
Abstract
Introduction
The COVID-19 pandemic has increased the prevalence of mental health issues. A national mental health survey conducted in March 2020, during the first wave of the pandemic in South Korea, reported that 48% of the population experienced feelings of depression related to COVID-19. Consequently, experts emphasized the need for interventions to prevent a “mental-demic,” a phenomenon in which psychological impacts or trauma spread across society like an infectious disease. 1
Infectious diseases are often accompanied with stigma, and the stigma associated with COVID-19 can be a contributing factor to depression. 2 However, the relationship between the societal stigma surrounding COVID-19 and depression in the general population remains insufficiently examined.
Hence, this study aimed to fill this research gap by analyzing the relationship between the societal stigma surrounding COVID-19 and depression in the general population.
Methods
This study used raw data from the Korean National Mental Health Survey due to COVID-19 (KNMHS-Cov19). The KNMHS-Cov19 data measured the mental health status of Korean adults aged 19 years and older during the COVID-19 pandemic, covering 17 provinces nationwide in Korea. The survey was conducted online in March 2021, 1 year after the COVID-19 outbreak in South Korea, and the sample size was 2000. 3
Participants represented the general adult population regardless of COVID-19 infection history; therefore, the sample included both individuals who had experienced COVID-19 infection (personally or among close contacts) and those without such experience.
The severity of self-reported depression was assessed using the Patient Health Questionnaire 9-item (PHQ-9) scale of the PRIME-MD instrument. The answers are calculated to achieve a total score within 0 to 27. The cutoff value for PHQ-9 to define depressive symptoms was set at 10 points. 4 Stigma, the key variable of interest, was measured through the question, “Do you perceive social stigma toward individuals confirmed with COVID-19?” The responses were categorized into three: “No,” “Yes,” and “Strongly Yes.”
This study included several potential confounding factors: demographic factors (eg, sex and age); socioeconomic factors (eg, marital status, educational level, and annual household income); COVID-19-related factors (eg, changes in economic status during the pandemic and subjective stress caused by COVID-19, both measured on a 5-point Likert scale); mental health factors (eg, sleep quality during the pandemic, measured on a 5-point Likert scale); and health-related factors (eg, underlying conditions). These factors were incorporated into the final model.
To analyze the study’s final objective, which was to assess the impact of the “perceived stigma” on depression, we employed logistic regression analysis. Statistical data were analyzed using STATA version 14, and the level of significance (α) was .05.
Results
Among 2000 participants, 353 (17.7%) had depressive symptoms. Depressive symptoms also varied according to COVID-19 infection experience, with higher prevalence among respondents who reported infection in themselves or their close contacts compared with those without such experience. The prevalence of depressive symptoms was significantly higher among participants perceiving social stigma related to COVID-19 compared to those who did not. Specifically, the depression prevalence was 8.9%, 17.5%, and 39.1% in those who reported “No,” “Yes,” and “Strongly Yes” regarding stigma perception, respectively (Table 1).
Prevalence of Depression According to the General Characteristics of the Study Sample.
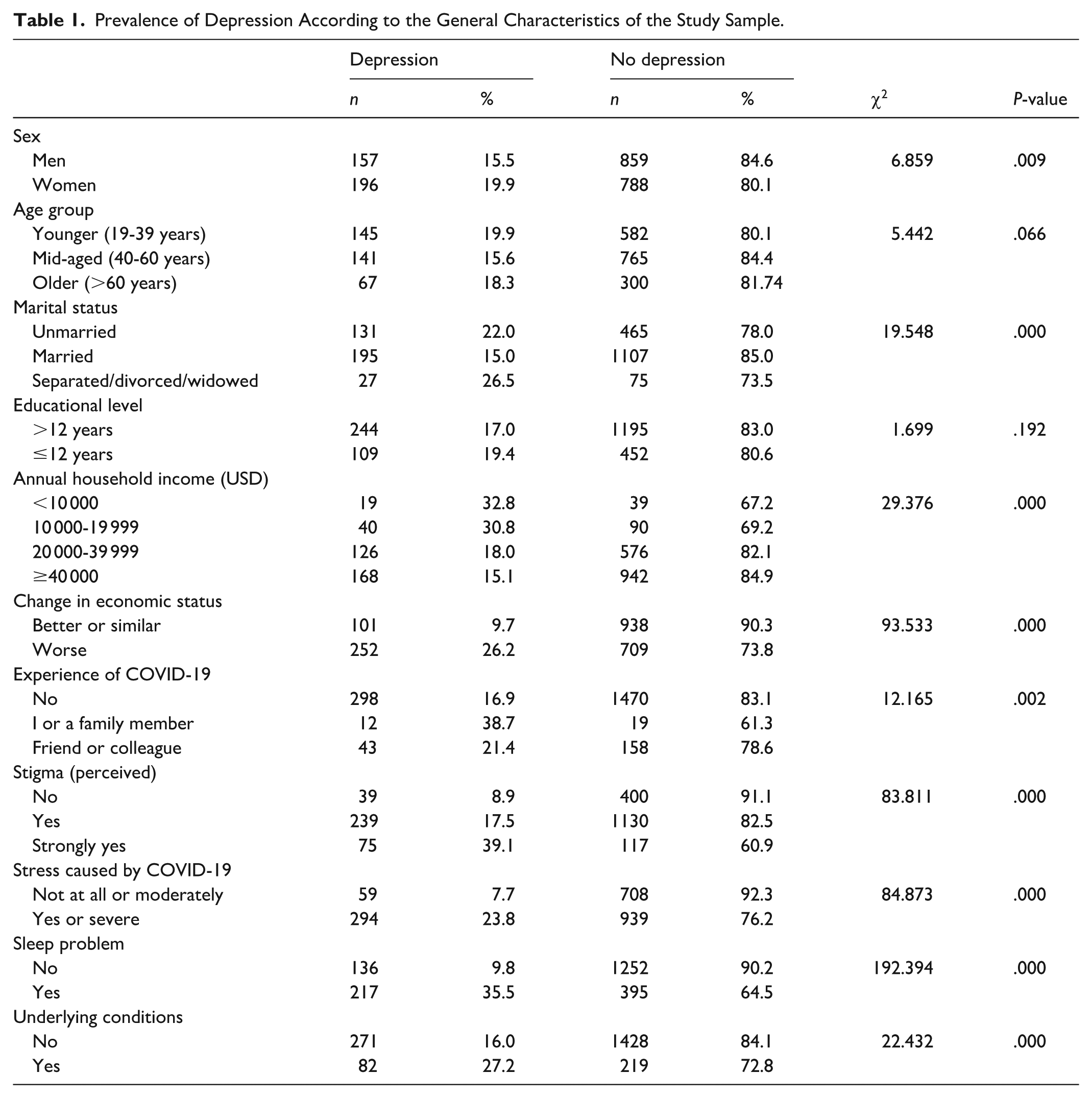
Table 2 presents the factors associated with depression. Compared with those participants without stigma perception, those with stigma perception had a 1.75 times higher risk of depression (95% confidence interval [CI]: 1.18-2.60), and those with “Strongly Yes” responses had a 4.42 times higher risk of depression (95% CI: 2.71-7.20).
Logistic Regression Results of the Association Between Perceived Stigma and Depression.
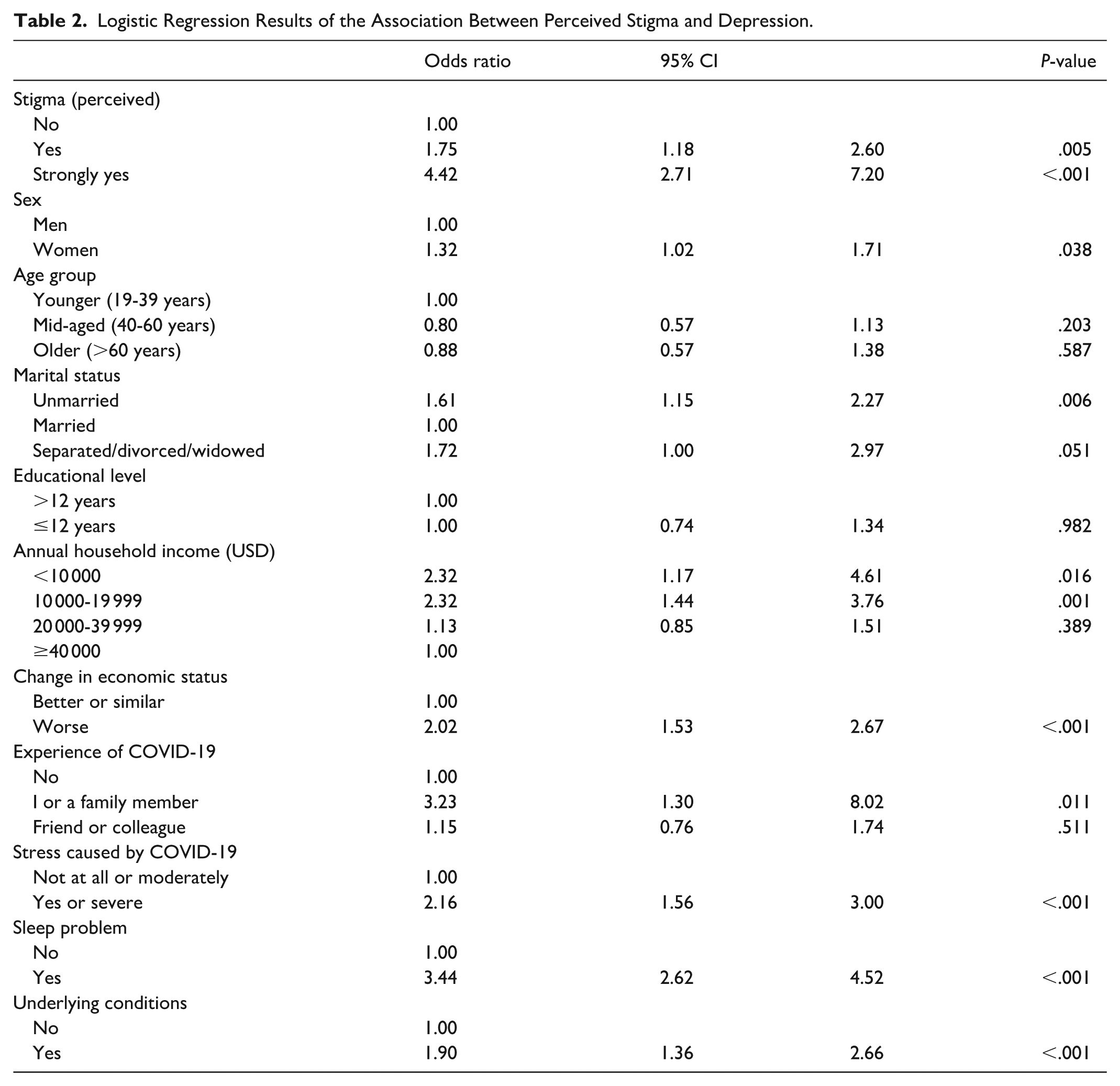
In the domain of socioeconomic factors, marital status was a significant risk factor for depression. Among the COVID-19-related factors, changes in economic status during the pandemic and subjective stress caused by COVID-19 were significant. In terms of mental and physical health-related factors, sleep quality during the pandemic and the presence of underlying conditions were significant.
Discussion
This study investigated the association between perceived stigma toward individuals diagnosed with COVID-19 and depressive symptoms in the general population. Results revealed that stigma perception is significantly related to depressive symptoms during the pandemic, with individuals reporting higher levels of stigma perception exhibiting a greater likelihood of depressive symptoms. These findings align with previous studies highlighting stigma as a critical stressor contributing to mental health issues during infectious disease outbreaks.5,6 Unlike previous studies wherein the study population was limited to specific subgroups such as health care workers or COVID-19 survivors, this study examined the relationship between stigma and depression in the general population. While prior studies have documented the high prevalence of stigma and depression among health care workers,7,8 this study demonstrates that stigma is a significant risk factor for depression even in the broader population.
These results contribute to the growing body of evidence on the psychological impact of stigma during infectious disease outbreaks and provide valuable insights for public health strategies aimed at mitigating mental health consequences. First, considering the strong association between stigma perception and depressive symptoms, public health campaigns are needed to address stigma during infectious disease outbreaks. Moreover, educational initiatives should aim to reduce stigma. Second, pandemic response plans should include mental health support to identify and assist individuals at risk of depression, particularly those experiencing high levels of stigma perception.
Despite its contributions, this study has several limitations. First, the cross-sectional design limits the ability to establish causal relationships between stigma perception and depression. Hence, longitudinal studies are needed to determine whether stigma precedes depression or if individuals with depression are more likely to perceive stigma. Second, reliance on self-reported data may introduce bias because participants may underreport or overreport their experiences of stigma and depression. Third, the study’s findings are based on data from South Korea; thus, they may not be generalizable to other cultural or socioeconomic contexts.
Conclusion
Perceived stigma plays a critical role in shaping mental health outcomes during infectious disease outbreaks. Stigma perception is strongly associated with depressive symptoms in the general population; thus, comprehensive public health strategies that address both the medical and social dimensions of infectious diseases are necessary. Reducing stigma should be central to pandemic preparedness, ensuring that individuals are not only physically but also psychologically protected during public health crises.
Footnotes
Authors’ Note
AI was not used in the analysis or preparation of this manuscript.
Ethical Considerations
The present study was approved (Number P01-202402-01-005) by the Public Institutional Review Board Designated by Ministry of Health and Welfare.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was supported by Soonchunhyang University Research Fund.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.