
Abstract
This study investigated the association between COVID-19-related characteristics and oral health in Korean adults. Data from the 2021 Korean Community Health Survey were used (n = 229 242). A total of 26.5% responded that their subjective oral health status was good, and 20.2% experienced chewing discomfort. People less affected by COVID-19 in their daily lives were more likely to have good subjective oral health. Subjective oral health status was more likely to be good in those who had increased physical activity, did not consume instant food, smoked less, and were vaccinated against COVID-19. Those who were concerned about being infected, concerned about being criticized, and worried about economic damage due to COVID-19 were more likely to experience chewing discomfort. People with decreased physical activity, increased instant food consumption, and increased alcohol drinking and smoking due to COVID-19 were more likely to experience chewing discomfort. Our findings suggested that COVID-19-related characteristics were associated with oral health status.
What We Already Know
COVID-19 is an infectious respiratory disease that is transmitted through droplets in coughs and sneezes.
Owing to the nature of dental treatment, which treats the oral cavity, there has been a decrease in the number of patients visiting dental clinics during the COVID-19 pandemic.
The COVID-19 pandemic has affected access to dental visits and treatment.
What This Article Adds
A total of 26.5% responded that their subjective oral health status was good, and 20.2% experienced chewing discomfort.
People who were less affected by COVID-19 in their daily lives and whose health behaviors improved were more likely to have good subjective oral health.
Those who were concerned about being infected, concerned about being criticized, and worried about economic damage due to COVID-19 were more likely to experience chewing discomfort.
Introduction
Coronavirus disease (COVID-19) is a respiratory infection caused by a new type of coronavirus that first emerged in Wuhan, China, in December 2019 and has since spread across China and around the world. On March 11, 2020, the World Health Organization declared COVID-19 a global pandemic. In Korea, the first confirmed case occurred in January 2020, and as of August 2023, the cumulative number of confirmed COVID-19 cases was more than 34 million and resulted in 35 000 deaths. 1
To prevent the spread of the COVID-19 infectious disease, social distancing measures such as refraining from going out, meeting and using multiple facilities, prohibiting the use of indoor sports facilities, recommending working from home, and restricting restaurant and cafe business hours have been implemented.2,3 The prolonged COVID-19 pandemic has affected various aspects of daily life, including economy, society, employment, and health care. Dental care includes procedures that can transmit the virus through aerosols, and dental personnel are among the highest risk groups for transmission and contact of the virus.4,5
Owing to the nature of dental care that treats the oral cavity, the number of patients visiting the dentist decreased during the COVID-19 pandemic, affecting access to dental visits and care. In a review that presented safety precautions to be followed from patient admission to treatment completion, to prevent the spread of COVID-19, dental treatment was limited to patients in urgent or emergency situations. 6 According to data released by the Health Policy Institute in Korea, when comparing the number of patients who visited the hospital in April 2020 with the average for the last five years, a total of approximately 820,000 patients decreased by approximately 20.5%. This decrease in the number of patients resulted in a 20.7% decrease in dental treatment costs compared with the average over the past five years. A decrease in dental visits by patients not only leads to a decrease in dental revenue but can also affect individual oral health care if proper dental treatment is delayed. 7
A positive perception of oral health is essential for practicing oral health behaviors, and continuous oral health management is essential to prevent dental caries and periodontal diseases. 8 Chewing discomfort is associated not only with oral diseases such as periodontal disease and dental caries but also with other chronic diseases such as diabetes, myocardial infarction, arthritis, and asthma. 9
In previous studies, women reported better oral health than men, and younger age, higher household income, and higher educational levels were associated with better oral health.10,11 Chewing discomfort was higher in those with low-income levels, low education levels, 12 increased smoking, decreased alcohol consumption, limitations in daily life due to disease, and the presence of chronic diseases. 9
Although the COVID-19 pandemic has raised concerns regarding oral health, data on oral health in adults are limited. Therefore, this study aimed to identify the relationship between COVID-19-related characteristics, subjective oral health status, and chewing discomfort in Korean adults.
Methods
Data Source and Study Population
This study used raw data from the 2021 Korea Community Health Survey (KCHS). The KCHS has been conducted every year since 2008 with the goal of producing community health statistics for the establishment and evaluation of community health care plans. The Korea Disease Control and Prevention Agency (KDCA), 17 cities and provinces, 255 community health centers, and 34 community universities participated in the study. The population of the survey comprised adults aged 19 years or older residing in the sample household at the time of the survey. Sample areas were selected using the probability proportional sampling method, and sample households were selected using a systematic sampling method. 13
Trained interviewers visited households selected as samples to conduct a 1:1 interview, and the interviewers directly entered the responses on a tablet personal computer. The interviewers were vaccinated against COVID-19 according to the guidelines for conducting investigations to prevent infectious diseases and were tested for COVID-19 before the start of the investigation; only those who tested negative participated in the investigation. In addition, health conditions such as fever and cough were checked daily, interviewers with symptoms were excluded from the survey, and quarantine rules were strictly followed. The KCHS protocol was approved by the Institutional Review Board of the KDCA (2016-10-01-P-A), and informed consent was obtained from all participants.
The survey period of the 2021 KCHS was from August 16, 2021, to October 31, 2021. A total of 229 242 people participated in the survey, and data of 229 239 people were analyzed. Three participants did not respond to questions on oral health status and were therefore excluded.
Study Variables
General and Health-Related Characteristics
General characteristics included sex (male, female), age (19-44, 45-64, 65+ years), residential area (urban, rural), educational level (elementary school, middle and high school, university+), and spouse (with, without). Health-related characteristics included smoking status (never, former, current), alcohol drinking frequency (none, ≤1/month, ≥2/month), exercise (yes, no), hypertension diagnosis history (yes, no), diabetes diagnosis history (yes, no), and tooth brushing after lunch yesterday (yes, no).
Coronavirus Disease-Related Characteristics
The impact of COVID-19 pandemic on daily life was assessed on a scale of 0 to 100 for the following questions, with 0 to 30 points being “very much,” 40 to 50 points being “a lot,” 60 to 70 points being “a little,” and 80 to 100 points being classified as “very slightly affected” (daily life is rather active compared with before the COVID-19 pandemic) and the question posed was: “If your daily life before the COVID-19 pandemic is 100 points and your daily life completely stopped is 0 points, what is your current status?”
The expected responses for psychological impact caused by COVID-19 were “strongly yes” or “yes” as response to concerns about infection with COVID-19, concerns about criticism from others due to infection with COVID-19, and concerns about economic damage caused by COVID-19 which were assessed using the following statements: “I am concerned about contracting COVID-19,” “I am concerned that if I am infected with COVID-19, I will be criticized or harmed by those around me for that reason,” and “I am concerned that the COVID-19 pandemic will cause economic damage to me and my family (including losing or finding a job).”
Changes in household income and consumption due to COVID-19 were evaluated as “decrease,” “no change,” or “increase” for the following questions: “Has your household’s total income changed compared to before the COVID-19 pandemic (January 2020)?” “Compared to before the COVID-19 pandemic (January 2020), did your household have any changes in essential consumption expenditures such as clothing, food and dining, housing, hospital care, and education?”
Changes in health behavior due to the COVID-19 pandemic were evaluated with the following questions as “increased,” “no change,” “decreased,” or “not applicable” for each of physical activity, instant food intake, drinking, and smoking: “What changes compared to before the COVID-19 pandemic?”
People vaccinated for COVID-19 were identified based on a “yes” or “no” response to the following question: “Have you ever been vaccinated against COVID-19?”
Oral Health Status
Oral health status was evaluated based on the subjective oral health status and chewing discomfort. Good subjective oral health status was defined as a “very good” or “good” response to the following question: “When you think about yourself, how do you feel about your oral health, including your teeth and gums?” Chewing discomfort was assessed based on the responses “very uncomfortable” or “uncomfortable” to the following question: “Do you currently feel difficulty or discomfort in chewing food due to problems in your mouth, such as teeth, dentures, or gums?”
Analysis
The SPSS version 27.0 was used for the data analysis. Descriptive analyses were conducted to present the distribution of the general characteristics, health-related characteristics, COVID-19-related characteristics, and oral health status of the study population. Chi-square tests were conducted to analyze the relationships between general characteristics, health-related characteristics, COVID-19-related characteristics, subjective oral health status, and chewing discomfort. Finally, multiple logistic regression analysis was conducted to determine the relationship between COVID-19-related characteristics, subjective oral health status, and chewing discomfort. The statistical significance level was tested based on P < .05.
Results
The proportions of participants with good subjective oral health and chewing discomfort were 26.5% and 20.2%, respectively. The proportion of good subjective oral health was 26.7% in males and 26.4% in females; 36.6% in 19 to 44 years old, 26.3% in 45 to 64 years old, and 17.8% in those aged 65 years or older. According to smoking status, the good subjective health rate was 28.4% among non-smokers, 23.8% among ex-smokers, and 22.1% among smokers. The rate of chewing discomfort was 19.5% in males and 20.7% in females; 5.7% in 19 to 44 years old, 16.7% in 45 to 64 years old, and 37.2% in those aged 65 years or older. According to smoking status, the rate of experiencing chewing discomfort was 18.9% in non-smokers, 22.7% in ex-smokers, and 22.1% in smokers (Table 1).
Oral Health Status According to General and Health-Related Characteristics.
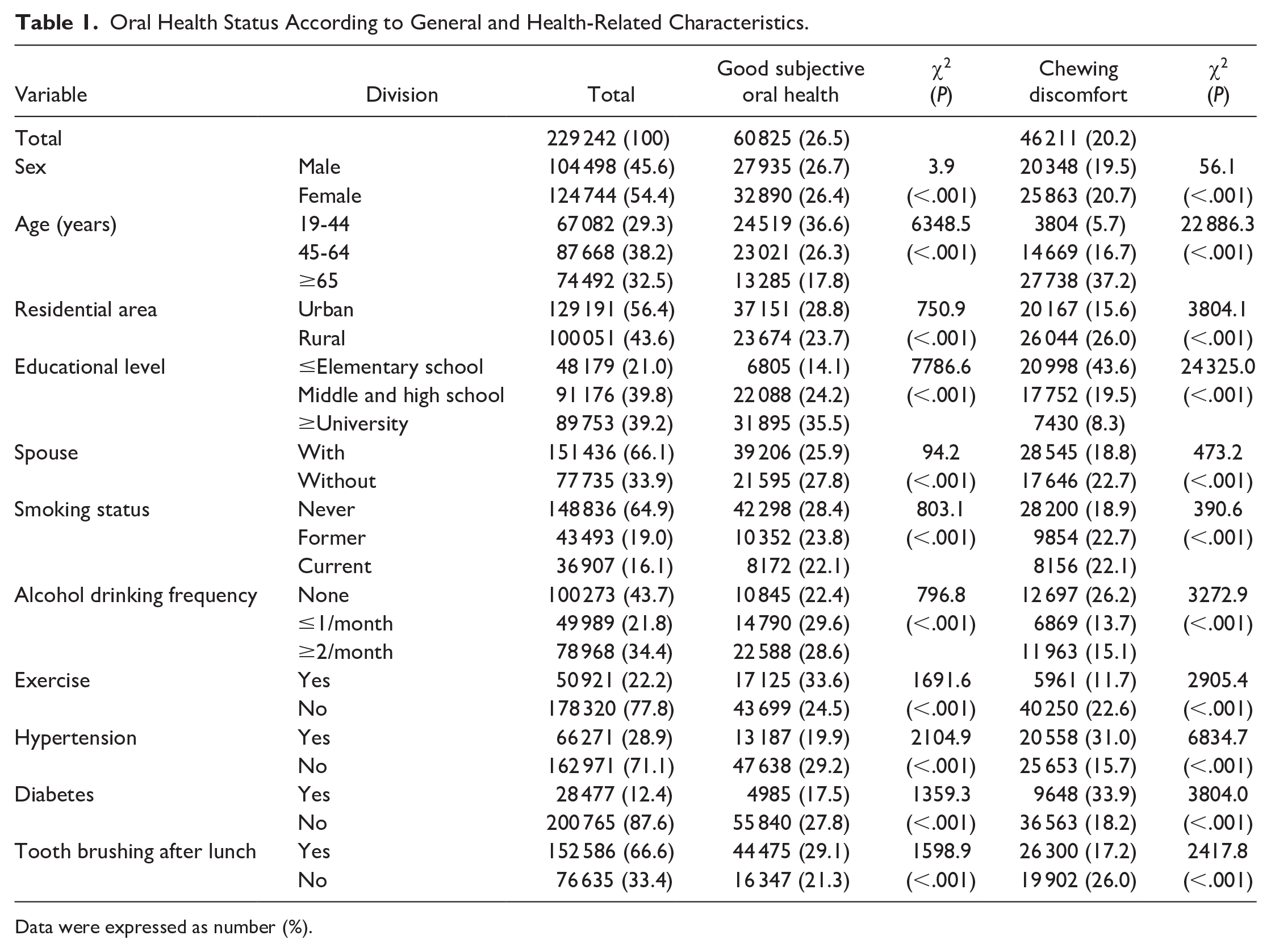
Data were expressed as number (%).
The proportion of patients with good subjective oral health was 25.7% when the degree of impact on daily life due to COVID-19 was very high (25.3%, 28.0%, and 27.1%, respectively). The good subjective oral health rate was 26.7% when income decreased due to COVID-19, and 30.7% when income increased. The rate of chewing discomfort was 20.8% for those who experienced a significant impact on their daily lives due to the COVID-19 pandemic: 20.5%, 17.3%, and 22.5%, respectively. Regarding the psychological impact, the rate of chewing discomfort was 21.2% among those who were concerned about being infected, 21.3% among those who were concerned about being criticized, and 21.9% among those who were concerned about receiving economic losses due to COVID-19 (Table 2).
Oral Health Status According to COVID-19-Related Characteristics.
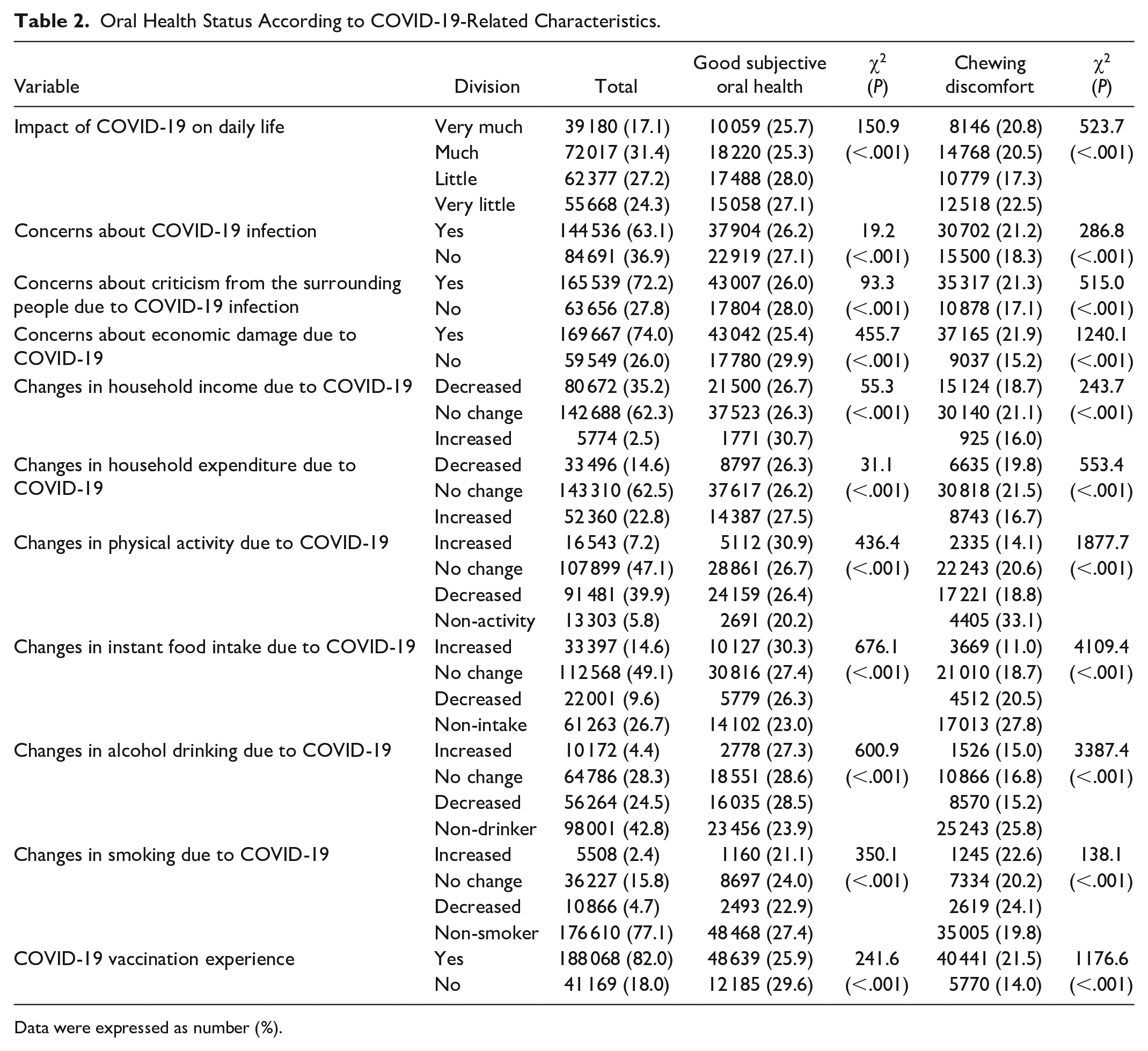
Data were expressed as number (%).
The odds ratio for good subjective oral health status was significantly higher in those who were very little affected by COVID-19 in daily life (odds ratio [OR] = 1.15, confidence interval [CI] = [1.11, 1.18]) and those who were concerned about being infected (OR = 1.05, CI = [1.03, 1.08]). In addition, the people who had increased physical activity due to COVID-19 (OR = 1.05, CI = [1.01, 1.09]) and those who were vaccinated for COVID-19 were more likely to have good subjective oral health (OR = 1.13, CI = [1.10, 1.16]). The odds ratio for the experience of chewing discomfort was significantly high in those who were concerned about COVID-19 infection (OR = 1.04, CI = [1.01, 1.07]), those who were concerned about being criticized around them (OR = 1.03, CI = [1.00, 1.06]), and those who were concerned about economic damage due to COVID-19 (OR = 1.11, CI = [1.07, 1.15]). Those with increased alcohol drinking (OR = 1.15, CI = [1.08, 1.23]) and smoking (OR = 1.28, CI = [1.19, 1.38]) due to COVID-19 were more likely to experience chewing discomfort (Table 3).
Oral Health Status According to COVID-19-Related Characteristics.
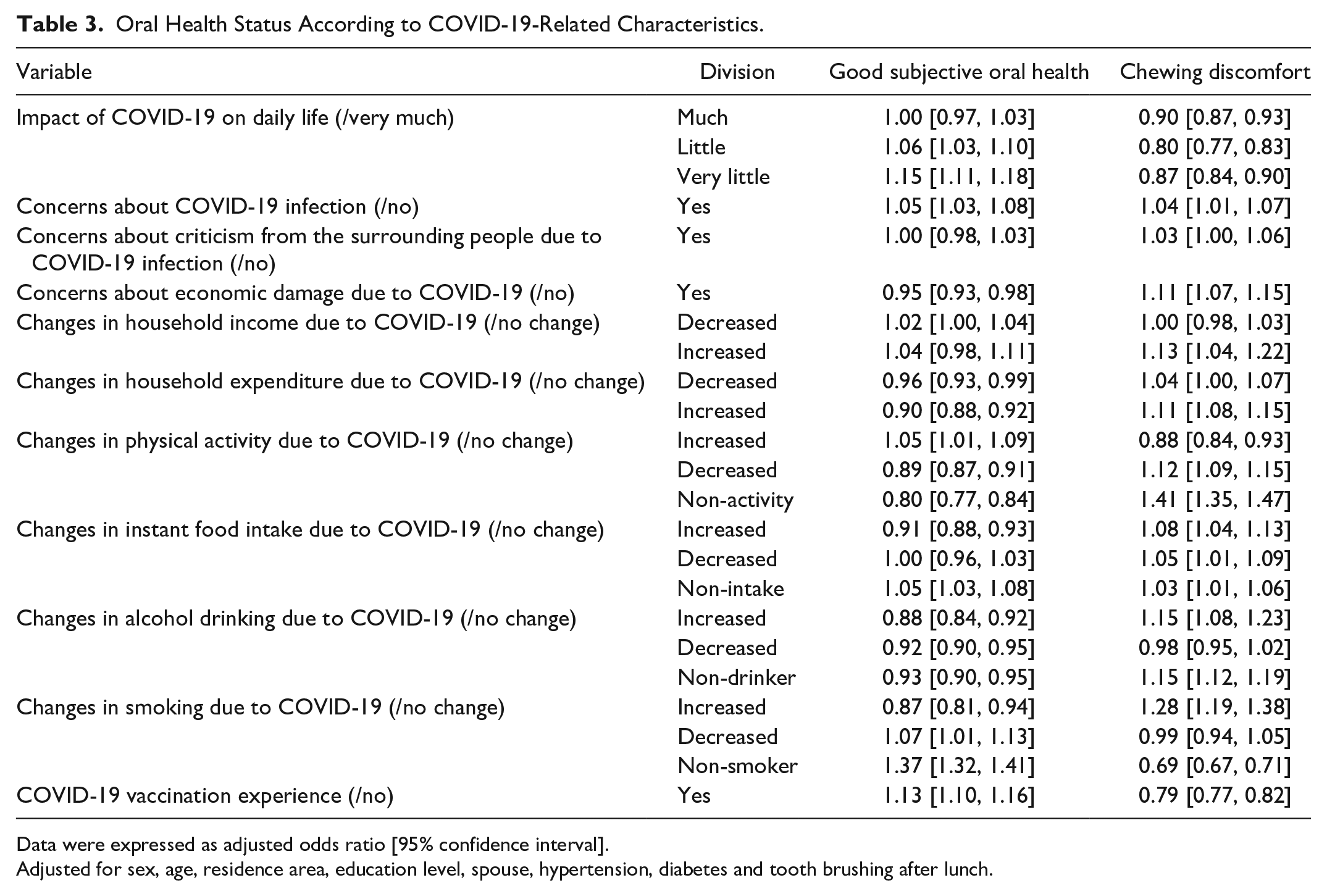
Data were expressed as adjusted odds ratio [95% confidence interval].
Adjusted for sex, age, residence area, education level, spouse, hypertension, diabetes and tooth brushing after lunch.
Discussion
The COVID-19 is an infectious respiratory disease caused by a new type of coronavirus that is transmitted through droplets in coughs and sneezes. The prolonged COVID-19 pandemic is affecting all aspects of the economy, society, employment, and health care. This study aimed to investigate the oral health status of Korean adults during the COVID-19 pandemic using the 2021 KCHS data.
In this study, the good subjective oral health rate was 26.5% in 2021, which increased from 23.1% in the 2019 KCHS before the COVID-19 pandemic. The discomfort experience rate was 20.2% in 2021, which decreased from 21.3% in the 2019 KCHS. In this study, the subjective oral health rate and chewing discomfort were 26.5% and 20.2%, respectively, in 2021. In 2019, before the COVID-19 pandemic, they were 23.1% and 21.3%, respectively. Compared with the pre-COVID-19 pandemic period, the number of cases recognizing that their subjective oral health condition was good increased and chewing discomfort decreased. Owing to the COVID-19 pandemic, interest in the importance of daily health care and health behaviors may have increased. After the COVID-19 pandemic, regular visits to hospitals and clinics decreased, but oral health behaviors, such as brushing, improved, especially among those with a higher fear of COVID-19. 14
People who were greatly affected by COVID-19 in their daily lives and those who were concerned about COVID-19 were less likely to perceive their subjective oral health as good and were more likely to complain of chewing discomfort. The greater the change in daily life due to COVID-19, the higher the likelihood of feeling stressed; considering the prolonged COVID-19 pandemic, management policies for groups with vulnerable demographic, social, and health-related characteristics are required. 15 Greater the number of people who perceive their physical and oral health status as healthy, the greater positive effect it had on health behaviors related to oral care. 16 Therefore, as restrictions in daily life caused by COVID-19 can negatively associate subjective oral health or chewing discomfort, continuous management is necessary in the future.
People whose consumption expenditures changed owing to COVID-19 were less likely to have good subjective oral health and more likely to complain of chewing discomfort. The COVID-19 pandemic reduced household income and expenditure and had a greater impact on expenditure than on income.17,18 Over the past 10 years, the prevalence of negative oral health perception, chewing discomfort, and speaking discomfort among Korean adults has decreased overall but is still high, and the difference between income levels generally tends to persist or worsen. 19 The frequency of dental treatment and level of self-care were relatively low in the lower socioeconomic group.20,21 Low-income individuals were reported to be a high-risk group for poor oral health even before COVID-19, and COVID-19 would have further worsened their economic situation. Therefore, policies to increase dental service accessibility for socioeconomically vulnerable groups are required to reduce the oral health gap.
In this study, when smoking or drinking increased due to COVID-19, the likelihood of good subjective oral health was low, and the likelihood of chewing discomfort was high. In some cases, unhealthy behaviors, such as smoking and drinking, have decreased owing to COVID-19. However, 15.8% and 28.3% of the participants did not change their smoking or drinking status, respectively, and were still maintaining unhealthy behaviors, even during times when interest in personal hygiene or health increased, such as COVID-19. In addition, smoking and drinking are well-known risk factors for oral diseases such as periodontal disease.22,23 Therefore, oral health education on the harmful effects of smoking and drinking should be continued and people who continue to engage in unhealthy behaviors should be managed, even in situations such as COVID-19.
People who did not receive COVID-19 vaccination were less likely to have good subjective oral health and were more likely to experience chewing discomfort. People who received preventive medical services such as health checkups were related to other preventive services such as vaccinations.24,25 Therefore, individuals vaccinated against COVID-19 may have had good oral health because they followed the recommended health guidelines or were interested in their health.
One limitation of this study is that the KCHS is a cross-sectional study, which makes it difficult to identify causal relationships between the variables. In previous studies, oral examinations and use of oral aids were important factors affecting oral health; however, these were not included in the survey. In addition, COVID-19-related characteristics including clinical characteristics such as confirmed experience or self-isolation were not included.
Conclusion
This study identified the relationship between COVID-19-related characteristics, subjective oral health status, and experience of chewing discomfort in Korean adults by using the KCHS data that can represent Korean adults. The results of this study can be used as evidence for oral health management during infectious disease pandemic.
Footnotes
Authors’ Note
This article is a condensed form of the first author’s master’s thesis from Chosun University.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Basic Science Research Program through the National Research Foundation of Korea (NRF), funded by the Ministry of Education (2021R1I1A3041301) and the Ministry of Science and ICT (NRF-2022R1A5A2030454).