
Abstract
While COVID-19-related stigma perception is recognized as a mental health risk, its effects on the general population are understudied. This study examined the link between stigma perception and symptoms of anxiety disorder among the general population in South Korea. This study used data from a nationwide survey, the Korean National Mental Health Survey related to COVID-19. Anxiety symptoms were measured using the Generalized Anxiety Disorder 7-item scale (GAD-7). Stigma perception was assessed with a single question and categorized as “No,” “Yes,” or “Strongly Yes.” Logistic regression was used, adjusting for demographic, socioeconomic, COVID-19-related, and health-related factors. Results showed that 12.7% of respondents met the criteria for anxiety disorder. Compared with those who perceived no stigma, individuals who answered “Yes” had 2.12 (95% CI [1.31, 3.46]) times higher odds of anxiety, and those who answered “Strongly Yes” had 6.61 (95% CI [3.75, 11.62]) times higher odds. Other significant factors included marital status, lower income, worsened economic conditions during the pandemic, subjective stress, poor sleep quality, and underlying health conditions. These findings suggest that stigma perception related to COVID-19 is a strong and independent risk factor for anxiety. Public health interventions should incorporate anti-stigma strategies to support mental health during and beyond pandemic.
What We Already Know
The COVID-19 pandemic has profoundly affected individuals’ mental health globally, leading to an increase in the incidence of anxiety.
COVID-19-related stigma perception has been associated with adverse mental health outcomes, including anxiety, in studies focusing mainly on individuals infected with COVID-19.
What This Study Adds
This study was the first to examine the association between COVID-19-related stigma perception and anxiety in the Korean general population using nationally representative data.
The results of this study revealed a strong, dose-dependent positive association between the level of stigma perception and the odds of experiencing significant anxiety symptoms, even after adjusting for demographic, socioeconomic, COVID-19-related, and health-related (mental and physical) factors.
Introduction
The COVID-19 pandemic placed a significant burden on public health systems around the world and had a negative impact on the mental health of various populations.1,2 Numerous studies have reported higher levels of anxiety, depression, and mental distress during the pandemic.3-6 Previous studies have indicated that anxiety symptoms exhibited the highest prevalence among various mental health outcomes. 7 In South Korea, similar trends have been observed. A national mental health survey conducted in March 2020, during the first wave of the pandemic, reported that 48% of the population experienced feelings of anxiety related to COVID-19. The situation worsened in the following year, with the 2021 national survey indicating that 55.8% of respondents reported feelings of anxiety. Moreover, the rate of suicidal ideation increased to 12.7% in 2022, nearly three times higher than the 4.6% recorded in 2019, before the pandemic.8,9 These circumstances have led experts to emphasize the need for interventions to prevent a “mental-demic,” a phenomenon in which psychological impacts or trauma spread across society like an epidemic in response to the COVID-19 pandemic.8,10,11
Various studies have been conducted on mental health issues related to the COVID-19 pandemic, and a range of risk factors, including demographic characteristics, socioeconomic conditions, pandemic-related factors, and psychosocial determinants, have been identified. Among these determinants, stigma perception is one of the most important factors. It is conceptualized as a multidimensional process involving negative perceptions and attitudes toward specific groups, including labeling, stereotyping, separation, status loss, and discrimination. 12 Past infectious disease outbreaks have demonstrated that stigma acts as an exacerbating factor for individual psychological distress, extending beyond the fear of infection itself through mechanisms such as fear of social judgment, relationship withdrawal, and reduced access to health and social.13-15 Because of this, the World Health Organization (WHO) emphasized that anti-stigma strategies should be included as part of efforts to protect mental health during the pandemic. 16
Several studies have reported associations between COVID-19-related stigma perception and both depressive symptoms and anxiety.7,15,17 However, since these previous studies were conducted primarily on individuals infected with COVID-19, the association between stigma perception and mental health within the general population remains unclear. Even though South Korea was one of the first countries in the world to experience the pandemic, there has been no research on the status of COVID-19-related stigma perception and its impact on mental health in the general population during the pandemic. This study aimed to examine the association between stigma perception related to COVID-19 and symptoms of anxiety disorder in the general population, using nationwide survey data from South Korea.
Methods
Data Source
This study used raw data from the Korean National Mental Health Survey related to COVID-19 (KNMHS-Cov19). The KNMHS-Cov19 assessed the mental health status of Korean adults aged 19 and older during the COVID-19 pandemic, encompassing all 17 provinces across the country. A stratified random sampling method with proportional allocation was applied based on sex, age, and region to select participants aged 19 years and above. The survey was administered online in March 2021, approximately one year after the onset of the COVID-19 outbreak in South Korea and included a total of 2000 respondents. 18
Variable Definition
Anxiety severity was measured using the Generalized Anxiety Disorder 7-item scale (GAD-7), a brief and widely validated screening instrument suitable for diverse settings. The GAD-7 comprises seven items rated on a four-point Likert scale, assessing the frequency of anxiety symptoms over the past two weeks, with total scores ranging from 0 to 21. A score of 10 or higher, indicating moderate to severe anxiety, has demonstrated a sensitivity of 89% and specificity of 82%. 19 Accordingly, this study adopted a cut-off score of ≥10 to define the presence of an anxiety disorder.
The primary variable of interest, “stigma perception,” was assessed by asking participants, “Do you think there is social stigma perception toward individuals confirmed with COVID-19 in our society?” Responses were categorized into three groups: “No,” “Yes,” and “Strongly Yes.” This study also accounted for several potential confounding variables, including demographic characteristics (e.g., sex and age); socioeconomic factors (e.g., marital status, education level, and annual household income); COVID-19-related factors (e.g., changes in economic status during the COVID-19 pandemic, and subjective stress caused by COVID-19, both measured using a five-point Likert scale); mental health factors (e.g., sleep quality during the pandemic, measured on a five-point Likert scale); and health-related factors (e.g., underlying conditions). All these variables were included in the final analytical model. For analysis, the five-point Likert scale responses were recategorized. In terms of changes in economic status during the pandemic, responses of “significantly improved,” “improved,” and “similar” were grouped as “similar or better,” whereas “worsened” and “significantly worsened” were classified as “worse.” Regarding subjective stress caused by COVID-19, responses of “very severe” and “severe” were grouped as “yes or severe,” and “not at all,” “not severe,” and “moderate” were grouped as “not severe or moderate.” Also, sleep problem during the pandemic, responses of “significantly improved,” “improved,” and “similar” were considered “similar or better,” whereas “worsened” and “significantly worsened” were classified as “worse.”
Statistical Analysis
Group differences in anxiety prevalence across general characteristics were assessed using chi-square tests. To evaluate the primary study objective—examining the association between stigma perception and anxiety—logistic regression analysis was conducted. All statistical analyses were performed using STATA version 14, with a significance level set at α = .05.
Results
Among the 2000 participants, 253 (12.7%) were classified as having anxiety. The prevalence of anxiety was significantly higher among individuals who had stigma perception related to their COVID-19 infection compared with those who did not. Specifically, the prevalence rates of anxiety were 5.0%, 12.1%, and 33.9% among those who responded “No,” “Yes,” and “Strongly Yes,” respectively, to the question on stigma perception (Table 1).
Prevalence of Anxiety According to the General Characteristics of the Study Sample (n = 2000).
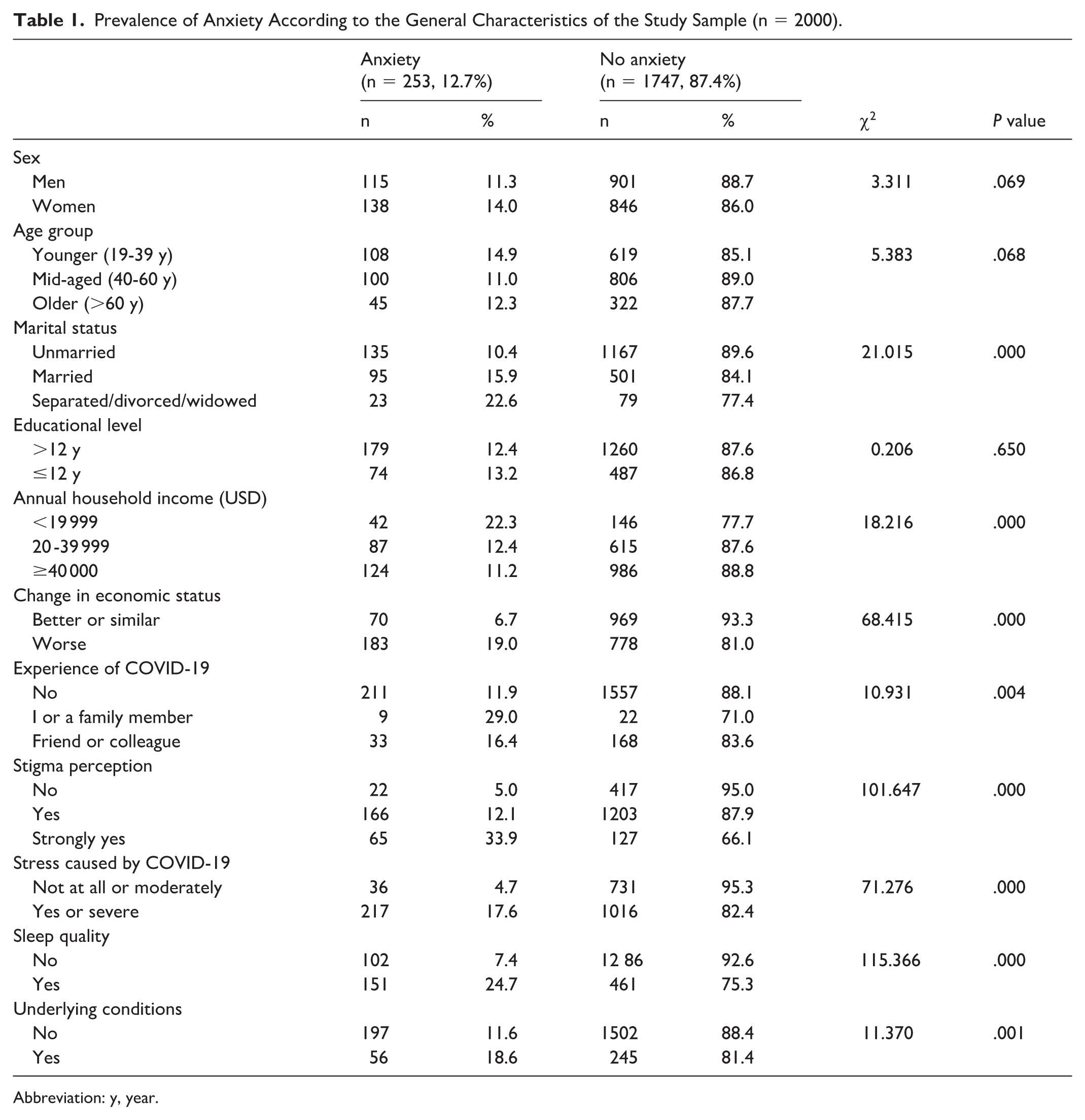
Abbreviation: y, year.
Table 2 presents the factors associated with anxiety. Participants who reported stigma perception had 2.12 times higher odds of experiencing anxiety than those who did not report stigma perception (95% confidence interval [CI] [1.31, 3.46]). In addition, those who strongly reported stigma perception (“Strongly Yes”) had 6.61 times higher odds of anxiety (95% CI [3.75, 11.62]).
Logistic Regression Results of the Association Between Stigma Perception and Anxiety (n = 2000).

Abbreviation: y, year.
Regarding socioeconomic characteristics, both marital status and annual household income were significantly associated with anxiety. Compared with married individuals, those who were unmarried (odds ratio [OR]: 1.53, 95% CI [1.05, 2.25]) or separated/divorced/widowed (OR: 2.44, 95% CI [1.37, 4.34]) had increased odds of anxiety. In terms of income, individuals with an annual household income less than 19 999 dollars (US) had significantly higher odds of anxiety (OR: 199, 95% CI [1.24, 3.17]) than those with an income more than 40 000 dollars (US).
Among COVID-19-related variables, both changes in economic status during the COVID-19 pandemic and subjective stress related to COVID-19 were significantly associated with anxiety. Individuals who reported a “worsened” economic status had significantly higher odds of anxiety compared with those whose status was “similar or better” (OR: 2.02, 95% CI [1.47, 2.78]). Similarly, participants reporting “yes/severe” subjective stress had higher odds of anxiety than those reporting “not at all/moderate” levels (OR: 2.60, 95% CI [1.75, 3.87]).
With respect to mental and physical health factors, both sleep quality during the pandemic and the presence of underlying conditions were significantly associated with anxiety. Participants who experienced “worsened” sleep quality had significantly higher odds of anxiety than those with “similar/better” sleep quality (OR: 2.55, 95% CI [1.88, 3.46]). In addition, those with “underlying conditions” had significantly greater odds of anxiety compared with those with “no underlying conditions” (OR: 1.65, 95% CI [1.13, 2.41]).
Discussion
This was the first study to investigate the association between COVID-19-related stigma perception and anxiety in the Korean general population. Furthermore, it might be the first to investigate this relationship in the general population using nationally representative data based on self-reported.
This study investigated the association between COVID-19-related stigma perception and anxiety among Korean adults, using data from a nationwide survey conducted approximately one year after the onset of the pandemic. The main finding revealed a strong, dose-dependent positive association between the level of stigma perception and the odds of experiencing significant anxiety symptoms, even after adjusting for demographic, socioeconomic, COVID-19-related, and health-related (mental and physical) factors. That is, individuals who reported stigma perception (“Yes”) had 2.12 times the odds of experiencing anxiety, whereas those who strongly perceived stigma (“Strongly Yes”) had 6.61 times the odds, compared with those who reported no stigma perception. This primary finding consistent with previous research reporting the negative impact of stigma perception on mental health during infectious disease outbreaks.7,13-15 Especially, according to the results of this study, COVID-19-related stigma perception can be a major cause of anxiety even among individuals who have not been infected. Also, the more strongly a person reports stigma perception, the more likely they are to experience anxiety. This result supports the notion that stigma perception contributes to psychological distress by operating through mechanisms such as fear of social judgment and social isolation. 12 Moreover, perceived stigma may accelerate the spread of disease by discouraging the disclosure of infection status. 7 It can be indirectly experienced and internalized through community attitudes, media portrayals, and broader societal discourses. This indirect stigma perception can impose a psychological burden, including anxiety, even on individuals without a history of infection. 20 Similarly, this study found that individuals who reported stigma perception toward themselves or others were more likely to experience negative mental health outcomes, such as anxiety, depression, and psychological distress. It is noteworthy that this perception of stigma can operate independently of actual infection status, implying it can exert widespread psychological effects even among the uninfected general population.
Consistent with existing literature on mental health during the pandemic, several other factors were significantly associated with anxiety in this study. Being unmarried or separated/divorced/widowed,18,21,22 lower household income,23,24 worsened economic status due to COVID-19,18,22 subjective stress from the pandemic, 25 worsened sleep quality, 26 and underlying conditions2,27 were all linked to increased odds of anxiety. These findings highlight those various factors—such as socioeconomic vulnerability, direct pandemic-related experiences, and physical health problems—contribute to anxiety during public health crises like the COVID-19 pandemic. Even after controlling these strong confounding variables, the association between stigma perception and anxiety remained robust, further confirming that stigma perception is an important risk factor.28,29
This study had several limitations. First, because this study used a cross-sectional design, it could not show whether stigma perception causes anxiety or vice versa. To better understand the direction of the relationship, future studies using a longitudinal approach are needed. Second, since the data were based on participants’ self-reports, there might be some bias; people might have underreported or overreported their experiences of stigma perception or anxiety. Third, although this study was adjusted for various confounding factors, other factors were not measured, such as existing mental health conditions or cultural attitudes toward stigma perception, could have affected the results. Lastly, since the data came from South Korea, the findings might not be able to apply to people in other countries or cultural and economic settings.
Despite these limitations, the study offers important implications. From a public health perspective, the findings underscore the urgent need to integrate anti-stigma strategies into pandemic preparedness and response plans, aligning with recommendations from the WHO. 16 Public health messaging should aim to counter misinformation, foster empathy, and promote supportive attitudes toward those affected by illness, directly or indirectly. This study’s findings can contribute to evidence-based policymaking focused on preserving public mental health in the context of future infectious disease outbreaks.
Conclusion
In conclusion, this study, based on nationally representative data from the general population in South Korea, highlights a strong association between COVID-19-related stigma perception and increased anxiety. Recognizing and combating stigma perception should be an integral component of comprehensive mental health support strategies during infectious disease outbreaks.
Footnotes
Ethical Considerations
The present study was approved (Number P01-202402-01-005) by the National Bioethics Committee of South Korea appointed by the Ministry of Health and Welfare.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.