
Abstract
Climate change is a major factor influencing cardiovascular health, yet its impact on diverse cardiac conditions in East Asia remains insufficiently explored. This study investigated associations between meteorological factors and cardiac morbidity in 3 South Korean cities—Seoul, Busan, and Daejeon—using monthly administrative data from 2010 to 2023. Generalized additive models were employed to assess the effects of temperature, precipitation, and extreme weather indicators on acute pericarditis and heartbeat abnormalities. The results revealed distinct city-specific sensitivities: in Seoul, heatwave days were positively associated with increased pericarditis visits, while in Busan, more frequent precipitation days were linked to higher risks of heartbeat abnormalities. Furthermore, relative humidity emerged as a significant factor, with lower humidity levels correlating with increased pericarditis in Seoul and Daejeon, and higher humidity associated with elevated heartbeat abnormality risks in Seoul. Our results indicate that urban cardiovascular vulnerability involves a complex interplay of thermal and hygrometric stressors that varies by city. These findings highlight the importance of weather factors beyond temperature alone, suggesting the necessity of considering city-specific climate patterns in epidemiological monitoring.
Keywords
What We Already Know
Climate change, including rising temperatures and extreme weather events, contributes to increased cardiovascular morbidity and mortality.
Heatwaves and thermal stress are well-established triggers of cardiovascular events, especially in urban settings affected by the heat island effect.
Evidence from East Asia remains limited, particularly regarding how multiple meteorological factors—such as temperature, precipitation, and tropical nights—affect specific cardiac conditions.
What This Article Adds
Extends climate-cardiac research to acute pericarditis and heartbeat abnormalities—conditions with substantial healthcare burdens that are often underrepresented in climate epidemiology relative to fatal outcomes such as myocardial infarction.
Identifies city-specific meteorological associations: heatwave days with pericarditis in Seoul and precipitation frequency with heartbeat abnormalities in Busan, highlighting heterogeneous climate-cardiac pathways across urban environments.
Identifies relative humidity as an independent predictor of cardiac morbidity—with dry conditions linked to pericarditis in Seoul and Daejeon, and high humidity to heartbeat abnormalities in Seoul—proposing humidity as a candidate indicator for urban climate-health early warning systems.
Introduction
Climate change, characterized by rising temperatures and altered precipitation, increasingly contributes to adverse health outcomes. Among the conditions most sensitive to environmental stressors are cardiovascular diseases, which are particularly vulnerable to elevated temperatures and humidity that may exacerbate existing conditions and increase both morbidity and mortality. 1 Numerous epidemiological studies have established consistent associations between prolonged exposure to high temperatures and an elevated risk of myocardial infarction, arrhythmias, and other cardiovascular events. 2
In South Korea, recent decades have seen rising temperatures, increasing tropical nights, and more irregular rainfall. 3 These trends are pronounced in urban centers such as Seoul, Busan, and Daejeon, where the heat island effect amplifies thermal stress. Alongside these climatic shifts, ambient air quality remains a critical determinant of regional public health. While ambient air pollutants are known to exacerbate chronic conditions, 4 few studies have examined the combined effects of temperature, precipitation, and nighttime heat on cardiovascular health in East Asia. 5 Notably, recent Asia-Pacific investigation has identified humidity and temperature as critical predictors for climate-sensitive health outcomes. 6
While many studies have established links between meteorological factors and high-mortality cardiovascular conditions, research has often centered on outcomes that are direct causes of death, such as myocardial infarction. 2 In this study, we extended our focus to include outcomes that represent distinct physiological responses to environmental stress and contribute substantially to medical service utilization. Acute pericarditis, an inflammatory condition of the pericardial sac, has demonstrated seasonal variation consistent with viral respiratory activity, suggesting sensitivity to meteorological fluctuations, 7 and may be further aggravated by systemic or thermal stress. 8 Heartbeat abnormalities reflect autonomic nervous system sensitivity to ambient conditions; experimental evidence shows that high ambient temperature induces vagal withdrawal and impairs parasympathetic cardiac regulation, 9 and such irregularities are commonly observed during thermal stress.10,11 Both conditions remain underexplored in climate epidemiology despite representing a considerable healthcare burden. By investigating these specific outcomes across 3 major urban centers, we aimed to explore a wider spectrum of cardiovascular vulnerability and the resulting healthcare burden under changing climate conditions.
This study assesses associations between meteorological factors—temperature, precipitation, heatwaves, and tropical nights—and cardiac morbidity, focusing on acute pericarditis (I30) and heartbeat abnormalities (R00). We employed a time-series ecological design using 14 years (2010-2023) of monthly data from Seoul, Busan, and Daejeon to examine heterogeneous climate effects across urban environments. We hypothesized that higher temperatures, heatwaves, precipitation, and tropical nights would be associated with increased morbidity through regionally variable or nonlinear pathways. These findings aim to provide actionable insights for public health preparedness amid rapid urbanization and climate change.
Materials and Methods
This study employed a time-series ecological design to investigate the associations between meteorological variables—including temperature, rainfall, and extreme weather indicators—and cardiac-related morbidity across 3 major South Korean cities. A generalized additive model (GAM) with a quasi-Poisson distribution was used to account for overdispersion, to adjust for seasonality and long-term temporal trends, and to flexibly model potential nonlinear relationships between climatic factors and health outcomes. Long-term trends and seasonality were adjusted using penalized (k = 24) and cyclic cubic splines (k = 12), respectively, with smoothing parameters estimated via restricted maximum likelihood. To account for variations in population size over the 14-year study period, the logarithm of the annual city-level resident population was incorporated as an offset term in all models.
The study focused on 3 geographically distinct metropolitan areas in South Korea—Seoul (northwest), Daejeon (central), and Busan (southeast)—to reflect regional variation in climate and health outcomes. Monthly meteorological data, including average and maximum temperatures, rainfall, days with precipitation, heatwaves, and tropical nights, as well as environmental factors such as mean relative humidity (%) and particulate matter (PM10, μg/m3) were obtained from the Korea Meteorological Administration for the period between January 2010 and December 2023. In the analysis, meteorological factors including temperature, precipitation, heatwaves, and mean relative humidity were treated as primary exposure variables of interest. To address potential confounding by environmental factors, all models were adjusted for PM10 using a smooth term with 3-degrees-of-freedom (k = 3). A heatwave day was defined as a day with a maximum temperature of 33 °C or higher, and a tropical night was defined as a night with a minimum temperature that did not fall below 25 °C, in accordance with the criteria of the Korea Meteorological Administration. Health outcome data, including the number of patients and outpatient visit days related to acute pericarditis and abnormalities of heartbeat, were retrieved from the Health Insurance Review and Assessment Service for the same period. In this context, the number of patients was defined as the monthly count of unique individuals diagnosed with the condition, while visit days represented the total aggregate of days on which outpatient encounters occurred, regardless of whether they involved the same individual.
This study utilized monthly meteorological data and population-level health data from the selected cities, covering the entire resident population without applying specific eligibility criteria. The primary outcome included the monthly number of patients and healthcare visits related to acute pericarditis and abnormalities of heartbeat. Exposure variables included meteorological factors such as mean, maximum and minimum temperature, rainfall, precipitation days, mean relative humidity, heatwave days, and tropical nights, measured at the city level. These meteorological variables were modeled as smooth terms with 3- to 4-degrees-of-freedom (basis dimension k = 3-4), allowing for flexible but parsimonious nonlinear associations. Time trend and calendar month were modeled as smooth functions, as described above, to adjust for long-term and seasonal variations. For each exposure variable, a reference value of zero (e.g., zero heatwave days) or the minimum observed value (e.g., minimum monthly mean humidity) was used to calculate rate ratios (RRs) and their 95% confidence intervals. To visualize these associations, marginal RR curves were derived from the fitted GAM using the predict.gam() function. Predicted values were obtained on the log (link) scale by fixing all other covariates at their median values. The RR at each exposure level was calculated as the exponentiated difference between the predicted log count at that level and the predicted log count at the reference value. Pointwise 95% confidence intervals were calculated from standard errors (±1.96 × SE).
All meteorological variables were treated as continuous variables and entered as smooth terms. Lag effects were not modeled, as the study used monthly aggregated data. No subgroup or interaction analyses were performed. There were no missing data. While the primary analyses used mean temperature as the main exposure variable, additional models using maximum temperature were also explored to examine the robustness of the observed associations.
Results
This study used city-level aggregated data without individual participant characteristics. During the 14-year study period (2010-2023), the monthly mean number of patients with acute pericarditis across South Korea was 184, with regional means of 58 in Seoul, 12 in Busan, and 6 in Daejeon. The corresponding mean number of visit days were 154 in Seoul, 35 in Busan, and 17 in Daejeon. For abnormalities of heartbeat, the national monthly patient counts ranged from 10 300 to 51 000, with a mean of 22 000. The regional means were 6100 in Seoul, 1410 in Busan, and 670 in Daejeon. The respective mean number of visit days were 8300 in Seoul, 1890 in Busan, and 900 in Daejeon.
Figure 1 illustrates the monthly trends in nationwide average, minimum, and maximum temperatures from 2010 to 2023. The monthly maximum values of nationwide average, minimum, and maximum temperatures were primarily observed in the recent decade, particularly after 2018. Notably, July and August of 2018 recorded the highest monthly average and maximum temperatures, reaching 26.6 °C and 32.1 °C, respectively. Furthermore, September 2023 recorded the highest mean temperature for that month (22.6 °C) during the study period. Nationwide monthly temperature records revealed that many of the highest monthly temperatures were observed in recent years. Record-high temperatures concentrated after 2020, with March showing a warming trend.
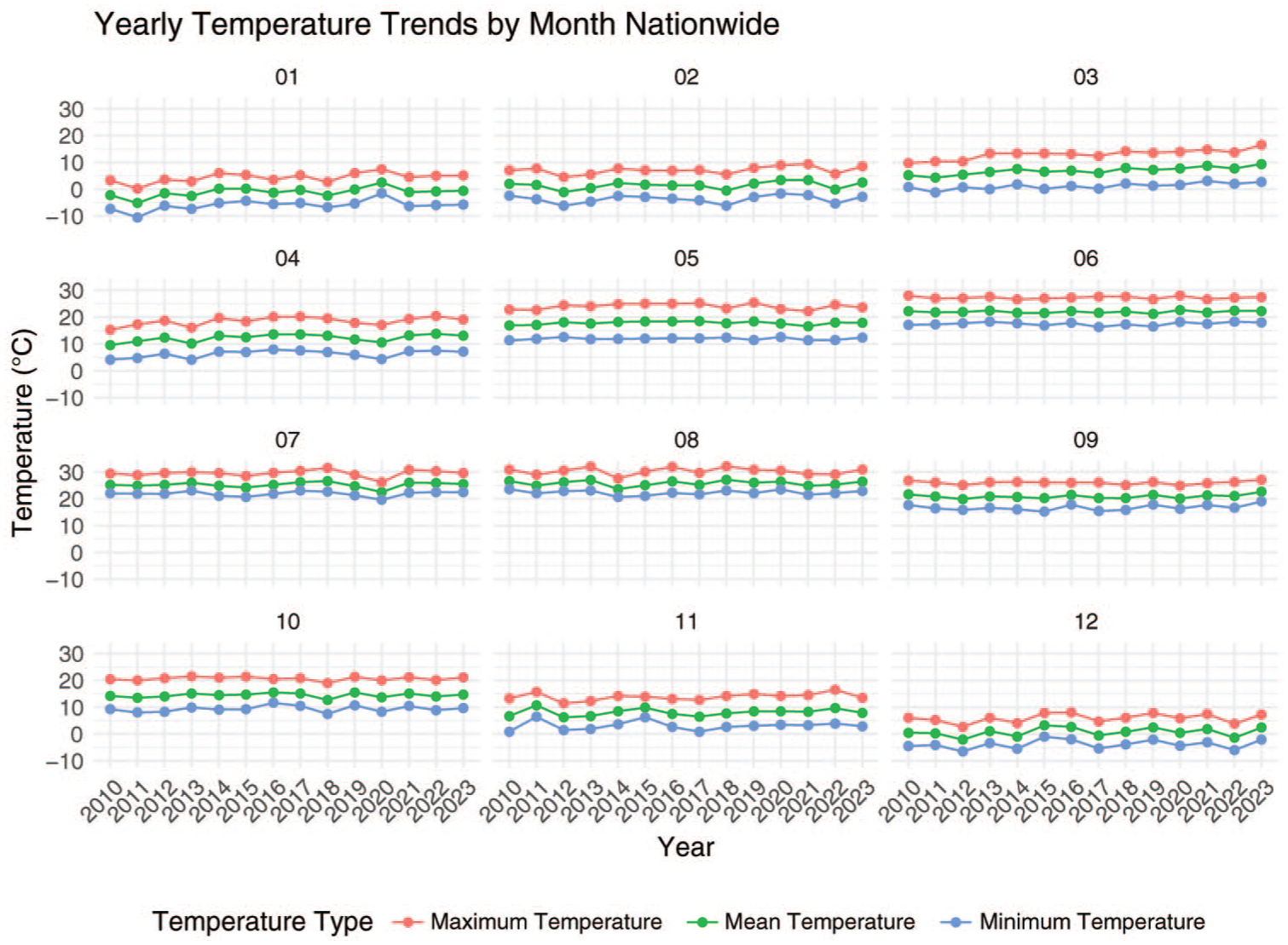
Yearly temperature trends by month in nationwide.
The smoothed effects of meteorological factors are summarized in Supplementary Tables 1 and 2. These tables present the effective degrees of freedom (edf) and P-values from the GAMs, indicating the overall contribution of each variable to the models. To further examine how cardiac risks vary across different weather conditions, marginal RR curves were visualized in Figures 2 and 3. As detailed in the Methods, these RRs illustrate the specific patterns of the exposure-response relationships while accounting for all covariates.
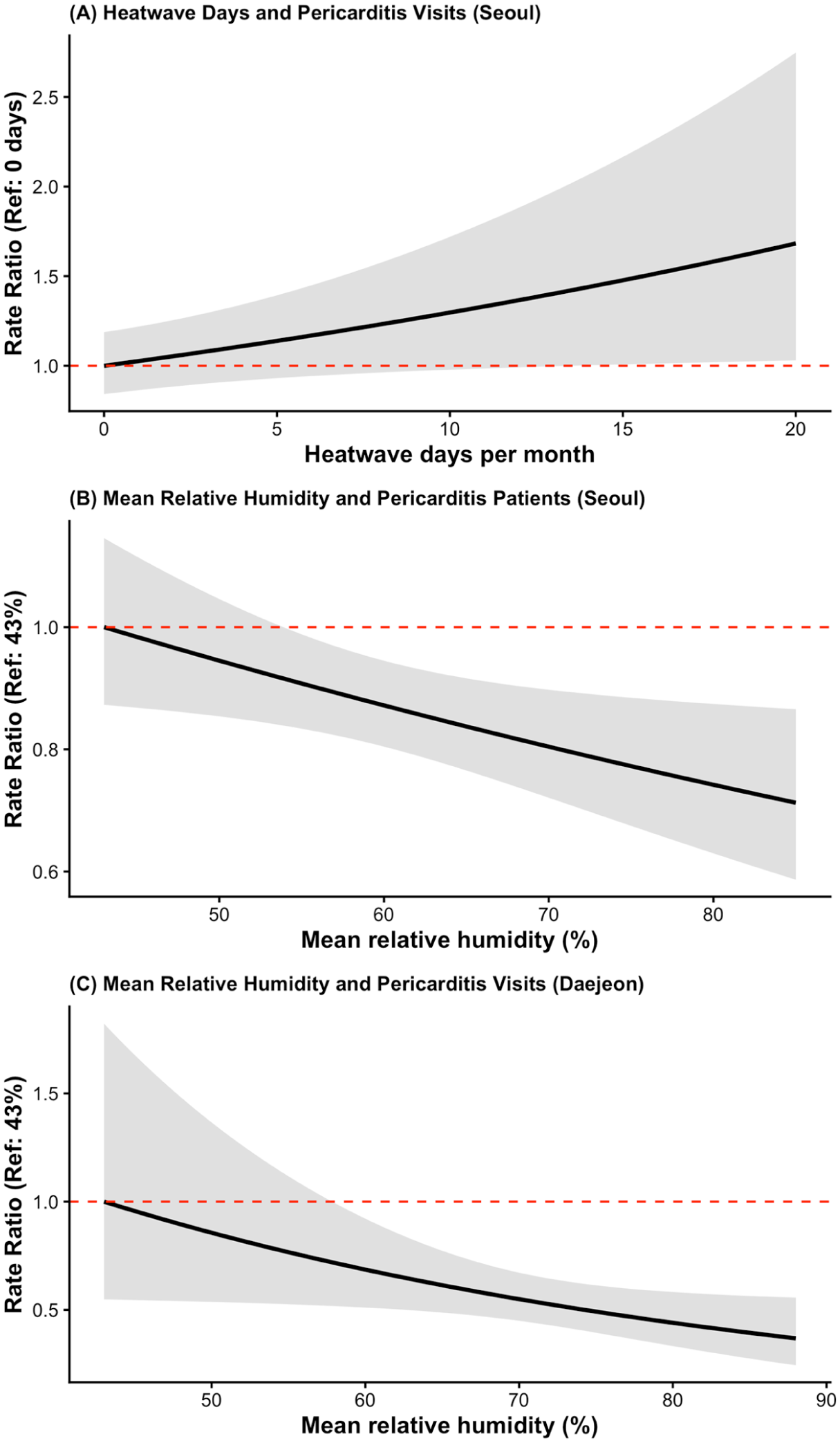
Associations between selected meteorological factors and acute pericarditis in Seoul and Daejeon. (A) Heatwave days and outpatient visits in Seoul; (B) Mean relative humidity and patient counts in Seoul; (C) Mean relative humidity and outpatient visits in Daejeon. Curves depict RRs relative to reference values (0 days for heatwaves; minimum observed monthly mean humidity for panels B and C), with shaded areas representing 95% confidence intervals. The models were adjusted for long-term trends and seasonality, PM10, and population offsets. All other covariates were fixed at their median values in the rate-ratio calculations.
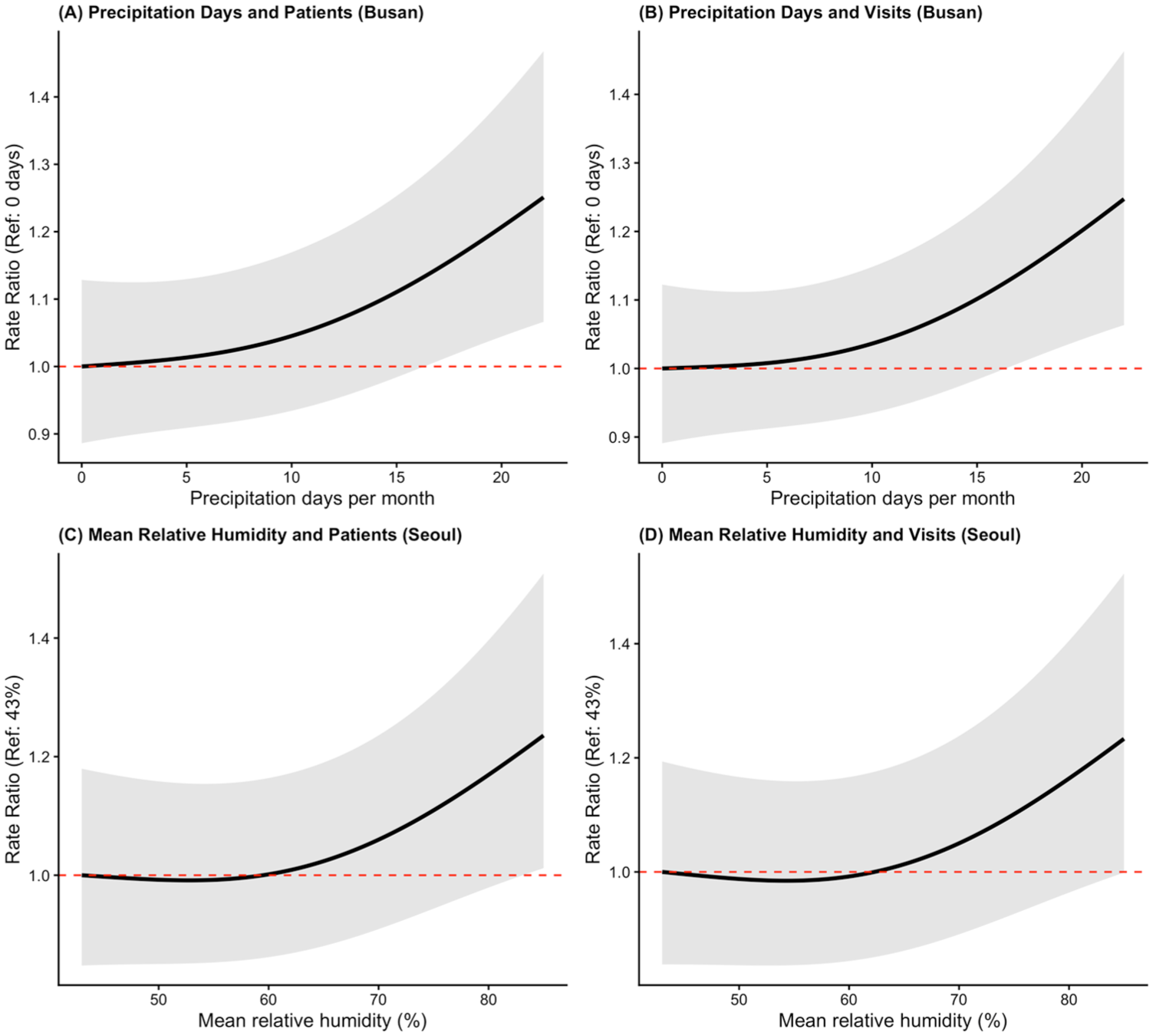
Associations between selected meteorological factors and abnormalities of heartbeat in Busan and Seoul. (A) Precipitation days and patient counts in Busan; (B) Precipitation days and outpatient visits in Busan; (C) Mean relative humidity and patient counts in Seoul; (D) Mean relative humidity and outpatient visits in Seoul. Curves depict RRs relative to reference values (0 days for precipitation; minimum observed monthly mean humidity for panels C and D), with shaded areas representing 95% confidence intervals. All models were adjusted for long-term trends and seasonality, PM10 and population offsets. All other covariates were fixed at their median values in the rate-ratio calculations.
For acute pericarditis, the number of heatwave days was significantly associated with outpatient visits in Seoul (P = .032) after adjusting for environmental confounders. Furthermore, mean relative humidity emerged as a significant independent correlate; low humidity levels were associated with increased patient counts in Seoul (P = .022) and higher outpatient visits in Daejeon (P = .036). In Busan, no meteorological variables reached statistical significance for acute pericarditis.
For abnormalities of heartbeat, precipitation-related indicators and humidity were more prominent. In Busan, the number of precipitation days was consistently associated with both patient counts (P = .014) and outpatient visits (P = .017). In addition, mean relative humidity showed a significant positive association with abnormalities of heartbeat in Seoul, particularly for patients counts (P = .024) and visits (P = .020). In Daejeon, no significant associations were identified for this outcome.
The smooth term for time was statistically significant in most models (typically P < .001), indicating the presence of strong long-term temporal trends. While many exposure variables had edf close to 1.0, suggesting linear associations, some factors such as precipitation days in Busan and humidity in Seoul exhibited higher edf values (>1.5), implying potential nonlinear effects. Overall, after adjusting for measured environmental confounders and population offsets, our findings indicate that specific meteorological factors, including heatwaves, precipitation frequency, and humidity, exert independent effects on cardiac-related morbidity, although these associations are highly city- and outcome-specific.
Figure 2 illustrates representative associations between meteorological factors and acute pericarditis, highlighting the independent impacts of heatwaves and humidity. In Seoul, the number of heatwave days showed a steadily increasing, approximately linear association with outpatient visit days (panel A). Furthermore, mean relative humidity emerged as a significant predictor for pericarditis. In Seoul, lower humidity levels were associated with increased patients counts (panel B), and a similar trend was observed for outpatient visits in Daejeon (panel C).
Figure 3 illustrates representative associations between meteorological factors and abnormalities of heartbeat. In Busan, the number of precipitation days emerged as a consistent and significant predictor; both patient counts (panel A) and outpatient visits (panel B) rose noticeably as the frequency of precipitation exceeded approximately 10 days per month. Furthermore, mean relative humidity showed a significant positive association with abnormalities of heartbeat in Seoul. Specifically, higher humidity levels were associated with increased patient counts (panel C) and outpatient visits (panel D), exhibiting a contrasting pattern to the humidity-pericarditis association observed in Figure 2.
To examine the robustness of the findings, additional models were fitted using maximum temperature instead of mean temperature as the primary exposure variable. The results were highly consistent across the 2 model specifications, with no meaningful differences in statistical significance, even when applying a more lenient threshold (P < .10). This consistency suggests that the observed associations are robust to the choice of temperature metric.
Discussion
Our findings extend existing research by focusing on cardiovascular morbidity rather than mortality, identifying how broad meteorological variables impact urban health. The pronounced urban heat island effect in Seoul likely exacerbates thermal stress and cardiovascular strain, especially among older adults.12 -15 This heightened vulnerability is believed to arise from a combination of factors, including impaired nocturnal cooling, increased metabolic demands, and compromised autonomic regulation.16 -18 The absence of heat relief in urban environments prolongs physiological stress, potentially exacerbating inflammatory responses in susceptible individuals. 19 Furthermore, the significance of relative humidity as an independent predictor suggests that the meteorological risk in Seoul is multifaceted. The observed negative association—where lower humidity levels correlate with higher pericarditis patient counts—points toward a potential biological mechanism where dry air impairs mucociliary clearance and compromises innate mucosal immunity. 20 This environment potentially increases susceptibility to respiratory viral infections, 21 which are well-recognized triggers that often precede the onset of acute pericardial inflammation.
In Busan, precipitation frequency emerged as a more consistent predictor for abnormalities of heartbeat than for acute pericarditis. Both patient counts and outpatient visits for heartbeat abnormalities increased significantly with a greater number of precipitation days, suggesting frequent rain plays a more pivotal role than total rainfall volume. Interestingly, our findings in Seoul further support this association, as higher relative humidity was also linked to increased healthcare utilization for heartbeat abnormalities. These parallel results across 2 major cities suggest a common underlying mechanism: high-humidity environments, often associated with frequent precipitation, can impair the evaporative cooling capacity of the human body. This failure in thermoregulation exacerbates thermal stress and triggers autonomic nervous system imbalances, which are known to provoke arrhythmic events and heartbeat irregularities. 22 While heavy, isolated rainfall events might occasionally provide temporary relief from extreme heat, the prolonged exposure to high-humidity conditions during frequent precipitation days appears to impose a sustained physiological strain on the cardiovascular system. These findings highlight the importance of considering the hygrometric aspect of rainfall, as the frequency of exposure to moist, unstable air masses may be more potent driver of cardiac-related morbidity that total monthly precipitation amounts.
In Daejeon, consistent with the patterns observed in Seoul, mean relative humidity emerged as a significant independent factor associated with acute pericarditis. This negative association indicates that lower humidity levels are linked to increased healthcare utilization, suggesting that arid environmental conditions may be associated with a higher risk of pericardial inflammation. This consistency across geographically distinct metropolitan areas reinforces the hypothesis that dry air may compromise the mucosal immunity of the respiratory system, 20 potentially facilitating the viral or bacterial infections that often serve as precursors to acute pericarditis. 21 While previous studies have predominantly focused on the thermal dimensions of climate change, our findings emphasize that the hygrometric state of the atmosphere—specifically persistent dryness—represents a distinct and significant factor for pericardial diseases. Furthermore, the robust and independent association identified in both Seoul and Daejeon suggests that moisture-related atmospheric variables may play a more prominent role in the occurrence of pericarditis than other transient meteorological events. These results highlight the potential utility of incorporating humidity as a component in public health surveillance for cardiovascular morbidity.
Several methodological limitations warrant consideration. As an ecological time-series analysis, the study was unable to account for individual-level confounders, such as age, sex, and pre-existing health conditions. Although we adjusted for PM10 as a primary environmental confounder, potential confounding effects from other air pollutants, such as nitrogen dioxide (NO2) or ozone (O3), were not fully incorporated into the models. Although we adjusted for PM10 as a primary environmental confounder, other air pollutants—including nitrogen dioxide (NO2) and ground-level ozone (O3)—were not incorporated into the models. Both pollutants are known to interact with thermal stress and independently affect cardiovascular and respiratory outcomes, and their omission may introduce residual confounding, particularly during summer heatwave periods when photochemical oxidant concentrations are elevated. In addition, the use of health insurance claims data reflects healthcare utilization patterns rather than true disease incidence; factors such as healthcare accessibility, individual health-seeking behavior, and socioeconomic status may have differentially influenced visit rates across cities. Furthermore, while seasonal smooth terms were included to partially account for infectious disease seasonality—relevant especially for pericarditis—granular fluctuations in viral respiratory activity were not directly measured, and their residual influence on observed associations cannot be excluded. Furthermore, while our analysis focused on concurrent monthly associations, the use of monthly aggregated data restricts the temporal resolution, potentially obscuring short-term exposure-response relationships and immediate lag effects. These limitations might prevent the detection of acute physiological responses to daily meteorological fluctuations, which could offer additional insights into the temporal dynamics of cardiac risks. In particular, the absence of lagged exposure modeling means that delayed physiological responses—such as those occurring 1 to 3 days after a heatwave or sustained period of high humidity—cannot be captured in the current analytical framework. This is especially relevant for conditions like heartbeat abnormalities, where autonomic dysregulation may manifest with a short but meaningful temporal delay following meteorological stress. Future studies using daily-level data with distributed lag non-linear models would be better positioned to disentangle immediate versus delayed effects and provide more precise estimates of exposure-response relationships. Although standardized climate measurements were employed, these may not accurately reflect the actual perceived climate conditions or personal exposures experienced by individuals in their daily environments. As all analyses were conducted exclusively in major urban centers, the findings may not be generalizable to rural or non-urban populations. Socioeconomic factors, healthcare accessibility, and individual health-seeking behaviors likely influenced the observed results, particularly regarding the heterogeneous associations identified for humidity and precipitation-related variables. Furthermore, while temporal variables were included in the models to account for seasonality, these may only serve as proxies and might not fully capture granular fluctuations in seasonal infectious diseases or shifts in healthcare-seeking behaviors that could independently influence cardiac-related visits. In addition, the scope of this study was limited to 2 specific cardiovascular categories, which may not represent the full spectrum of climate-related cardiac risks. The absence of stratified analyses based on disease severity or individual-level clinical characteristics further restricts the generalizability and direct clinical application of these findings. Future research encompassing a broader range of cardiovascular outcomes and multi-level patient data is necessary to refine the clinical interpretation of meteorological impacts.
Future research should utilize individual-level longitudinal data to achieve finer control over confounding factors. Incorporating models with lagged exposure effects and aligning clinical records with high-resolution meteorological data would further improve the precision of these estimates.
Despite its limitations, this study provides possible insights into the complex relationship between climate variables and cardiovascular health. By demonstrating that humidity and precipitation frequency—alongside extreme heat—are significant factors associated with cardiac morbidity, these findings offer practical implications for the development of public health policies and early warning systems in rapidly warming urban environments.
From a public health perspective, our findings carry several actionable implications. First, city-specific meteorological thresholds—such as approximately ten precipitation days/month threshold identified in Busan or the elevated heatwave day burden in Seoul—could serve as empirically grounded triggers for cardiovascular health alerts within existing meteorological early warning systems. Second, given that humidity independently predicted both pericarditis and heartbeat abnormalities, incorporating hygrometric indices alongside temperature in heat-health watch systems would improve their sensitivity to a broader spectrum of cardiac risks. Third, urban planners and public health authorities should consider city-level climate heterogeneity when designing climate adaptation strategies, as a uniform national policy may fail to capture locally dominant stressors.
Conclusions
This study explores the complex and heterogeneous associations between meteorological factors and cardiac conditions across 3 major South Korean cities. Our findings suggest that extreme heat and humidity are important factors associated with cardiovascular morbidity, even after accounting for atmospheric pollutants and population shifts. In Seoul, the number of heatwave days was positively associated with outpatient visits for acute pericarditis. Furthermore, relative humidity emerged as a notable factor in these observations; lower humidity levels were linked to increased pericarditis in Seoul and Daejeon, whereas higher humidity and frequent precipitation were associated with greater heartbeat abnormality rates in Seoul and Busan, respectively. These findings emphasize that both thermal and hygrometric stressors uniquely contribute to cardiovascular health in different urban environments. Given the ecological design of this study, these findings should be interpreted as exploratory associations rather than causal interpretations. Future research utilizing individual-level data and incorporating lagged exposure effects will be essential to move toward causal inference and improve generalizability. By identifying specific meteorological correlates beyond temperature alone, these findings provide a foundation for further research and the development of targeted public health strategies to mitigate climate-related cardiovascular risks in urban populations.
Supplemental Material
sj-docx-1-aph-10.1177_10105395261452740 – Supplemental material for Associations Between Meteorological Factors and Cardiac-Related Morbidity in 3 South Korean Cities
Supplemental material, sj-docx-1-aph-10.1177_10105395261452740 for Associations Between Meteorological Factors and Cardiac-Related Morbidity in 3 South Korean Cities by Taeon Lee, Seyoung Choi, Dongryul Kim and Chunhoo Cheon in Asia Pacific Journal of Public Health
Footnotes
Ethical Considerations
This study was reviewed and approved by the Institutional Review Board of Kyung Hee University (registration number KHSIRB-25-511 (EA)), which granted exemption from ethical review for the use of pre-existing, aggregated, and publicly available data.
Author Contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Kyung Hee University Undergraduate Research Program; and National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT) (No. 2020R1A5A2019413). The funder had no role in design, management, analysis and publication of the study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data analyzed in this study are publicly available. Meteorological data were obtained from the Korea Meteorological Administration (https://data.kma.go.kr/), and health outcome data were retrieved from the Health Insurance Review and Assessment Service (![]() ). No additional datasets were generated by the authors.
). No additional datasets were generated by the authors.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.