
Abstract
The household double burden of malnutrition (DBM), where maternal overnutrition coexists with child undernutrition, is a concern in Malaysia, as adult obesity rises alongside child undernutrition. Local evidence focused on rural and indigenous populations, lacking studies in vulnerable urban communities. This study determined the prevalence, subtypes, and factors associated with household DBM among residents of low-cost housing communities in Kuala Lumpur. A cross-sectional survey was conducted from April to July 2024 among 346 households of children attending public early childhood education centres, using cluster random sampling. Data on sociodemographics, food security, dietary diversity, and anthropometry were collected and analysed with SPSS 29. Household DBM prevalence was 11.0%, predominantly among underweight children. Risk was higher with maternal short stature (aOR 2.80, 95% CI [1.01-7.76]) and higher child birth order (aOR 2.03, 95% CI [1.15-3.59]), while older maternal age was protective (aOR 0.84, 95% CI [0.74-0.96]). These findings support the need for integrated maternal and child nutrition strategies, guided by local data.
What We Already Know
The double burden of malnutrition (DBM) is increasingly recognised in low- and middle-income countries (LMICs) undergoing nutrition transition, where undernutrition and overnutrition coexist and are linked to long-term health consequences.
The most common household DBM subtype globally is an overweight or obese mother with a stunted child, though in several Asian contexts, it often involves underweight children.
Household DBM is reported in Malaysia’s rural and indigenous populations, with scarce evidence from urban low-cost housing communities.
What This Article Adds
Describes households in urban low-cost housing areas, showing high maternal education but low workforce participation, and other constraints that may shape household nutrition.
Provides local evidence of the prevalence of household DBM in urban low-cost housing communities, with the most common subtype being an overweight or obese mother with an underweight child.
Identifies maternal short stature and higher child birth order as risk factors for household DBM in urban low-cost housing communities, while older maternal age is protective. Findings can inform national policies addressing child undernutrition and adult overweight within households.
Introduction
The coexistence of undernutrition and overnutrition within individuals, households, and populations, known as double burden of malnutrition (DBM), is a global nutrition dilemma. Undernutrition was once linked to poverty and infection, while overnutrition was associated with affluence and sedentary lifestyles. These conditions now increasingly overlap, driven by dietary shifts towards processed, high-calorie food, less physical activity, urbanisation, and income inequality.1,2 The DBM imposes substantial health and economic burdens, particularly in low- and middle-income countries (LMICs), where infectious diseases, undernutrition, and obesity intersect, amplifying non-communicable diseases (NCD) risk such as type 2 diabetes, hypertension and cardiovascular diseases. 2 Globally, NCDs account for 41 million deaths annually, with 80% occurring in LMICs, where malnutrition exacerbates health care costs and hinders economic progress. 3
At the household level, DBM has been reported across diverse settings. A systematic review of 35 studies from 70 countries found prevalence up to 26.8%, with most involving a stunted or underweight child and an overweight mother. 4 In Indonesia, household DBM prevalence exceeds 25%, driven by rapid urbanisation and shifts in dietary patterns, 5 while lower prevalence has been observed in countries like Vietnam (3.7%) and the Kyrgyz Republic (15.5%). 4 Cross-country comparisons remain difficult due to methodological variation, highlighting the need for locally relevant data.
Malaysia has experienced a nutritional transition linked to urbanisation, globalised food systems, and changing lifestyles. 6 In 2023, more than half of Malaysian adults were overweight or obese, the highest in Southeast Asia. 7 Concurrently, childhood stunting doubled to 22% in 2019, with underweight and wasting rising to 15.3% and 9.9%, respectively. 8 Prior local studies among rural Malay and Indigenous populations identified household DBM prevalence between 20% and 38%, with underweight children more common in rural Malays and stunted children in Indigenous populations. Associated factors included maternal short stature, low maternal education, larger household size, food insecurity, and child characteristics such as younger age and male sex.9,10 These findings highlight DBM in disadvantaged communities, but evidence from urban low-cost housing remains limited, despite pressures from increased food prices, reliance on processed food, and dense urban living, reflecting broader changes in food environments observed in urban Asian settings. 11
Malaysia has introduced policy frameworks to address nutrition and health. The National Plan of Action for Nutrition of Malaysia III (2016-2025) seeks to reduce all forms of malnutrition, while the National Strategic Plan for Non-Communicable Diseases (2016-2025) prioritises reducing risk factors such as unhealthy diet, physical inactivity, and obesity-related conditions. Yet, DBM is addressed largely in parallel, with little focus on its coexistence within households. Therefore, the objectives of this study were to determine the prevalence, subtypes, and associated factors of household DBM in Kuala Lumpur’s low-cost housing communities, with the aim to generate evidence to support integrated child nutrition and NCD prevention strategies.
Methods
This cross-sectional study was conducted in Kuala Lumpur, the capital of Malaysia, which spans 243 km2 with an estimated population of 1.98 million. 12 The study population comprised mother-child pairs with children aged 2 to 6 years attending public early childhood education centres, which mainly serve low-cost housing communities. These are subsidised, high-rise residences for B40-income households under the National Housing Department. Eligible participants were mothers aged 18 to 49 years and their children who had lived in Kuala Lumpur for at least 12 months and were able to communicate in the Malay language or English. Pregnant and lactating mothers were excluded, as were those with mental or physical disabilities, together with their children.
The sample size was calculated as 310 participants, factoring in a 20% nonresponse rate to achieve 80% study power at a 95% confidence interval (CI). A cluster random sampling method was employed, selecting 42 centres from a sampling frame of 135 public early childhood education centres under the Department of National Unity and Integration in Kuala Lumpur, with approximately eight mother-child pairs included per cluster. Data collection involved questionnaires, face-to-face interviews, and anthropometric measurements.
Independent variables include sociodemographic factors such as parental age, education, and household income; infant feeding practices; food security; and dietary diversity. Infant feeding practices were assessed using two categorical indicators: breastfeeding status and age-appropriate complementary feeding. Breastfeeding status was defined as exclusive breastfeeding from birth until 6 months of age, 13 while age-appropriate complementary feeding referred to the timely introduction of food alongside breast milk or formula at 6 months. 14
Household food security was assessed using the Food Insecurity Experience Scale (FIES), a validated eight-item experience-based tool developed by the Food and Agriculture Organization (FAO). 15 Responses were analysed with Rasch modelling for SDG Indicator 2.1.2, applying FAO-calibrated thresholds for moderate-to-severe (−0.52) and severe (3.10) food insecurity. The model showed acceptable fit (Rasch reliability 0.74). Prevalence estimates were adjusted for a design effect of two and reported at the 90% CI, as per FAO protocol. 15
Household dietary diversity was evaluated through a 24-hour dietary recall for 3 days (two weekdays and one weekend). Responses were categorised into 12 food groups following FAO guidelines, and the mean score determined dietary diversity adequacy. 16
Anthropometric measurements included the weight and height of mothers and children using a Seca 217 stadiometer and a Seca 813 digital scale. The stadiometer measures from 20 to 205 cm with 1 mm graduation, and the scale supports up to 200 kg with 100 g increments on a wide, nonslip platform. Both instruments meet WHO recommendations for anthropometric assessment and are widely used in nutrition surveys. 17 Calibration was performed daily with a standard weight and ruler, and each measurement was taken twice and averaged to minimise error.
Children’s weight-for-age (WAZ), height-for-age (HAZ), weight-for-height (WHZ), and body mass index-for-age (BAZ) z-scores were calculated using WHO Anthro and WHO AnthroPlus software. The WAZ and HAZ were calculated for all children, whereas WHZ was only for those under 5 years old and BAZ for those aged 5 and above. Children were classified as undernourished if they were stunted (HAZ<−2 SD), underweight (WAZ<−2 SD), wasted (WHZ<−2 SD), or thin (BAZ<−2 SD) based on WHO reference standards. 17 For mothers, body mass index (BMI) was calculated as [weight (kg)]/[height (m)] 2 . The BMI cut-off used for overweight was 23 kg/m2 to < 25 kg/m2, and for obesity, it was ≥ 25 kg/m2. This was classified using the Asia-Pacific BMI Classification. 18
The outcome was defined as household DBM, comprising five forms. In all forms, the mother was either overweight or obese. The DBM was classified as an overweight or obese mother and underweight child (OWOB/U) when the child was underweight, overweight or obese mother and stunted child (OWOB/S) when stunted, overweight or obese mother and wasted child (OWOB/W) when wasted, and overweight or obese mother and thin child (OWOB/T) when thin. The overweight or obese mother and undernourished child (underweight, stunted, wasted or thin) (OWOB/USWT) referred to cases where the child had at least one form of undernutrition, namely underweight (U), stunting (S), wasting (W), or thinness (T).
Descriptive analyses summarised the study population and DBM prevalence. Categorical variables were presented as frequencies and percentages, while continuous variables were expressed as mean (SD) or median (IQR) after normality assessment. Missing data were minimal (<3.5%) and considered Missing Completely at Random (MCAR), based on a non-significant MCAR test. Pairwise deletion was applied for descriptive analyses and listwise deletion for multivariable models.
Logistic regression assessed associations between independent variables and household DBM (OWOB/USWT). Univariable analyses were first performed, and variables with a P value below .25 or theoretical relevance were retained in multivariable models. A hierarchical approach was applied, whereby variables were entered in blocks according to their conceptual grouping, with household characteristics included in the first block, followed by maternal characteristics in the second block and child characteristics in the final block. Variance inflation factor (VIF) values for all variables were below 5, indicating no multicollinearity. Model fit was evaluated using the Hosmer-Lemeshow test, classification tables, and the area under the receiver operating characteristic (ROC) curve.
Results
Baseline Characteristics
The study included 346 mother-child pairs, with baseline characteristics presented in Table 1. The median household size was five members (IQR 4, 6), with a median of three children (IQR 2, 4). Most households (n = 282, 81.5%) were from the B40-income group, while 16.8% were in the M40 category and only 1.7% in the T20 group. Mothers had a mean age of 35.2 years (SD = 5.6), and the majority were Malay (n = 306, 88.4%) and married (n = 326, 94.2%). Although nearly half of mothers (n = 162, 46.8%) had attained tertiary-level education, less than half were employed (n = 165, 47.7%). Fathers had lower proportions of tertiary education (n = 115, 34.1%) but were almost all employed (n = 329, 98.5%).
Baseline Characteristics of Study Population.
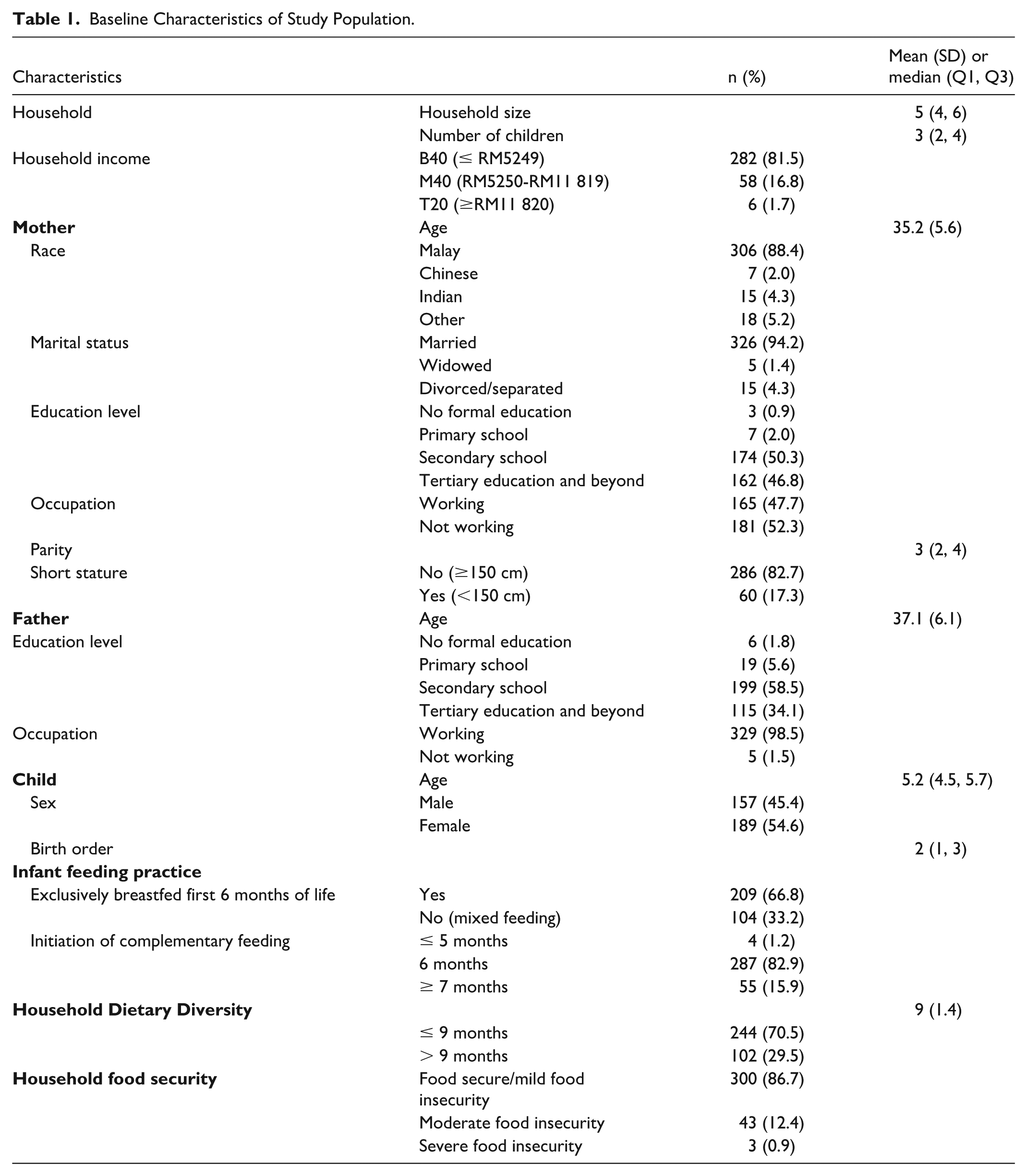
Children had a mean age of 5.2 years (IQR 4.5, 5.7), with a slightly higher proportion of girls (n = 189, 54.6%) compared to boys. The median birth order was two (IQR 1, 3). Infant feeding practices showed that 66.8% of children had been exclusively breastfed for the first 6 months, while one-third (n = 104, 33.2%) received mixed feeding. Complementary feeding was timely in most children (n = 287, 82.9%), whereas 1.2% received food earlier than 6 months and 15.9% later than 6 months. Regarding household dietary diversity, 70.5% of households recorded scores of nine or below and 29.5% scored above nine. Most households were food secure or mildly food insecure (n = 300, 86.7%), but 12.4% experienced moderate food insecurity and 3.0% reported severe food insecurity.
Anthropometric Measurements of Mothers and Children
Mothers had a median height of 155.0 cm (IQR 151.8, 158.8) and a median weight of 66.3 kg (IQR 56.1, 77.1), corresponding to a median BMI of 27.7 kg/m2 (IQR 23.4, 31.6). The majority of mothers were obese (n = 226, 65.3%), while 12.4% were overweight, 18.5% had normal weight, and 3.8% were underweight. According to WHO reference standards, 58 children (16.8%) were undernourished, whereby 41 children (11.8%) were underweight, 31 (9.0%) were stunted, 19 (9.6%) were thin, and 3 (2.0%) were wasted.
Prevalence of Household DBM
The overall prevalence of household DBM, defined as the coexistence of an overweight or obese mother with an undernourished child (OWOB/USWT), was 11.0%. The most frequent subtype was OWOB/U, observed in 8.4% of households. This was followed by OWOB/S at 5.5%, OWOB/T at 3.2%, and OWOB/W at 2.0%. These findings are presented in Figure 1.
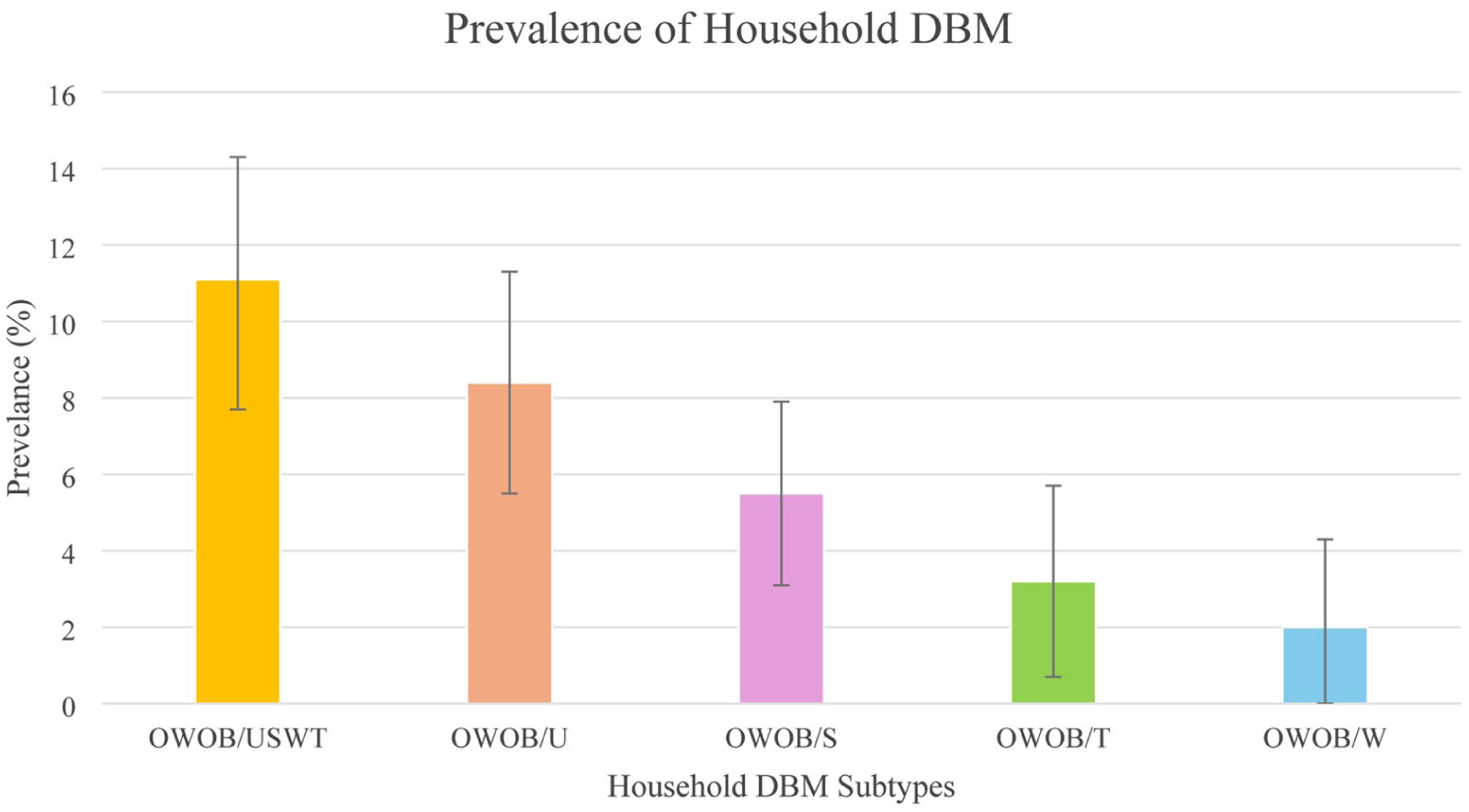
Prevalence of household DBM.
Factors Associated With Household DBM
Univariable and multivariable logistic regression analyses for factors associated with household DBM are presented in Table 2. In univariable analysis, among household characteristics, larger household size (OR 1.23, 95% CI [1.03-1.47]) and a greater number of children (OR 1.45, 95% CI [1.13-1.87]) were significantly associated with increased odds of DBM. For maternal characteristics, higher parity was linked to a greater risk (OR 1.20, 95% CI [1.00-1.42]). Among child characteristics, higher birth order was significantly associated with DBM (OR 1.33, 95% CI [1.09-1.64]).
Sociodemographic Characteristics, Household Food Insecurity, Household Dietary Diversity and Infant Feeding Practices Association With Household DBM Using Logistic Regression.
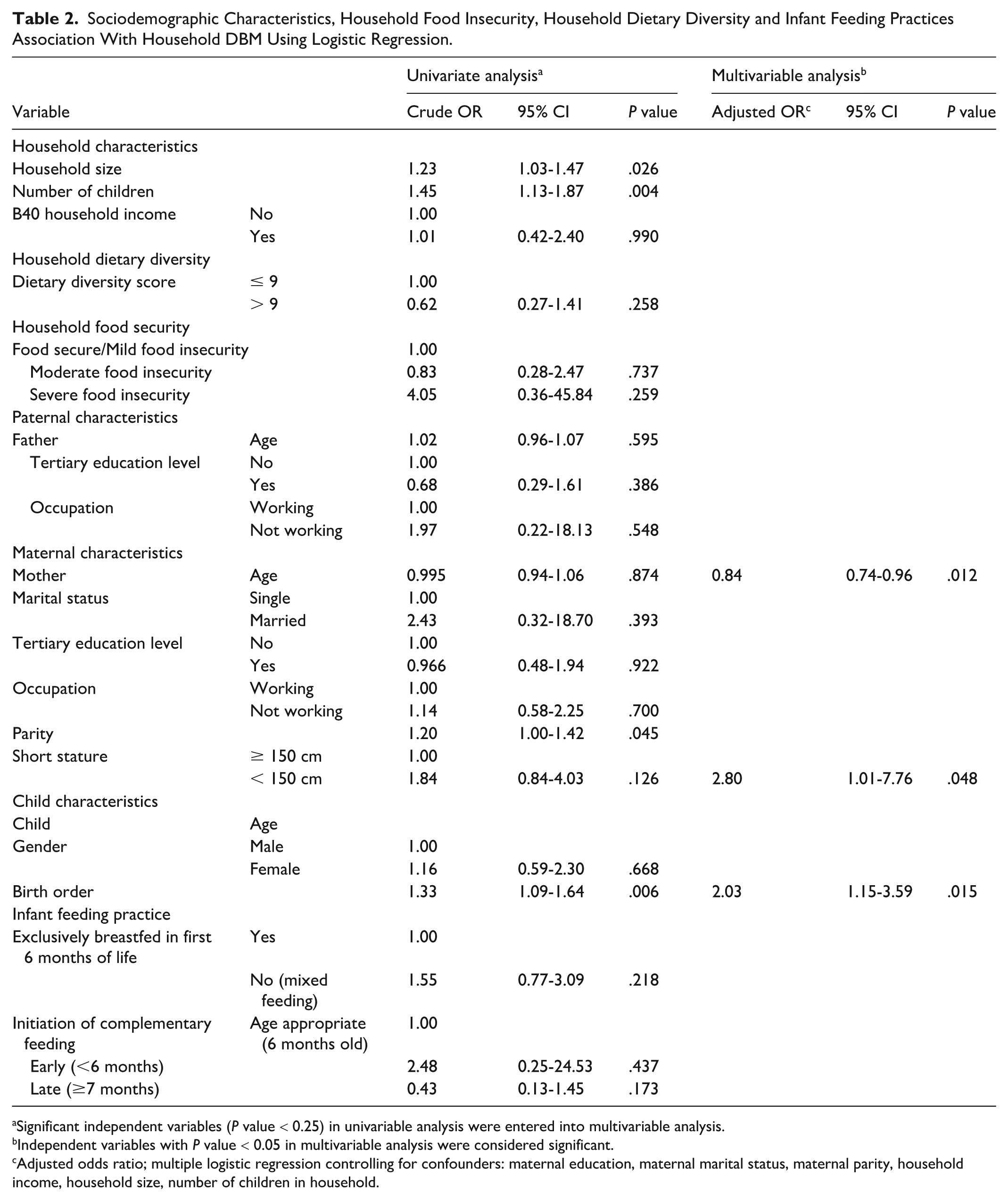
Significant independent variables (P value < 0.25) in univariable analysis were entered into multivariable analysis.
Independent variables with P value < 0.05 in multivariable analysis were considered significant.
Adjusted odds ratio; multiple logistic regression controlling for confounders: maternal education, maternal marital status, maternal parity, household income, household size, number of children in household.
No significant associations were found between levels of household food security and DBM, although severe food insecurity showed an elevated crude odds ratio (OR 4.05, 95% CI [0.36-45.84]). A dietary diversity score above nine appeared protective (OR 0.62, 95% CI [0.27-1.41]), though this was not statistically significant. Infant feeding indicators were also not significant. Mixed feeding during the first 6 months showed a higher but nonsignificant odds of household DBM (OR 1.55, 95% CI [0.77-3.09]). Similarly, early introduction of complementary foods increased the risk (OR 2.48, 95% CI [0.25-24.53]), although this result was not significant.
In multivariable analysis, older maternal age was protective, with the odds of DBM decreasing by 16% for each additional year (aOR 0.84, 95% CI [0.74-0.96]). This corresponds to a lower likelihood of DBM among older mothers. Maternal short stature (<150 cm) was associated with nearly threefold higher odds of household DBM (aOR 2.80, 95% CI [1.01-7.76]). This indicates that mothers with short stature had greater odds of DBM compared to those of normal height. Child birth order remained significant, with each increase in birth order doubling the odds of household DBM (aOR 2.03, 95% CI [1.15-3.59]). This suggests that children with more older siblings are associated with an increased likelihood of DBM. Other factors, including household size, food security status, dietary diversity, paternal education, maternal education, and infant feeding practices, did not show significant associations after adjustment. The final logistic regression model correctly classified 88.2% of cases. Specificity was high, with 99.3% of non-DBM households correctly identified (266 out of 268), while sensitivity was low at 8.1% (3 out of 37 DBM households). Despite this, ROC analysis indicated good discriminatory ability, with an AUC of 0.80 (95% CI [0.73-0.86], P < .001).
Discussion
This study focused on households represented by mother-child pairs from public early childhood education centres in Kuala Lumpur. These centres largely cater to low- and middle-income households located within or near government-subsidised housing. Although residency in subsidised housing or B40-income status were not strict inclusion criteria, the sample skewed towards families with constrained socio-economic resources who rely on public services.
Children in this study were aged 2 to 6 years old, with a median age of 5.2 years. Most nutrition research focuses on those under 5 years, following global monitoring frameworks such as WHO’s Global Nutrition Targets 2025 and UNICEF’s State of the World’s Children. Including older preschoolers fills a gap, as some may show catch-up growth or, conversely, cumulative deficits from prolonged inadequate intake. 19 This highlights a data gap often overlooked in national surveillance.
Despite high educational attainment, most mothers were not employed. This may be explained by caregiving responsibilities, limited childcare options, and cultural expectations that prioritise women’s domestic roles, consistent with national trends revealing many educated Malaysian women stay unemployed. 20 This contributes to household financial strain, increasing dependence on cheaper, calorie-dense foods, which may restrict dietary diversity and perpetuate intergenerational cycles of malnutrition. 21
Most households in this study were food secure or only mildly food insecure, with a lower prevalence of moderate or severe food insecurity compared to national SDG estimates. 22 This may reflect the study population’s characteristics, including higher maternal education, urban residence with widespread access to water and waste services, and enrolment in public early education centres, which may indirectly buffer against food insecurity. 23 Nevertheless, these results emphasise ongoing susceptibility to nutritional compromise, potentially affecting growth and health. Greater attention is needed for disadvantaged urban families through food and nutrition-sensitive aid design and delivery.
The household DBM prevalence in this study was at the lower end of regional estimates but remains a concern in urban low-cost housing. It was also lower than in local rural and Indigenous populations, where greater food insecurity and limited services heighten risk,9,10 whereas urban households may access more services but remain vulnerable due to reliance on affordable, energy-dense food. 21 These findings indicate nutritional vulnerability in urban environments, reflecting uneven access to healthy diets and potential long-term metabolic disorders and economic stress on both families and health systems. 2
The predominance of the OWOB/U subtype highlights child underweight as the major contributor to household DBM in these communities. Underweight reflects both acute and chronic nutritional stress and is linked to impaired immunity and higher morbidity. 24 Stunting, while less frequent in this study, remains the most common form of child undernutrition nationally and carries long-term cognitive and economic consequences. 25 The lowest prevalence was observed for OWOB/W and OWOB/T. Wasting is often linked to recent illness or acute food deprivation, while thinness captures undernutrition among children 5 years and older. 17 Their relatively low prevalence in this study may reflect fewer acute episodes, though underlying vulnerabilities remain.
In crude analysis, larger households, more children, and higher maternal parity were associated with DBM, reflecting the resource-dilution hypothesis where food and care are spread thinly. 26 Mothers in such households may also gain excess weight as they resort to low-cost, high-calorie foods. 2 After adjustment, only child birth order remained significant, suggesting risk is driven by later-born children. This highlights how constrained household resources within larger families may influence nutrient allocation and child growth, particularly among younger siblings.
Maternal age showed an inverse association, with older mothers at lesser risk of DBM. Available studies vary, as the association appears context-dependent. In some settings, older age reflects cumulative biological and social disadvantages, 27 while among others, younger mothers may be more vulnerable due to early motherhood under constrained conditions and limited decision-making power. 28 In this study, within the context of urban low-cost housing, older mothers may have accumulated knowledge, caregiving experience, and more predictable routines, which could enable more consistent meal preparation despite financial constraints. This is supported by studies showing higher maternal age associated with healthier child feeding behaviours, including lower consumption of soft drinks and snacks, 29 suggesting a need for targeted dietary and social support for younger mothers within urban communities.
Maternal short stature showed nearly threefold higher odds of DBM after adjustment. Though the confidence interval was wide due to small numbers, the direction of effect was consistent with regional findings that identify maternal height as a marker of intergenerational undernutrition.10,27 Maternal short stature reflects the cumulative effects of early-life nutritional deprivation that influence pregnancy outcomes and child growth, 25 and these results demonstrate such effects remain even in urban settings.
Severe food insecurity showed higher odds of DBM but was not significant, likely reflecting the small number of affected households. Evidence across Malaysia 9 and internationally 4 has been mixed, partly due to different measurement instruments and populations. Higher dietary diversity appeared protective yet was not significant and may be underestimated as diversity metrics capture food groups rather than nutrient quality or portion size. Exclusive breastfeeding and timely complementary feeding were common, reducing variability, but the direction of effect is consistent with evidence that breastfeeding and timely complementary feeding lower DBM risk. 27 Overall, food security, dietary diversity, and infant feeding practices may influence DBM indirectly through maternal and child factors, including early childhood behaviours that have been associated with variations in growth and anthropometric outcomes. 30
Strengths and Limitations
This study adds to the limited Malaysian literature on household DBM in urban low-cost housing, offering policy and programme-relevant insights. However, some limitations should be acknowledged. The cross-sectional design prevents inference of causality. Dietary information and household conditions were self-reported, introducing the possibility of recall and social desirability bias. Generalisability was limited to public preschool-attending households, and unmeasured factors such as physical activity were not captured. Nevertheless, the study’s use of validated tools and anthropometric measurements strengthens its contributions to public health knowledge.
Conclusion/Recommendation
This study identified a household DBM prevalence of 11% in Kuala Lumpur’s low-cost housing communities, with child underweight as the main subtype. Maternal age, maternal short stature, and higher child birth order emerged as associated factors, reflecting intergenerational vulnerabilities and resource dilution. Policy efforts can strengthen maternal nutrition, support young mothers, and expand access to affordable, healthy food and childcare in urban vulnerable groups. Future studies may adopt longitudinal designs, include broader urban populations, and examine physical activity and intrahousehold food allocation to clarify pathways and inform targeted interventions.
Footnotes
Acknowledgements
The authors would like to express their sincere gratitude to the Kuala Lumpur Department of National Unity and Integration for approving the conduct of this study at their Unity Kindergarten and Unity Childcare centres. They also extend heartfelt thanks to the dedicated teachers at these centres for their kind cooperation and support, particularly in facilitating communication between the research team and participating parents. The authors further acknowledge the Director General of Health, Malaysia, for granting permission to publish this article. It is hoped that the outcomes of this study will help guide future public health initiatives addressing the double burden of malnutrition within households in Malaysia’s urban low-cost housing communities.
Ethical Considerations
Ethical approval was obtained from the University of Malaya Research Ethics Committee on July 31, 2023 (Ref: UM.TNC2/UMREC_2812). Data were entered into REDCap using unique identifiers to preserve participant anonymity and confidentiality. The involvement of children in this study was limited to noninvasive procedures, specifically the measurement of height and weight. In accordance with national and institutional ethical standards, assent was not required as all participating children were below the applicable age threshold and the procedures posed minimal risk. Mothers or children identified with malnutrition were referred to nearby clinics and, with consent, food-insecure households were linked to relevant civil society organisations. The study adhered to the Declaration of Helsinki and Malaysian Good Clinical Practice Guidelines.
Consent to Participate
Consent forms, participant information sheets, and questionnaires were distributed through head teachers and reviewed by researchers during data collection. Written informed consent was obtained from all participating mothers prior to enrolment in the study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Universiti Malaya through the Universiti Malaya Impact-Oriented Interdisciplinary Research Grant Programme (IIRG) (Subprogramme Number: IIRG001B-2022IISS). The funding body had no involvement in the study design, data collection, data analysis, interpretation of findings, or manuscript preparation.
Data Availability Statement
The datasets generated and analysed during the current study are not publicly available due to confidentiality agreements with participants but are available from the corresponding author on reasonable request.