
Abstract
The Orang Asli, the indigenous community of Peninsular Malaysia, experience significant health disparities. This study assesses the prevalence and factors associated with poor self-rated health (SRH) among adults aged 18 and above using data from the Orang Asli Health Survey 2022. The prevalence of poor SRH was 12.8% (95% CI: [9.74, 16.68]). Factors associated with poor SRH are health-related factors (acute illness [adjusted odds ratio, aOR = 4.61, 95% CI: [3.54, 5.99]], recent hospitalization [aOR = 2.58, 95% CI: [1.78, 3.74]]), sociodemographic (unemployment [aOR = 1.51, 95% CI: [1.30, 1.76]], older age [aOR = 0.43, 95% CI: [0.30, 0.64]], and the Negrito tribes [aOR = 0.61, 95% CI: [0.37, 0.99]]) as well as lifestyle (tobacco use [aOR = 1.26, 95% CI: [1.03, 1.53]]). These findings underscore the importance of integrated health and social interventions sensitive to Orang Asli beliefs to improve health equity.
What We Already Know
Self-rated health is a globally valuable common indicator of health and well-being of a population, which is collected regularly from the series National Health and Morbidity Survey in Malaysia—subpopulation analysis for the Orang Asli population; however, it is implied to have limited reliability due to its high degree of variability and should be interpreted with caution.
Indigenous populations, including the Orang Asli, are known to experience health disparities and often report worse self-rated health than national averages due to socioeconomic and cultural factors.
Previous studies that focused on the Orang Asli population in Malaysia have described the factors that influence their health status, but these studies tend to be localized to specific regions or localities and lack a comprehensive overview of the Orang Asli population in Malaysia.
What This Article Adds
This study identifies the factors that influence poor self-rated health, which was synthesized from the Orang Asli Health Survey, the first nationwide cross-sectional survey among the Orang Asli population in Malaysia.
Global assumptions on indigenous populations reporting poorer self-rated health than their national averages are challenged, highlighting the importance of considering worldviews when interpreting the indigenous population’s health status.
Several key factors of poor self-rated health were identified, highlighting the disadvantages faced by the Orang Asli population to be abreast with broader socioeconomic development.
Introduction
The indigenous population, despite their rich heritage, often faces significant health disparities compared to the general population. The Orang Asli, the indigenous population of Peninsular Malaysia, account for about 0.8% of the Malaysian population.1 -3 Traditionally, they used to live in relatively small, remote villages and survive by traditional harvesting, fishing, or hunting. These days, they are no longer completely isolated from external cultural and economic influence due to urbanization, governmental regulation, and the market economy.4,5 For example, the planned resettlement programs such as Rancangan Penempatan Semula by the government provided Orang Asli communities in Malaysia with housing infrastructure, clean water and electricity, schools, and health facilities at the margins of towns. 6 Despite this progress, they often still come from poorer socioeconomic backgrounds, and the debate on the loss of cultural preservation has led to speculations about whether these factors have caused poorer health outcomes. 2
Self-rated health (SRH) is a composite measure of overall well-being, as it integrates the physical, mental, and social aspects of an individual.7 -11 The World Health Organization recommends SRH as a valuable indicator for health monitoring, as it has been able to predict and measure health outcomes that range from morbidity and mortality to functional limitations in various populations, including the indigenous population.12,13 Multiple studies have highlighted that the prevalence of poor SRH among different populations in Malaysia is influenced by factors that include socioeconomic, lifestyle choices, access to health care, disease burden, and environmental conditions. 14
However, the socioeconomic factors that influence the general population’s SRH might not be the same for the indigenous population, and the availability of health information solely for the Orang Asli is limited and often ingrained within national statistics. This prevents us from comprehensively understanding the health status of this population. Prior literature indicates that for many indigenous populations, health perceptions are influenced by concepts of social cohesion for self-identity and broader cultural underpinnings. 15 While these constructs were not measured in this study, acknowledging this provides a theoretical context for interpreting SRH among the Orang Asli population. By understanding health factors among the Orang Asli population, a starting point can be established in understanding their health status and health care utilization patterns. The curation of targeted interventions for their needs based on these factors would translate to better health outcomes for this population, especially for those who rate their health as poor. Therefore, this study aims to address this gap by assessing the prevalence and factors of poor SRH among the Orang Asli adult population in Malaysia.
Methods
Study design and sample
Data for this study were obtained from the Orang Asli Health Survey (OAHS) 2022, a cross-sectional population-based survey that employed a complex survey design with stratified cluster random sampling and sampling weights. The primary stratum comprises three localities, namely urban, fringe and remote. The secondary stratum comprised three main tribes (Senoi, Proto-Malay, or Negrito). Samples were selected from each tribe according to their localities. The OAHS’s detailed methodology and sampling design are available elsewhere. 16 A total of 9225 Orang Asli adults aged 18 years and over participated in the survey. In this study, only data from respondents with complete responses on potential factors and SRH status were included. The proportion of missing data was 2.2% (n = 204), and the missing data of less than 5% was acceptable for complete case analysis. 17 When a preliminary analysis of all respondents was conducted, including those with missing data, no differences in results were observed.
Data Collection
The data collection was conducted from July to September 2022 via face-to-face interviews by trained data collectors using a structured and validated questionnaire prepared in Malay, along with a questionnaire manual and codebook for data collectors. An additional vocabulary of common terminologies used by the Orang Asli was prepared to assist data collectors to ease the interview process. The survey’s overall response rate was 83.4%.
Study Variables
Dependent (outcome) variable
The outcome variable was SRH. Respondents were asked to self-report their perception of their current overall health condition at the point of the interview using a 5-point Likert-type measure (excellent, good, fair, poor, very poor). For analysis purposes, the responses were collapsed into two categories: good (excellent, good) and poor (fair, poor, very poor). In the logistic regression analysis, “good” was used as the reference category. 14
Independent variables
Demographic variables that were included were sex (male or female); locality (urban or fringe or remote); Orang Asli tribes (Senoi, Proto-Malay, or Negrito); age groups (a continuous variable that was grouped into 18-39 years old, 40-59 years old, and 60 years old and over); marital status (unmarried/divorced/widowed or married/living with a partner); and education levels (no formal education, primary or secondary education). Socio-economic variables included working status (measured whether the individual was working within one month at the point of the interview; working, homemakers, and students; not working); household income (calculated based on the total monthly household income; grouped into less than MYR 1000 or MYR 1000 and over). Proxy measures for health needs included were self-reported acute illness in the last two weeks prior to interview; the presence of any known diabetes, hypertension, or hypercholesterolemia diagnosed by health care practitioners; and newly diagnosed non-communicable diseases (NCDs). The responses from these health conditions were grouped as having “presence of any known non-communicable disease” or “none,” as well as “presence of any unknown non-communicable disease” or “none.” Lifestyle behaviors (alcohol consumption and smoking) were included in analysis, where the history of current tobacco and alcohol use was taken as a “yes” response. Furthermore, outpatient health care utilization was assessed by the use of clinics or hospitals without an overnight stay in the last 12 months, and inpatient health care utilization was assessed by their hospital admission in the last 12 months.
Data Analysis
A complex sample design was applied in all analyses to account for the survey’s sampling weight and clustering. Respondents’ characteristics were described using descriptive statistics. The prevalence and 95% confidence intervals (CI) of poor SRH among the Orang Asli adult population were calculated. Univariate and multivariable logistic regression were employed to assess the factors of poor SRH. Both theoretical and statistical criteria were employed for selecting variables included in the final regression model. 18 The adjusted odds ratio (AOR) with 95% CI from the logistic model was presented. Area under the curve (AUC) and receiver operating characteristic curve (ROC) were used to evaluate the sensitivity of the model, with a value of more than 0.7 indicating a good accuracy in predicting the outcome. 19 The multicollinearity was examined using VIF (Variance Inflation Factor). A VIF of more than 10 indicates a potential problem with multicollinearity. 20 The classification table was assessed to conclude that the overall correctly classified percentage was good if it was above 70%. 21 P-values < .05 were considered statistically significant. Analyses used Stata version 18.0 (StataCorp, College Station, Texas) software.
Ethical Approval and Informed Consent Statements
This study was registered under the National Medical Research Register (NMRR) under the registration number NMRR-19-3108-50999, approved by the Medical Research and Ethics Committee (MREC) of the Ministry of Health Malaysia (MOH) on December 18, 2019 (Ref: KKM/NIHSEC/P19-2592(11)), and funded by the MOH Research Grant warrant number 91000321. Approval from the Department of Orang Asli (JAKOA) Malaysia and relevant local authorities was obtained before conducting data collection. The tenets of the Declaration of Helsinki were followed during the study. Informed consent was obtained from respondents’ prior interview. The authors declare no conflict of interest in any form, including with the funders, in design, data collection, data analysis, or writing of the manuscript.
Results
The characteristics of the respondents are shown in Table 1. Overall, 9021 respondents representing 105 553 Orang Asli adult populations were included in the analysis.
Characteristics of Study Respondents (n = 9021).
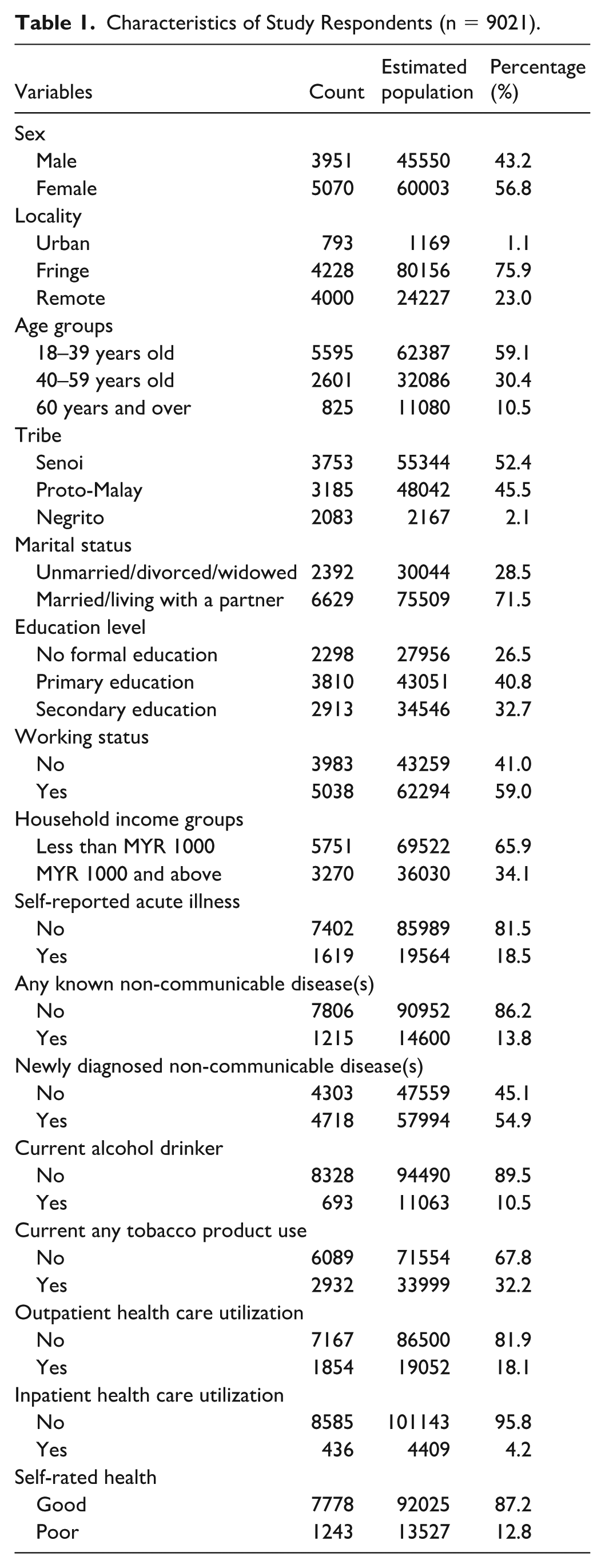
Table 2 presents the prevalence of Orang Asli adults who self-rated their health as poor and their factors. The overall prevalence of poor SRH was 12.8% (95% CI: [9.74, 16.68]), of which urban dwellers (37.1%, 95% CI: [30.50, 44.16]) have a higher prevalence than those dwelling in other localities. The Proto-Malays, who are mostly residing in urban localities, showed the highest prevalence of poor SRH (17.4%, 95% CI: [13.08, 22.70]). As age increases, poor SRH is more prevalent, where the highest prevalence found among those aged 60 years and over. Those of lower education levels up to primary education, lower salaries (less than MYR 1000), and not working showed high prevalences of poor SRH. The rate of poor SRH was also found to be highest among those who had self-reported illness (32.0%, 95% CI: [26.09, 38.46]), among those who had the presence of any NCDs (22.5%, 95% CI: [17.00, 29.17]), among users of outpatient health care services (20.3%, 95% CI: [14.38, 27.78]), and inpatient health care (30.3%, 95% CI: [22.04, 40.16]).
Prevalence of Self-Reported Poor Health, Among the Orang Asli Adult Population in Malaysia (n = 1243).
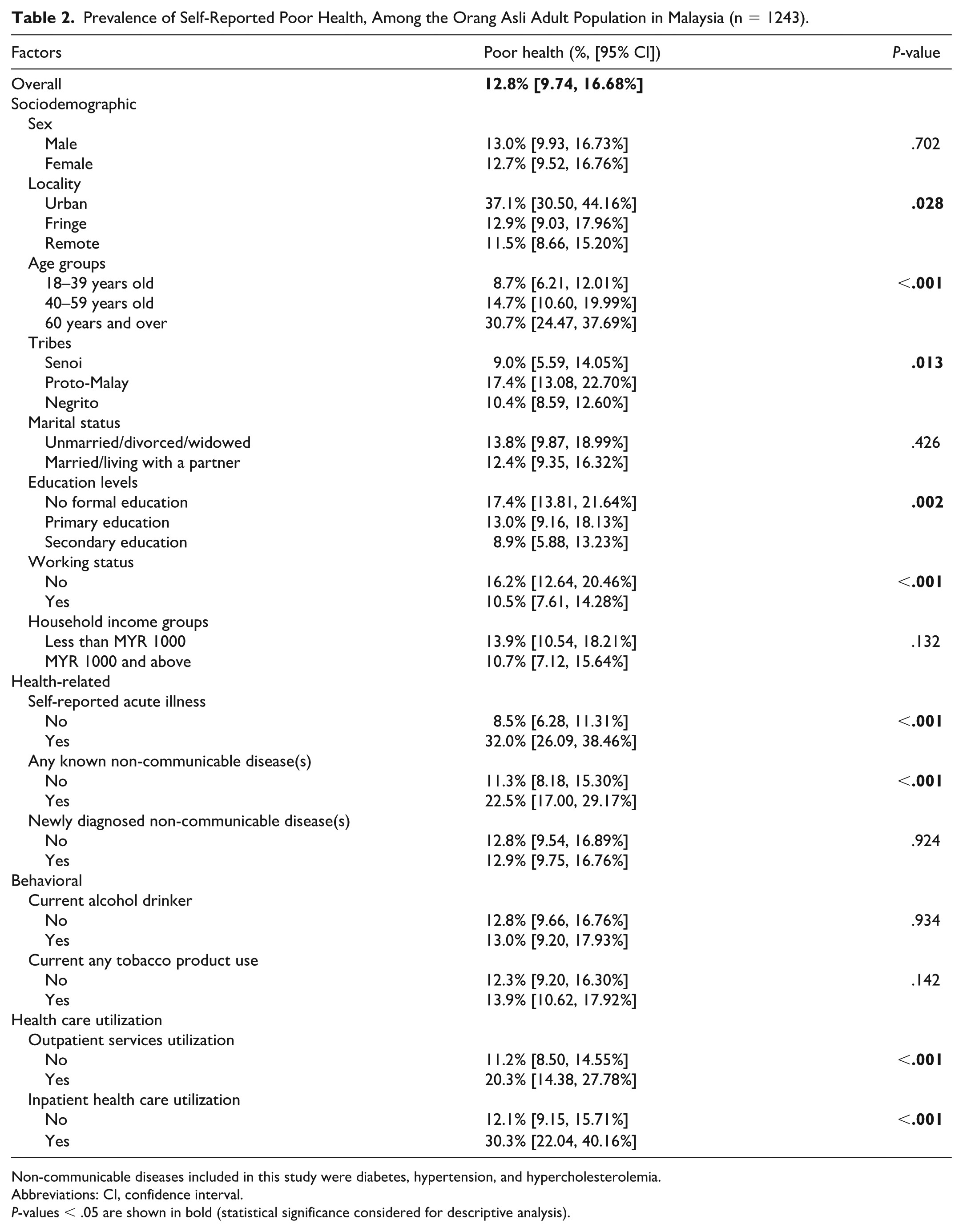
Non-communicable diseases included in this study were diabetes, hypertension, and hypercholesterolemia.
Abbreviations: CI, confidence interval.
P-values < .05 are shown in bold (statistical significance considered for descriptive analysis).
In Table 3, multivariable logistic regression analysis revealed that Orang Asli adults who live in urban areas were 2.63 times (AOR = 2.63, 95% CI: [1.63, 5.24], P = .007) more likely to self-report their health status as poor, while younger age groups (P < .001) and the Negrito tribe (AOR = 0.61, 95% CI: [0.37, 0.99], P = .047) showed less likelihood of poor SRH. Those who are not working were 1.51 times (AOR = 1.51, 95% CI: [1.30, 1.76], P < .001), and those with acute illness showed four times (AOR = 4.61, 95% CI: [3.54, 5.99], P < .001) more likelihood of poor SRH. Other factors found were current smokers (AOR = 1.26, 95% CI: [1.03, 1.53], P = .022) and utilization of inpatient health care services (AOR = 2.58, 95% CI: [1.78, 3.74], P < .001).
Multivariable Logistic Regression of Self-Reported Poor Health, among the Orang Asli Adult Population in Malaysia (n = 1243).
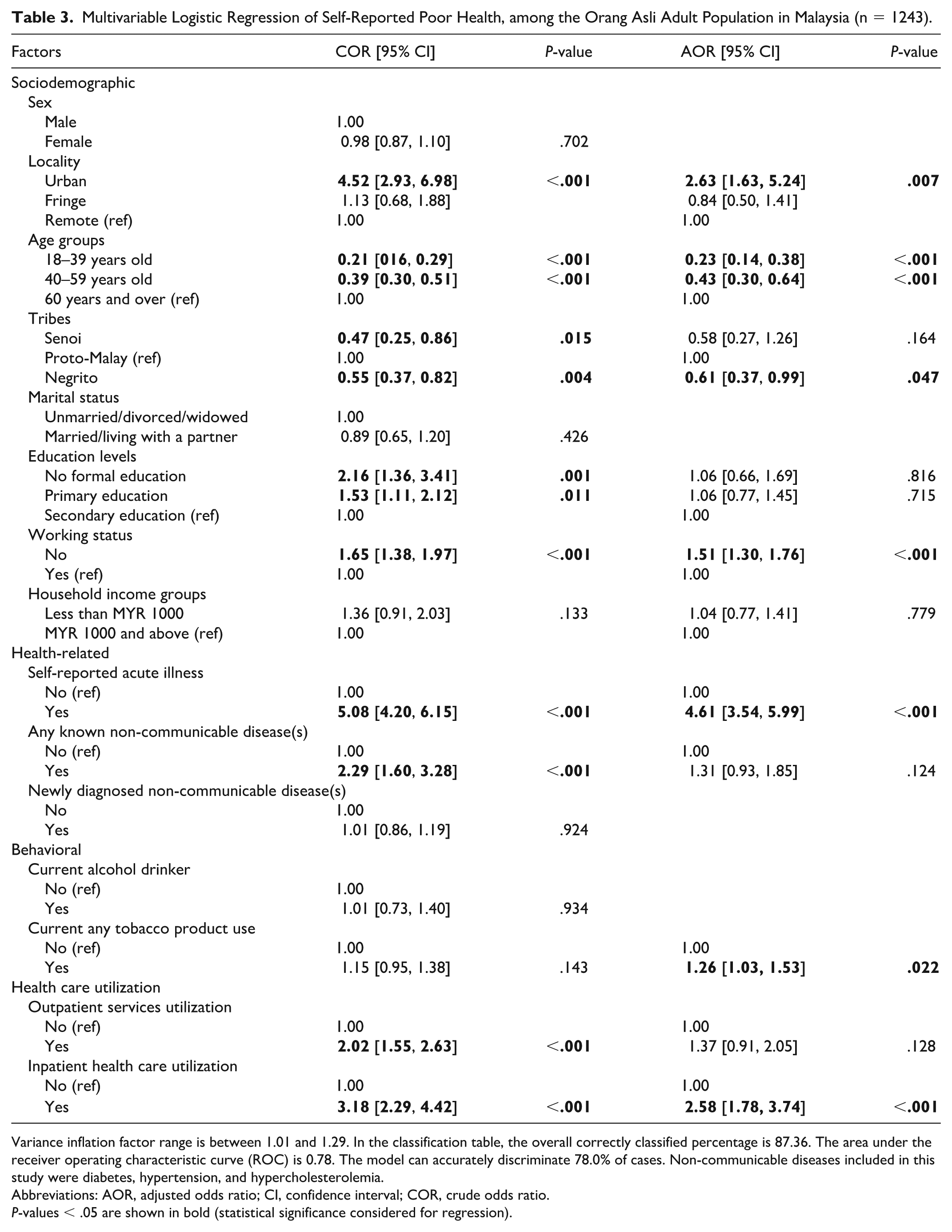
Variance inflation factor range is between 1.01 and 1.29. In the classification table, the overall correctly classified percentage is 87.36. The area under the receiver operating characteristic curve (ROC) is 0.78. The model can accurately discriminate 78.0% of cases. Non-communicable diseases included in this study were diabetes, hypertension, and hypercholesterolemia.
Abbreviations: AOR, adjusted odds ratio; CI, confidence interval; COR, crude odds ratio.
P-values < .05 are shown in bold (statistical significance considered for regression).
Discussion
The findings from this study illustrate several key factors influencing SRH among the Orang Asli community in Malaysia. These include locality, age, tribe, working status, self-reported illness, smoking status, and inpatient health care utilization. Overall, Orang Asli adults tend to rate their health better (12.8% reported poor SRH) than the general Malaysian population (15.8% reported poor SRH). 22 Most global studies report worse SRH among the indigenous community compared to national averages.13,23 -25 While literal comparisons of poor SRH cannot be made due to methodological differences between surveys, prior literature has indicated that distinctive cultural perspectives contribute to their holistic perspective toward health.3,5,10,11,15,24,25 Although these cultural nuances were not measured in this study, they provide useful context for interpreting why SRH factors among Orang Asli differ from the general population.
A notable finding from our study is the higher prevalence of poor SRH in urban areas that was represented by the Proto-Malay subgroup, as Senoi and Negrito respondents were not represented in urban settings. While rural localities are often associated with poorer health outcomes among the indigenous population in many countries, 13 our results suggest that urban-dwelling Proto-Malay folks may experience greater challenges. Factors such as increased stress and discrimination, compounded by limited access to well-paying jobs, may negatively impact their SRH. 10 In addition, we find that those who work associate themselves with having better SRH. Many indigenous communities worldwide observe similar trends with working status and better SRH, as being formally employed provides financial stability.2,10,13,24 Notably, most of our respondents were women who were homemakers—a category that was classified as not working. Evidence posits that women generally tend to rate their health lower, and this may have influenced the overall SRH findings. 10
Lifestyle factors such as smoking also significantly impact SRH. Evidence strongly links tobacco use to poorer health ratings, and in Malaysia, where current tobacco use prevalence is 19%, similar trends are observed among the Orang Asli community.16,23 Interestingly, despite evidence indicating a higher prevalence of NCDs among Orang Asli due to lifestyle factors, 16 our study demonstrated that almost one in three Orang Asli who reported an acute illness rated their health as poor (32.0%), and it remained a significant factor associated with poor SRH in our further analysis. Functional limitations and discomfort from conditions such as fever and pain might pose a greater immediate threat to perceived health than well-managed chronic diseases. 23 However, hospitalizations—a possible indicator of poorly controlled chronic conditions—are significantly associated with poorer SRH ratings. This could be due to the financial burden and loss of autonomy experienced during hospitalization, as it disrupts daily activities. 10
Our findings indicated two protective factors against poor SRH. Younger age, consistent with evidence from other general and indigenous populations, was linked with better SRH, which is typical as health perceptions generally decline with aging. The protective effect of the Negrito tribe is particularly interesting, as it challenges assumptions about indigenous populations universally reporting poorer health. It highlights the importance of considering unique worldviews and cultural factors when interpreting health status among indigenous groups. Education and income, which commonly emerge as significant predictors of SRH among the indigenous population, were not significant in this study.10,12,13 Possible reasons for this finding might be due to the aggregation of Orang Asli at the lower end of these categories, which might hinder contrasts across groups and detectable associations in the analysis.
The multifactorial nature of poor SRH among Orang Asli suggests that strategies to improve health outcomes should address not only health-related needs but also underlying social and behavioral factors. Expanding primary care and community-based services to minimize preventable admissions and developing culturally appropriate health education materials for smoking cessation and chronic disease management are practical strategies that could be adopted. 2 In addition, employment support programs could help mitigate the socioeconomic disparities faced by Orang Asli. By ensuring that outreach efforts are tailored to the beliefs and contexts of Orang Asli communities, SRH and overall well-being may be improved.
This is the first nationally representative study exploring factors of poor SRH among Orang Asli using OAHS data, providing valuable evidence for targeted health equity initiatives. However, as a cross-sectional and self-reported study, it is subject to recall bias, and causal inferences cannot be made. In addition, SRH is a subjective measure influenced by cultural perceptions, genetic predisposition, and environmental influences, and this study was not specifically designed to isolate SRH factors. Proxy measures of NCD burden, such as hypertension and diabetes, were used in the analysis instead of a comprehensive measure that includes other chronic conditions such as cancer, chronic obstructive pulmonary disease (COPD), stroke, and mental health, due to limitations in the data collected in the survey. Future research employing longitudinal studies and mixed-method approaches that explore cultural perspectives alongside health and socioeconomic conditions would be beneficial in fully understanding the factors influencing SRH and the actual health conditions within this community.
Conclusion/Recommendation
This study identifies the health-related, sociodemographic, and behavioral factors associated with poor SRH among Orang Asli adults in Malaysia. Urban locality, unemployment, acute illness, smoking, and hospitalization were factors associated with poor SRH, whereas younger age and those from the Negrito tribe were protective factors. These findings provide evidence to develop targeted interventions that address medical, social, and behavioral factors to bridge the gap between perceived health and actual health outcomes for the Orang Asli community.
Footnotes
Acknowledgements
The authors would like to thank the Director General of Health, Malaysia, for his permission to publish this article.
ORCID iDs
Ethical Considerations
This study was registered under the National Medical Research Register (NMRR) under the registration number NMRR-19-3108-50999, approved by the Medical Research and Ethics Committee (MREC) of the Ministry of Health Malaysia (MOH) on December 18, 2019 (Ref: KKM/NIHSEC/P19-2592(11)), and funded by the MOH Research Grant warrant number 91000321. Approval from the Department of Orang Asli (JAKOA) Malaysia and relevant local authorities was obtained before conducting data collection. The tenets of the Declaration of Helsinki were followed during the study.
Informed Consent Statements
Informed consent was obtained from respondents before the interviews. The authors declare no conflict of interest in any form, including with the funders, whether in the design, data collection, data analysis, or writing of the manuscript.
Author Contributions
SNMN, DSRM, NEAM, IAR, SJ, JAH, AM, and AAN: Conceptualization.
JAH, IAR, TAS, and MAAR: Data curation.
SNMN, NEAM, DSRM, SJ, and JAH: Formal analysis.
JAH, TAS, and MAAR: Investigation.
SNMN, DSRM, SJ, and NEAM: Methodology.
IAR: Project Administration.
AAN and AM: Validation.
SNMN, DSRM, and NEAM: Writing—original draft.
SNMN, DSRM, NEAM, IAR, SJ, JAH, AM, and AAN: Writing—review & editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This survey was funded by the Ministry of Health Malaysia research grant.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data supportting this study are available from the Institute for Public Health, Ministry of Health Malaysia, but access is restricted as the data are not publicly available. They can be obtained upon reasonable request and with permission from the Director General of Health Malaysia.