
Abstract
The COVID-19 pandemic reduced social contact, causing social isolation, which is dependent on risk perception—a motivation for social distancing. While studies have examined risk perception as a dual process, its application to real-world risk situations is unexplored. This study investigated the relationships between risk perception, social contact changes, and social isolation during COVID-19. A nationwide cross-sectional sample of 804 adults completed computer-assisted telephone interviews. The main variables were social isolation (face-to-face and non-face-to-face) and risk perception (affective and cognitive). Data were analyzed using analysis of variance, logistic regression models, and multinomial logistic regression models. Affective and cognitive risk perceptions were associated with changes in face-to-face and non-face-to-face social contact. Only affective risk perception was associated with social isolation. Thus, social isolation is a health-related concept, higher levels are associated with poorer mental and physical health. In addition, the isolation-reduction recommendations put forth have important well-being-improvement implications.
Keywords
What We Already Know
Higher risk perception is associated with protective behaviors.
Social isolation negatively affects mental and physical health.
Virtual communication can compensate for reduced face-to-face contact.
What This Article Adds
ARP and CRP are differently associated with face-to-face and non-face-to-face interaction.
Only ARP is associated with face-to-face and non-face-to-face social isolation.
Some individuals reduce social contact, aligning with the “poor-get-poorer” hypothesis.
Introduction
Social isolation has become a critical problem following the COVID-19 pandemic. Social isolation involves a lack of belonging, social engagement, contact, and support,1,2 and negatively impacts individuals’ physical and mental health, with examples including cardiovascular disease, psychological distress, and mortality.2,3 Even short-term social isolation can have long-term effects, leading to poorer mental health three years later. 4 Owing to COVID-19, people worldwide have been affected by social isolation. 5 Thus, studying social isolation can clarify the pandemic’s unintended consequences.
The South Korean government implemented strict measures to control the virus’ spread: mandatory quarantine protocols, rigorous testing and contact tracing, widespread mask mandates, and restrictions on public gatherings. 4 This limiting of social interactions significantly decreased social contact compared to pre-pandemic levels.6,7 The risk of social isolation during COVID-19 varied by age, gender, and risk perceptions.5,8 For example, people exposed to COVID-19 news for longer periods of time were associated with higher social isolation. 8 Identifying vulnerable groups is essential for targeting support and developing strategies for future national emergencies.
Both face-to-face and non-face-to-face interactions must be considered when discussing the social isolation caused by the COVID-19 pandemic. Face-to-face contact declined significantly during the pandemic, especially among people with lower socioeconomic status. 9 However, non-face-to-face social contact (e.g., phone calls, emails, and video calls) increased during the pandemic as an alternative approach. 6 Non-face-to-face interactions also positively affected mental health by reducing social isolation. 10 However, this may vary by demographic, for example, older adults of resource-limited status. 10
Risk perception refers to how a person perceives the risk of a situation and can vary depending on the person and situation in question. It significantly motivates individuals to perform specific actions in certain situations. During the pandemic, risk perception may have significantly influenced people following prevention-related guidelines. 11 This is also true for social distancing behaviors, wherein the perceived risk of emerging infectious diseases, such as COVID-19, predicted whether an individual engages in social distancing behaviors. 12
Affect and cognition are critical for measuring risk perception. Affective risk perception (ARP) is an instinctive, intuitive response to risk, while cognitive risk perception (CRP) is a logical response. 13 The outcomes of both determine a person’s behavior and attitude toward risk. 14 The importance of these two aspects can be explained by the “dual-process theory,” 13 contending that humans have two fundamental modes: the affective process, which is instinctive, automatic, and fast, and the cognitive process, which is analytical, controlled, and slow. 15
In the context of risk perception, this theory suggests that the two processes operate in different modes during a risk experience. Specifically, how people fear a risky stimulus may affect their risk perception; the more fearful people are, the more they will overestimate the risky stimulus’ impact. 16 Simultaneously, people’s assessment of the risk depends on the perceived frequency of experiencing it, which can significantly impact a person’s behaviors. 17 While studies have attempted to understand risk perception as a dual process (e.g., Do et al 18 ), its application to real-world risks remains unexplored. 17
Previous studies have suggested that higher risk perception of COVID-19 leads to more proactive preventive behaviors (e.g., Dryhurst et al 19 ), which may be related to individuals’ quarantine and social distancing behaviors. Individuals with higher-risk perception actively avoided social interactions as a protective measure, including avoiding gatherings and maintaining physical distance. 20 A higher-risk perception of COVID-19 is associated with increased social distancing adherence, raising the likelihood of social isolation being experienced.
Therefore, this study used a nationally representative sample to investigate the COVID-19 social isolation relationship by measuring both affective and CRP of COVID-19. The research aimed to elicit whether individuals’ face-to-face or non-face-to-face social contact and social isolation differed depending on their ARP and CRP during COVID-19.
Methods
Participants
We used a nationwide cross-sectional sample of 1001 adults aged 18 years or older, collected over March 2–3, 2022. The sample was selected using poststratification by sex, age, and region. Of the 25 534 eligible cases, 6537 were contacted (contact rate: 25.6%), and 1001 responded (cooperation rate: 15.3%; response rate: 3.9%). Trained interviewers conducted all surveys via computer-assisted telephone interviews (90% on mobile phones and 10% on landlines) using random digit dialing (RDD) numbers.
The analytic sample included 804 respondents, excluding those with missing data (n = 58). Exclusion criteria comprised those reporting increased face-to-face social contact since the pandemic began (n = 16); those with farming, forestry, or fishery jobs (n = 24); and residents of Jeju (n = 12). Only one student among 64 reported face-to-face social isolation (n = 64); thus, students were excluded. Participants previously infected with COVID-19 (n = 23) were also excluded as they did not report the ARP and CRP. The survey weight was based on the resident registration data from the Ministry of the Interior and Safety (February 2022). Gallup Korea, an affiliate of Gallup International, conducted the survey.
Demographic factors included age, sex, education, occupation, self-reported household economic status, and residential area. Age was categorized into five groups (18–29, 30–39, 40–49, 50–59, and 60+) and education into three groups (middle school or below, high school, and college or above). Economic status was classified into three levels based on five original categories: lower (including lower and lower-middle), middle, and upper (including upper-middle and upper). Occupation was classified into five groups (self-employed, blue-collar, white-collar, full-time homemakers, and unemployed/retired/others). Residential areas were categorized into seven regions: Seoul, Incheon, or Gyeonggi Province; Gangwon Province; Chungcheong Province; Jeolla Province; Daegu or Gyeongbuk; and Busan, Ulsan, or Gyeongnam.
Survey Instruments
Risk perception of COVID-19
The risk perception of COVID-19 was assessed in terms of ARP and CRP. Affective risk perception was evaluated using a single-item question—“How worried are you about being infected with COVID-19?”—with responses rated on a 4-point Likert scale (not worried at all, not so worried, somewhat worried, and very worried). Cognitive risk perception was assessed using another question—“How likely do you think it is that you are infected with COVID-19?”—rated on a 4-point Likert scale (not likely at all, less likely, somewhat likely, and very likely). Higher scores indicated higher ARP and CRP for COVID-19.
Social contact change during the COVID-19 pandemic
Social contact changes were assessed using items from the National Social Life, Health, and Aging Project (NSHAP COVID-19 substudy). These changes were evaluated from both face-to-face and non-face-to-face perspectives. 9 Face-to-face social contact change was assessed by asking: “Compared to before the COVID-19 pandemic, how much has the frequency of in-person visits with family not living with you or friends changed?” Change in non-face-to-face contact was measured by asking, “Compared to before the pandemic, how much has the frequency of online communication with family not living with you or friends changed?” Responses were rated as “no change,” “decreased,” or “increased.” Only 16 respondents reported increased face-to-face social contact; thus, they were excluded from the analysis.
Social isolation
This study defined social isolation as a lack of social contact to better understand the consequences of social distancing during the COVID-19 pandemic.1,21 Based on NSHAP COVID-19 substudy questionnaires, social contact was measured in two forms of isolation: face-to-face and non-face-to-face. 9 Face-to-face social isolation was assessed with the question, “Since the start of the pandemic, how often have you had in-person visits with family not living with you or friends?” Non-face-to-face social isolation was assessed with the question, “Since the start of the pandemic, how often have you engaged in online communication with family not living with you or friends?” Responses were rated on a 5-point scale (at least three times a week, once or twice a week, once or twice a month, once or twice a year, and rarely or never). Respondents who reported rarely or never meeting family or friends in person were classified as having face-to-face social isolation. Those who reported online communication once or twice a year, or rarely or never, were classified as having non-face-to-face social isolation.
Data Analysis
The descriptive characteristics of the four dependent variables were analyzed using analysis of variance (ANOVA) and post-hoc analyses. Logistic regression analyses investigated ARP’s and CRP’s effects on changes in face-to-face social contact, social isolation, and non-face-to-face social isolation. Multinomial logistic regression analyses examined the association between risk perception and changes in non-face-to-face social contact. Affective risk perception and CRP were analyzed in separate models. All logistic and multinomial regression models were adjusted for age, sex, education, occupation, self-reported household economic status, and residential area. Figures 1 and 2 present the findings of the eight regression models and show the predicted probabilities of social contact change and social isolation. Statistical significance was set at P < .05, two-tailed. Analyses were performed using Stata 17.0.
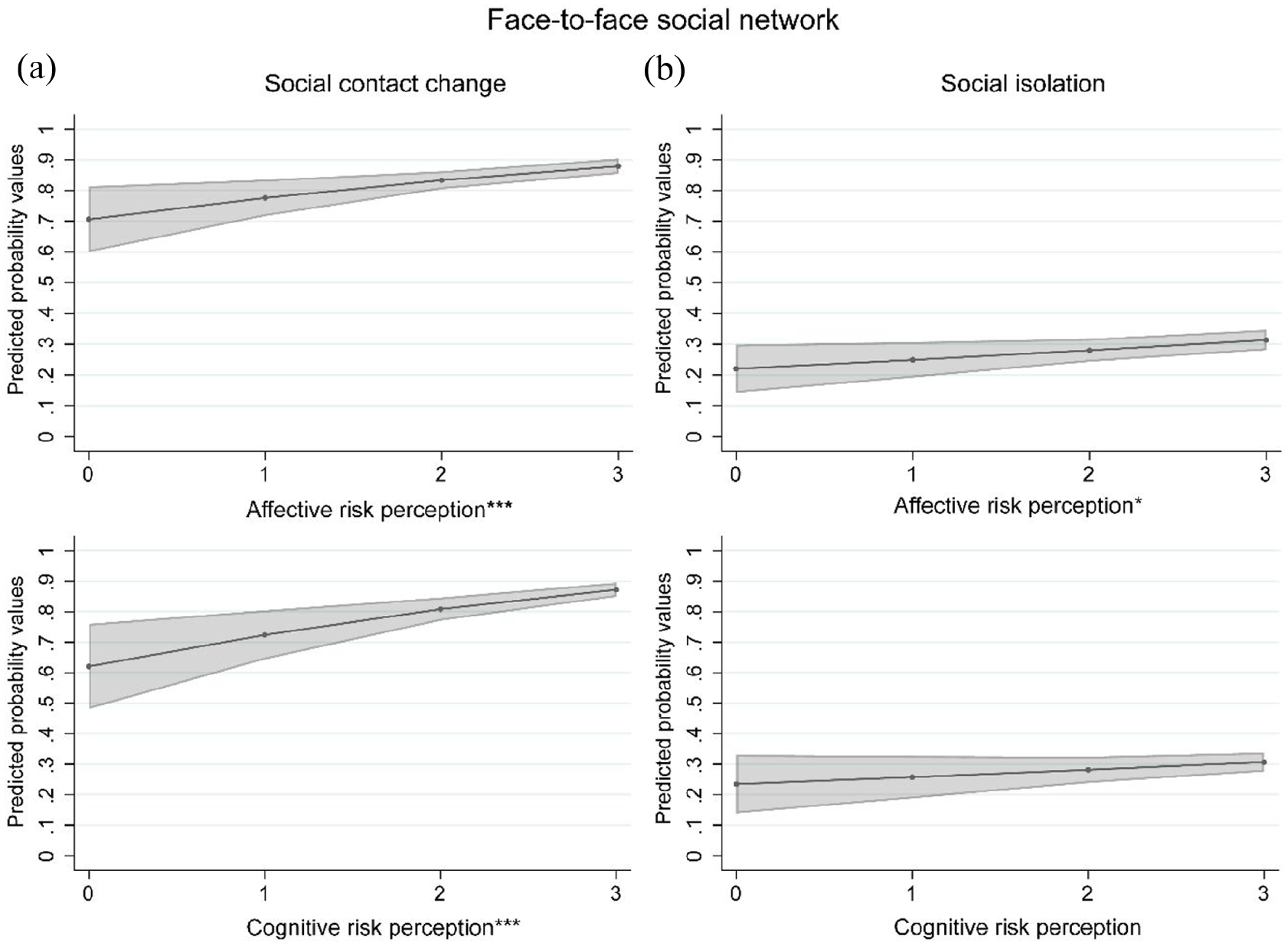
Association between face-to-face social network and two types of risk perception. The predicted probability values were calculated using the logistic regression models. All the models were adjusted for age, sex, educational level, occupation, self-reported household economic status, and residential area.
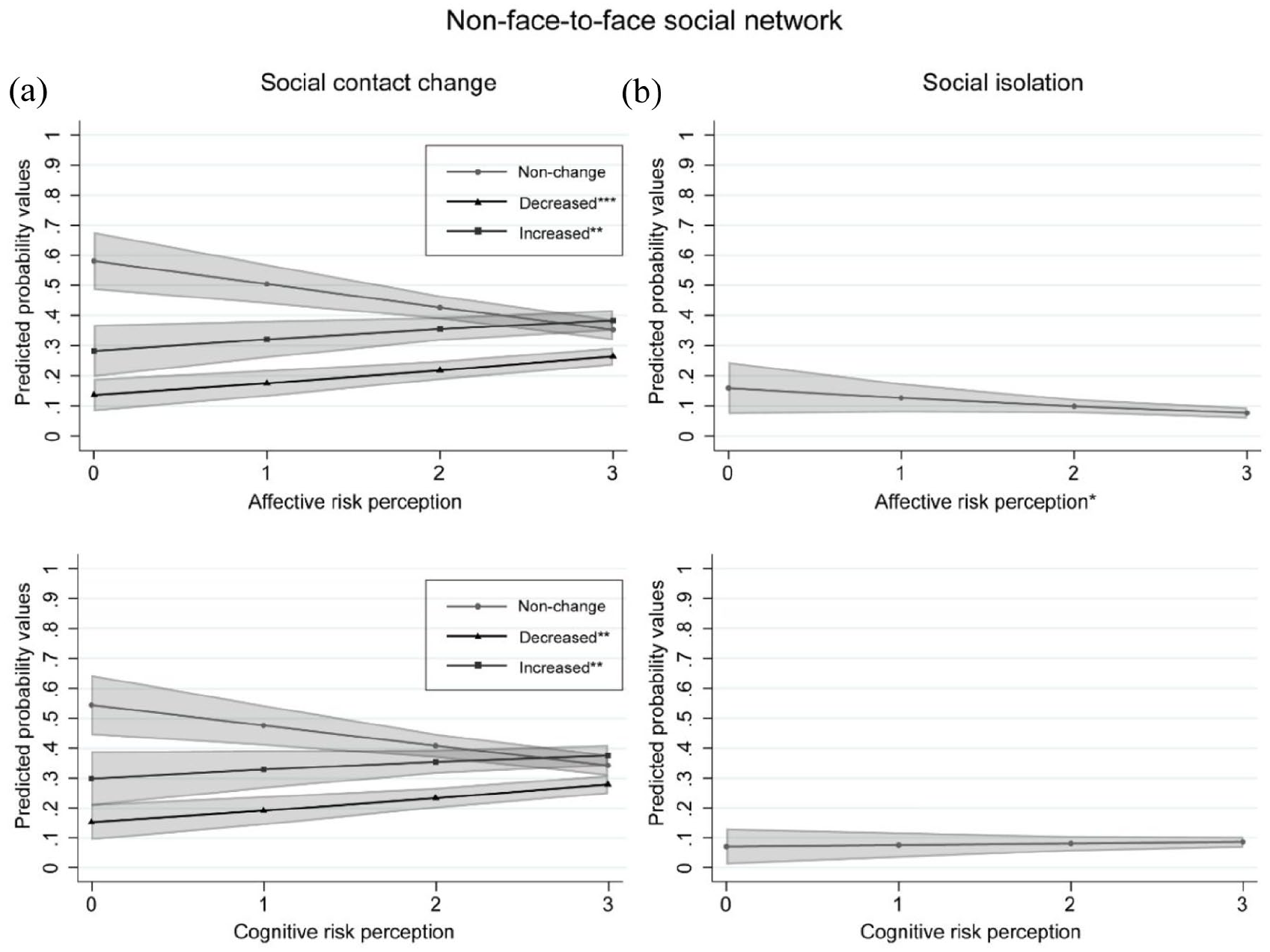
Association between non-face-to-face social network and the two types of risk perception. The predicted probability values were calculated using the multinomial logistic regression and logistic regression models. All the models were adjusted for age, sex, educational level, occupation, self-reported household economic status, and residential area. The nonchange group was used as the reference group in the multinomial logistic regression models shown as Figure 2a.
Results
Table 1 presents the descriptive characteristics of changes in social contact and social isolation. For face-to-face social contact, the decreased group exhibited higher ARP and CRP than the nonchange group (ARP: 2.70 ± 0.04 vs 2.32 ± 0.11, p = 0.001; CRP: 2.93 ± 0.03 vs 2.53 ± 0.09, P < .001). No group differences were found in sex, economic status, or residential area. The decreased group had a smaller proportion of respondents aged 18 to 29 years (70.2%) and unemployed/retired/others (74.6%), but more respondents with college education (88.2%). The socially isolated group had higher ARP (2.78 ± 0.07 vs 2.59 ± 0.04, P = .015), but similar CRP. This group also had fewer aged 18 to 29 (16.2%) and white-collar workers (20.1%), and more respondents with low education (50.3%) and low economic status (41.7%).
Descriptive Characteristics of Face-To-Face and Non Face-To-Face Social Network (n = 804).
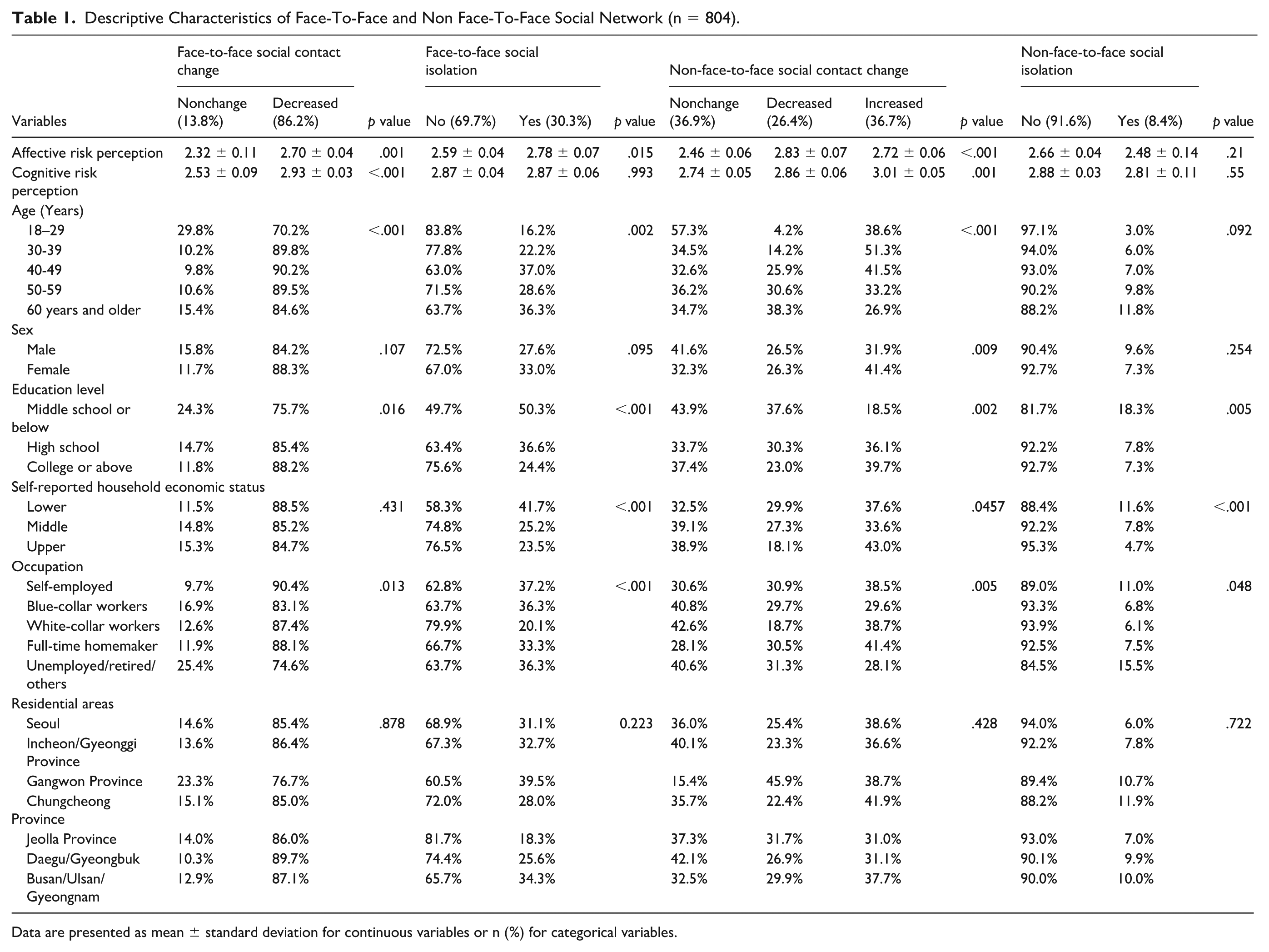
Data are presented as mean ± standard deviation for continuous variables or n (%) for categorical variables.
As regards non-face-to-face social contact, both the decreased and increased social contact groups exhibited higher ARP than the nonchange group (2.83 ± 0.06 in decreased vs 2.72 ± 0.06 in increased vs 2.46 ± 0.06 in nonchange, P < .001). The increased group also exhibited higher CRP (3.01 ± 0.05 in increased vs 2.86 ± 0.06 in decreased vs 2.74 ± 0.05 in nonchange, P = .001). Significant group differences were found in age, sex, education, economic status, and occupation. The decreased group contained more respondents aged 60+ (38.3%) and fewer with a college education (23.0%), upper economic status (18.1%), and white-collar workers (18.7%). The increased group contained fewer aged 60+ (26.9%), female (41.4%), low education (18.5%), and unemployed/retired/others (28.1%). Regarding non-face-to-face social isolation, ARP, and CRP did not differ significantly, but the isolated-individuals group contained more low education (18.3%), low economic status (11.6%), aged 60+ (11.8%), and unemployed/retired/others (15.5%).
Figure 1 shows associations between risk perception and changes in face-to-face social contact and social isolation from the logistic regression models. Higher risk perception was associated with an increased predicted probability of being in the decreased social contact group (Figure 1a), which increased from 0.70 to 0.88 in ARP (odds ratio [OR] = 1.53, P < .001; Supplemental Table 1) and from 0.63 to 0.88 in CRP (OR = 1.67, P < .001 in Supplemental Table 2). Higher-ARP individuals were more likely to belong to the isolated group (Figure 1b), with the predicted probability increasing from 0.22 to 0.31 (OR = 1.19, P = .046; Supplemental Table 1). However, CRP exhibited no significant association.
Figure 2 presents results for non-face-to-face contact and isolation from the multinomial logistic and logistic models. High ARP was associated with an increased predicted probability of being in both the decreased and increased social contact groups, with predicted probability increasing from 0.15 to 0.30 and from 0.30 to 0.38, respectively (compared to the nonchange group, OR = 1.46, P < .001 in the decreased group, OR = 1.28, P = .007 in the increased group; Figure 2a; Supplemental Table 3). In addition, as CRP increased, there was a rise in the predicted probability of being in the decreased group from 0.19 to 0.27 and the increased group from 0.21 to 0.37 (compared to the nonchange group, OR = 1.38, P = .004 in the decreased group, OR = 1.46, P = .001 in the increased group; Supplemental Table 4). Higher-ARP individuals were less likely to belong to the isolated group, with the predicted probability decreasing from 0.16 to 0.08 (OR = 0.73, P = .035; Figure 2b; Supplemental Table 3). Cognitive risk perception was not significantly related to isolation.
Discussion
This research explored how risk perception influences social contact and isolation in South Korea during COVID-19. High-risk-perception individuals—especially persons with ARP—were more likely to reduce in-person interactions. Those more susceptible to infectious diseases often reported higher risk perception, particularly ARP, encouraging protective behaviors. 22 Anxiety is crucial in this process, as it alerts individuals to threats and prompts them to take preventive actions. 23 Consequently, individuals with strong ARP had reduced face-to-face interactions. However, increased virtual social engagement may have counterbalanced the reduced contact. Thus, ARP is associated with social distancing and compensatory behaviors aimed at mitigating isolation’s adverse effects. This highlights the potential for risk perception-based communication to manage social distancing while minimizing unintended consequences such as social isolation.
Existing research demonstrates that the degree of risk perception is related to engagement in protective behaviors. 24 Xie et al 22 found that high-risk perception motivated individuals to engage in social distancing; it keeps people vigilant about pandemics and motivates them to act. Furthermore, a systematic review concluded that considering risk perception is essential when judging how cooperative people are with a country’s disease prevention policies, consistent with our findings. 25 Individuals who report high levels of both CRP and ARP are more likely to experience heightened sensitivity to pandemic situations and, subsequently, have fewer face-to-face social interactions, experiencing higher levels of face-to-face social isolation.
This study identified a bidirectional relationship between CRP, ARP, and changes in virtual social interactions during the COVID-19 pandemic. Specifically, individuals with heightened CRP or ARP either increased or decreased their engagement in non-face-to-face communication. These findings are partially consistent with previous research, which has suggested that, during pandemics, when social distancing is emphasized, individuals attempt to compensate for reduced in-person interactions by turning to digital communication. This aligns with the principles of the social compensation hypothesis (SCH), 26 suggesting that individuals seek alternative means of maintaining social connections.
However, we found that some individuals with high-risk perceptions reduced both face-to-face and virtual interactions. This contradicts SCH and aligns more with the “poor-get-poorer” hypothesis, 27 which suggests those struggling with real-world connections also engage less online due to limited motivation or ability. Government-imposed restrictions on social gatherings may have worsened this trend. Had social distancing been voluntary, some might have increased virtual interactions. Instead, enforced measures may have left socially limited individuals without the means or drive to maintain remote ties, further reducing engagement.
Demographic factors such as age, sex, and personality traits also influenced whether individuals adapted their social behaviors in line with SCH or the “poor-get-poorer” hypothesis. Research suggests that younger individuals, women, and introverts are more likely to increase their virtual interactions in response to reduced face-to-face contact. Contrastingly, older individuals, men, and extroverts tend to experience a decline in both forms of social contact when face-to-face interactions are restricted, leading to heightened social isolation.8,10,26 These findings indicate that future research should explore how personal characteristics shape the relationship between risk perception and social behavior.
Social isolation emerged as a significant public health concern across the Asia-Pacific region during COVID-19, affecting diverse populations regardless of national context. 5 For example, a study from Japan reported over 20% prevalence of social isolation during the pandemic, indicating that the phenomenon was not limited to Korea. 7 This tendency of people from Asian cultures perceiving a higher risk of infection from Europeans during the COVID-19 pandemic suggests that risk perception may exert a stronger influence in Asian regions. 11 Our study adds to this regional understanding by providing empirical evidence from South Korea, highlighting the importance of risk perception and similar challenges in maintaining social connectedness during the COVID-19 pandemic.
Although this study offers valuable insights, several limitations should be noted. First, its cross-sectional design prevents causal inference between risk perception, social contact, and isolation. Given the link between social isolation and mental health, 28 future research should adopt longitudinal approaches. Second, self-reported telephone surveys may introduce response bias. While common in similar research, using multiple data sources in future studies would improve reliability. Third, the study did not account for the duration of social isolation, which significantly affects stress and mental well-being. 29 Future research ought to examine how isolation length interacts with risk perception. Finally, the study used two unvalidated questions to assess risk perception. Developing standardized, validated tools and conducting large-scale studies would enhance future findings.
Conclusion
This study is among the first in South Korea to examine the interplay between face-to-face and non-face-to-face social interactions, social isolation, and risk perception during the COVID-19 pandemic. Our nationally representative sample provided insights into how individuals adapted their social behaviors in response to perceived threats. In addition, this study clarified how government-led social distancing measures affected mental health and social adaptation across different demographic groups.
The findings also have practical implications for public health policies. Interventions supporting individuals with high risk perceptions by providing alternative methods of social connection must be developed. European and North American Studies have shown that social isolation increases hospitalization risks and worsens health conditions, particularly for those with pre-existing illnesses. 30 Identifying vulnerable groups and implementing strategies to reduce their sense of isolation can improve overall well-being.
Supplemental Material
sj-docx-1-aph-10.1177_10105395251364942 – Supplemental material for Relationship Between COVID-19 Risk Perception and Face-To-Face and Non-Face-To-Face Social Isolation During COVID-19: Risk Perception and Social Isolation during COVID-19
Supplemental material, sj-docx-1-aph-10.1177_10105395251364942 for Relationship Between COVID-19 Risk Perception and Face-To-Face and Non-Face-To-Face Social Isolation During COVID-19: Risk Perception and Social Isolation during COVID-19 by Yookyung Eoh, Jiwon Baek, Deok Hyun Jang and Won Mo Jang in Asia Pacific Journal of Public Health
Footnotes
Ethical Considerations
This study was reviewed and approved by the Institutional Review Board (IRB) of the Seoul Metropolitan Government, Seoul National University Boramae Medical Center (IRB No. 20-2022-21). The need for informed consent was waived by the IRB because the data were analyzed anonymously.
Author Contributions
Research conception and design: all authors; Investigation and formal analysis: JB and DHJ; Methodology: all authors; Drafting of the manuscript: all authors; Supervision: WMJ; Writing—review and editing and approval of final manuscript: all authors.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: For this study, JB was supported by the Basic Science Research Program through the National Research Foundation of Korea (NRF), funded by the Ministry of Education (NRF-2022R1I1A1A01071924).
Declaration of Conflicting Interests
Data Availability Statement
The authors will provide access to the anonymized dataset upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.