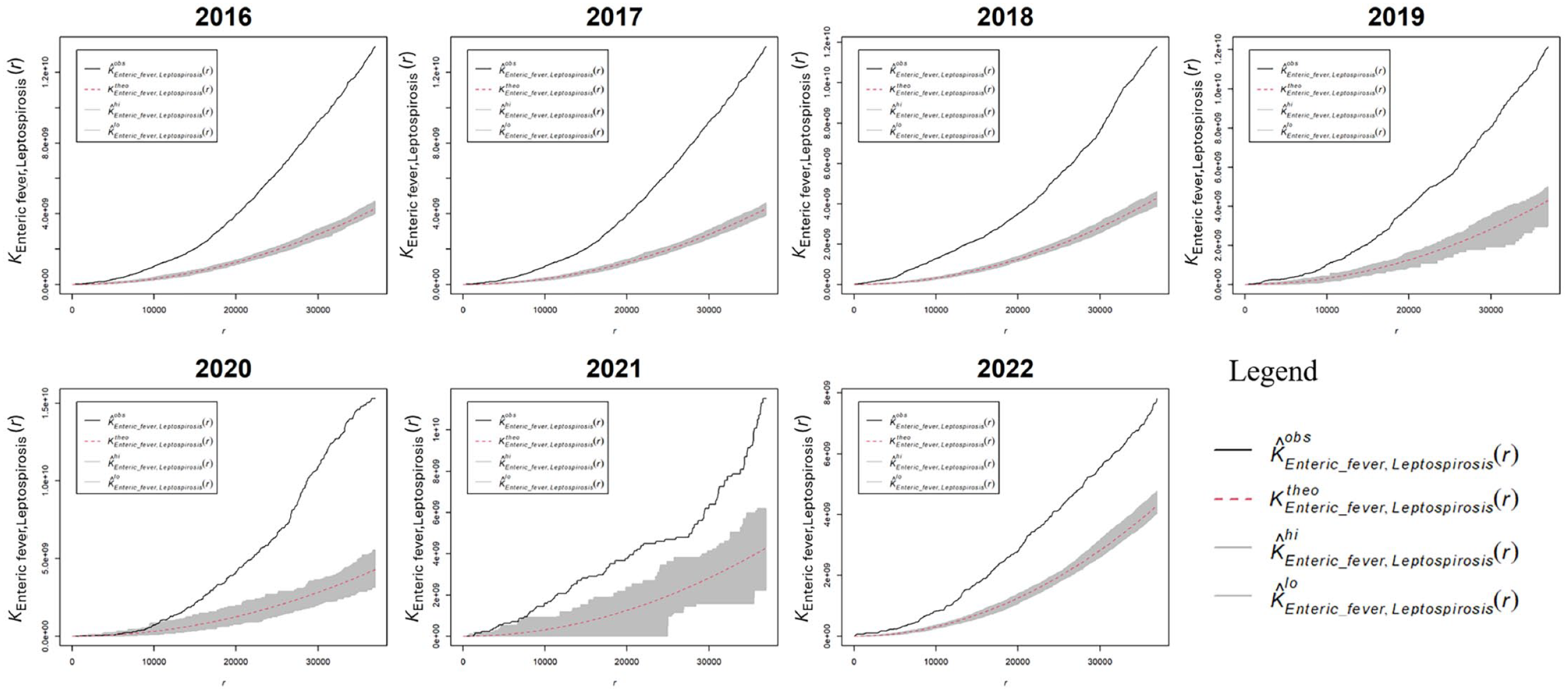
Bivariate Ripley’s K-function for enteric fever and leptospirosis cases in Kelantan, 2016-2022, observed
Bivariate Gij function analysis demonstrated consistent deviations of empirical above theoretical values within 2-10 km (average 4 km) distance for cases between 2016 and 2022 (Supplementary Figure 4). The observed clustering indicated that cases of these diseases are spatially dependent and tend to occur close to each other.
Spatially-Varying Probability
We estimated the spatially varying probability of a case being leptospirosis relative to enteric fever. Between 2016-2018, the probabilities of leptospirosis were relatively higher than enteric fever in most of the southern and central areas of the state but similar or lower in some northern regions especially over the earlier period (Figure 3). In 2019, there was an unusually high probability of enteric fever in the western region. From 2020 to 2022, the high-probability areas again primarily appeared in the southern regions, although with a smoother transition between high and low probabilities compared with earlier years.
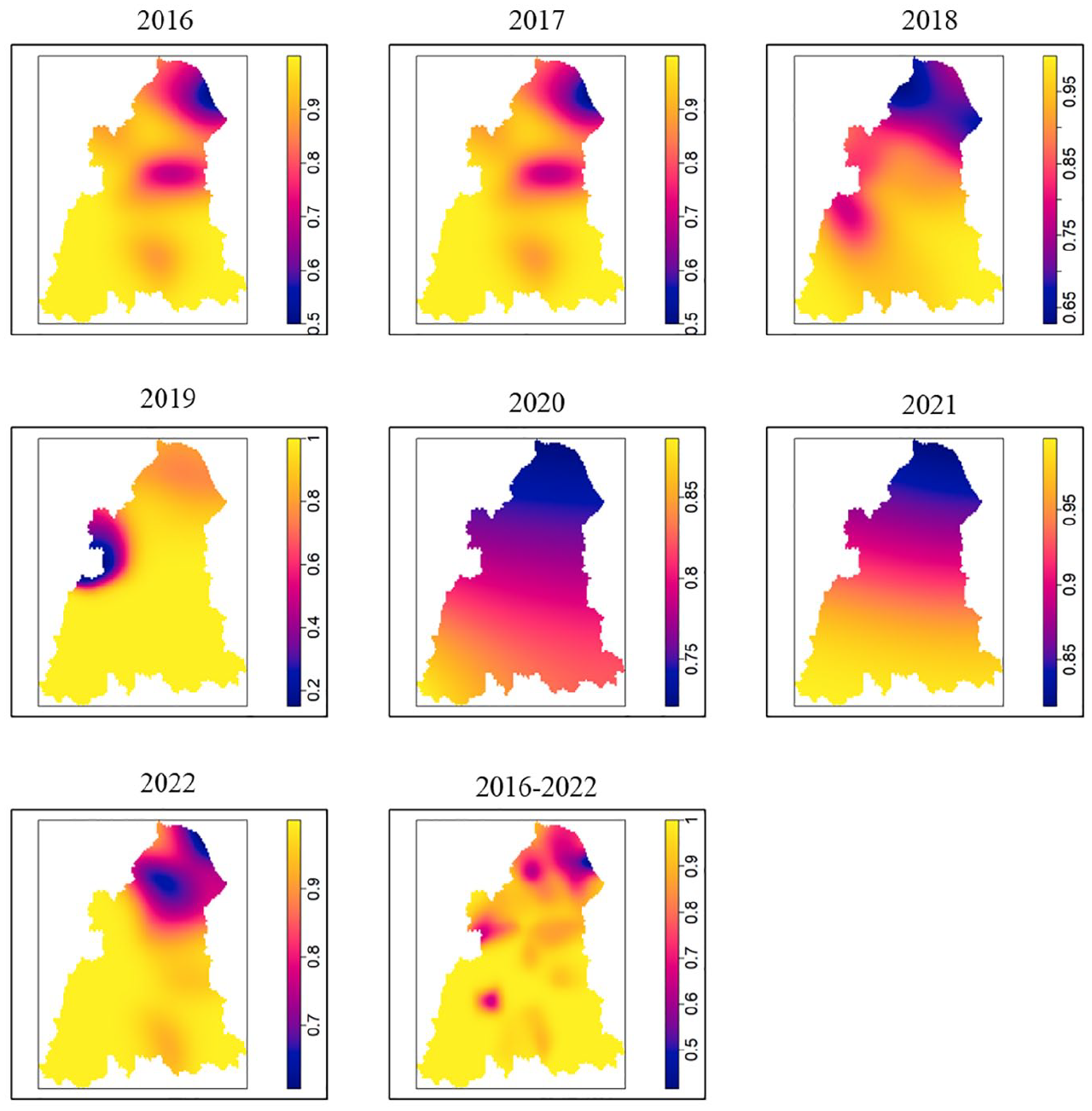
Spatially varying probability of being a leptospirosis case compared with enteric fever case at a given area in Kelantan, 2016-2022. Lighter shades indicate higher probabilities of leptospirosis relative to enteric fever.
Discussion
Our study indicates a spatial dependence between leptospirosis and enteric fever, suggesting that the occurrence of these diseases is not random but instead influenced by shared environmental and socioeconomic factors. While there is limited research directly exploring the spatial relationship between leptospirosis and enteric fever, existing literature and evidence enable us to infer several common risk factors that likely contribute to the spatial dependence and transmission of both diseases. Despite the difference in transmission routes—enteric fever primarily via the fecal-oral route and leptospirosis through animal reservoirs—their spatial dynamics suggest interconnected transmission influenced by various factors. These include rapid urbanization, high population density, large household sizes leading to crowded living conditions, inadequate water, sanitation, and hygiene (WASH), contamination of food and water sources, residing close to water bodies such as lakes and rivers, as well as climate changes such as heavy rainfall, natural disasters like floods and droughts, and tropical weather.10,11 Overlapping spatial patterns of poverty, infrastructure deficiencies, and population density may also create environments conducive to the transmission of both enteric fever and leptospirosis. Hence, regions vulnerable to one infectious disease may also face risks of outbreaks and transmission of other diseases. Recognizing these interconnected transmission dynamics emphasizes the necessity for targeted strategies that address shared environmental and socioeconomic factors contributing to both diseases. This understanding enables more efficient resource allocation, directing efforts and resources to regions with a higher likelihood of co-endemicity. Moreover, identifying shared risk factors facilitates the implementation of preventive measures that can simultaneously mitigate the transmission of both diseases which would be much more effective and efficient compared with carrying separate strategies for each disease. Implementing integrated education and awareness programs to address the co-occurrence of enteric fever and leptospirosis, particularly in high-risk zones offers advantages in efficiency, resource optimization, community engagement, and adaptability compared with separate disease-focused strategies, aligning with a holistic approach to public health.
The simultaneous occurrence of enteric fever and leptospirosis poses diagnostic challenges due to their similar symptoms, which can lead to misdiagnosis and delayed intervention. Our study underscores the need to consider co-infection in endemic areas, as it complicates treatment and heightens the risk of severe complications.23,24 Developing a diagnostic algorithm tailored to these co-endemic conditions can aid in differentiating between the two diseases. This algorithm should account for shared symptoms and risk factors. Additionally, risk zoning strategies could help identify regions with high co-occurrence, guiding targeted diagnostics and resource allocation. In Kelantan, rapid point-of-care testing for leptospirosis was limited to tertiary centers, and rapid tests for enteric fever were not routinely available. Given the remote populations in the southern and southeastern regions, public health officials should expand rapid testing to primary care facilities and endemic areas for timely diagnosis. As the incidence of these diseases rises, health systems may struggle with the dual burden, impacting surveillance, diagnosis, and treatment. Efficient and accurate diagnosis is essential for promptly distinguishing between the two diseases and initiating appropriate treatment. The co-occurrence of enteric fever and leptospirosis also strains health systems, highlighting the need to improve diagnostic capabilities, surveillance infrastructure, and treatment protocols. The existing surveillance systems should be enhanced to be adaptable, and capable of monitoring both diseases concurrently, integrating data collection methods that capture their overlap. Expanding the role of spatial analysis to be actively included in disease surveillance would allow for the prediction and modeling of not only the disease pattern and trend but also for other diseases with similar risk, improving the early warning, alert, and response (EWAR) system. This will support stakeholders and policymakers in making informed decisions on resource allocation, infrastructure, and emergency response based on regional needs.
In our study, we employed a combination of KDE, multitype point pattern analysis, and spatial clustering technique at a finer scale of subdistrict level compared with aggregated data in administrative boundaries, offering a more detailed insight into hotspot identification, and spatial patterns for enteric fever and leptospirosis, although KDE’s bandwidth sensitivity and the complexity of multitype functions can be limitations. The bivariate functions assess interactions between different point types, testing the null hypothesis of spatial independence that is useful for understanding how one disease affects the spatial distribution of another. In contrast, common methods employed in spatial analysis of infectious diseases such as SaTScan detect spatial clusters using circular windows but may be less specific in revealing interactions between diseases. 25 Methods like Local Indicator of Spatial Association (LISA), Moran’s I, Getis-Ord’s Gi*, and Knox test, while useful for global and local spatial clustering, may not offer the same level of granularity in assessing the interaction between multiple disease type. 25
Our study had several limitations as it relies on passive surveillance data that were subjected to voluntary reporting, which might introduce reporting biases. Additionally, the exclusion of non-laboratory-confirmed cases and enteric fever carriers might lead to an underestimation of the true disease burden and the possibility of selection bias, impacting the comprehensiveness of the results. Diagnostic confirmation of probable leptospirosis (positive rapid test or ELISA) was also not made mandatory; hence, a higher incidence of the disease was a possibility.
Conclusion
In conclusion, our research highlights the significant spatial dependence between enteric fever and leptospirosis, stressing the vital role of spatial analysis in epidemiology. Co-endemicity and spatial dependence of enteric fever and leptospirosis present significant challenges to public health in affected regions. Recognizing spatial patterns and interconnections, we advocate for a collaborative approach to address these health challenges effectively, emphasizing the urgency for a multi-faceted strategy. Integrating findings into public health policies and practices will be key to effectively addressing the challenges posed by the simultaneous presence of multiple infectious diseases in specific regions. Spatial analysis is pivotal in tailoring resilient, region-specific public health measures to combat these interconnected health threats.
Supplemental Material
sj-docx-1-aph-10.1177_10105395241286118 – Supplemental material for Spatial Interaction Between Leptospirosis and Enteric Fever in Kelantan, Malaysia: A 2016-2022 Notification Registry Analysis
Supplemental material, sj-docx-1-aph-10.1177_10105395241286118 for Spatial Interaction Between Leptospirosis and Enteric Fever in Kelantan, Malaysia: A 2016-2022 Notification Registry Analysis by Hazlienor Mohd Hatta, Kamarul Imran Musa, Nik Mohd Hafiz Mohd Fuzi and Paula Moraga in Asia Pacific Journal of Public Health
Footnotes
Acknowledgements
The authors would like to thank the Kelantan State Health Department’s Communicable Disease Control (CDC) unit. We would like to express our gratitude to the Director General of Health Malaysia for granting us permission to perform this research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.