
Abstract
This study explored how different multimorbidity patterns impact transitions between cognitive stages in the elderly in China using data from the Chinese Longitudinal Healthy Longevity Survey (CLHLS). The data included 8778 dementia-free participants aged ≥60 years (21 500 observations). At baseline, K-Means clustering identified 3 multimorbidity patterns: cardiovascular, sensory, and multisystem. A multistate Markov model estimated transition probabilities. Results showed that compared with the sensory pattern, the cardiovascular pattern (hazard ratio [HR] 0.45, 95% CI [0.34, 0.60]) and the multisystem pattern (HR 0.48, 95% CI [0.37, 0.63]) were associated with a lower risk of progression from normal cognition to cognitive impairment. The sojourn time for normal cognition in the sensory pattern is shorter than that in cardiovascular and multisystem patterns. At age 80, the sojourn time for cognitive impairment in the sensory pattern is longer (1.96 years) than that in others (1.42 and 1.55 years) but converged with other patterns at ages 90 and 100. Different multimorbidity patterns exhibit distinct transitions between cognitive stages. Targeted interventions based on risk factors may mitigate cognitive decline in the elderly.
Keywords
What We Already Know
Elderly individuals with multimorbidity are at high risk of developing cognitive impairment.
Specific multimorbidity patterns have distinct effects on cognition.
Cognitive state transitions constitute a dynamic and continuous neurobiological process.
What This Article Adds
This study employs a Markov modeling approach from a dynamic perspective to examine how distinct multimorbidity patterns influence transitions across cognitive states among the elderly.
The sensory pattern is associated with a higher risk of progression from normal cognition to cognitive impairment compared to the cardiovascular and multisystem patterns.
Introduction
The world is currently experiencing an unprecedented wave of aging. In 2020, the population of Chinese individuals aged 65 years and above reached 191 million, accounting for 13.5% of the total population. 1 With population aging intensifying, chronic diseases have become increasingly common among the elderly. The simultaneous presence of 2 or more diseases is defined as multimorbidity, and 75% of elderly individuals in China aged 65 years and above suffer from it. 2 This challenge is not unique to China; across the Asia-Pacific region, aging populations face a growing burden of multimorbidity. 3 Research has demonstrated that the presence of multiple chronic diseases, such as cardiovascular disease, diabetes, and respiratory illnesses, can significantly accelerate cognitive decline. 4 Research utilizing nationwide survey data has demonstrated that for every additional chronic disease, the cognitive function score may decrease (β = -0.064). 5 While this effect size appears modest, its cumulative impact over time in the elderly population is clinically meaningful.
Specific types of multimorbidity have differential impacts on cognition. Cardiometabolic multimorbidity is closely related to declines in executive function and memory, possibly impairing brain regions through cerebrovascular lesions and insulin resistance. 6 The effect of the respiratory/osteoporosis pattern on cognition may be lower than that of the hypertension/diabetes pattern. 7 Evidence indicates that sensory multimorbidity increases the risk of cognitive decline and dementia. 8 Furthermore, research from the Asia-Pacific region suggests that broader social and environmental factors, such as participation in community programs, are also associated with better overall functional health in older adults, which may encompass cognitive domains. 9
Cognitive state transitions constitute a dynamic and continuous neurobiological process, typically following the trajectory from normal cognition → cognitive impairment → dementia → death. Cognitive impairment plays a critical role in this process and is widely regarded as the transitional state between normal aging and dementia. Approximately 10% to 15% of individuals with cognitive impairment progress to dementia each year, which is much higher than the 1% to 2% annual conversion rate observed in healthy individuals. 10 This conversion risk makes cognitive impairment a key window for dementia prevention. Early intervention during the cognitive impairment stage is most effective, potentially delaying the onset of dementia. 11 Understanding the impact of disease patterns on cognitive state transitions is crucial for dementia prevention.
Previous studies have examined multimorbidity patterns among middle-aged and older adults in China and found that the cardiometabolic pattern is the predominant cluster.12,13 Another study with participants with a higher mean participant age (75.10 years) reported that the sensory pattern was nearly as prevalent as the cardiometabolic pattern. 14 However, relatively few researches have focused specifically on the elderly in China or explored how their disease patterns relate to cognition. Using nationally representative data from CHARLS, 1 study identified multimorbidity patterns through latent class analysis and demonstrated significant associations between specific patterns and memory-related diseases among middle-aged and older Chinese adults. 15 Another longitudinal study further revealed that the interaction between multimorbidity and lifestyle factors substantially influences cognitive impairment risk in older Chinese adults. 16 Chen et al 17 investigated multimorbidity patterns among the oldest-old populations in China and compared the associations of different disease clusters with cognitive function, finding that neurological disorders comorbid with other conditions were the principal determinants of cognitive performance in this age group. Other researchers have used generalized estimating equations as well as linear and logistic regression models to examine links between multimorbidity and cognitive function, but these approaches cannot capture transitions among cognitive states. 18
Few studies have explored how different multimorbidity patterns affect this process from a dynamic perspective. Traditional statistical methods struggle to capture the dynamic transitions among cognitive states, whereas multistate Markov models can effectively simulate transitions between different cognitive states and death, offering a novel angle of research. Using data from the Chinese Longitudinal Healthy Longevity Survey (CLHLS), a longevity-focused cohort of Chinese older adults, this study aims to uncover the impact of multimorbidity patterns on cognitive state transitions among the elderly in China and to provide information on the sojourn time in each cognitive state for individuals with different multimorbidity patterns.
Methods
Study Population
Study population data were sourced from the publicly available CLHLS, a prospective cohort study targeting Chinese individuals aged 60 years or older. This study used data from the waves conducted between 2002 and 2018. The CLHLS applied a multistage, stratified cluster sampling design to recruit participants from half of the counties in 23 provinces in China. The CLHLS study was approved by the Ethics Committee of Peking University (IRB00001052–13074). Detailed information on the CLHLS study design can be found elsewhere. 19
In this study, 8778 participants were recruited from 2002 to 2018 (across 4 waves), with each participant undergoing 1 baseline survey and 2 follow-up surveys, resulting in a total of 21 500 observations. The exclusion criteria were as follows: (1) individuals without multimorbidity; (2) participants missing Mini-Mental State Examination (MMSE) scores at all follow-up waves; and (3) those diagnosed with dementia at baseline. The detailed inclusion and exclusion criteria are shown in Supplemental Figure 1.
Measurements
Chronic Conditions and Multimorbidity
At baseline, data on 14 individual conditions or chronic diseases were collected to assess multimorbidity. The following 12 conditions were self-reported by participants: diabetes, heart disease (including coronary artery disease, arrhythmia, heart failure, valvular disease, and other heart diseases), hypertension, stroke or cerebrovascular disease, respiratory diseases (bronchitis, emphysema, asthma, and pneumonia), tuberculosis, cancer, prostate tumor, stomach or duodenal ulcer, Parkinson’s disease, pressure ulcers, and arthritis. Responses for each condition were coded as binary data. Visual impairment was defined as participants being blind or reporting that they had glaucoma or cataracts to such an extent that they could not see or distinguish breaks within a circle. 2 Hearing loss was defined as participants requiring a hearing aid. The presence of 2 or more conditions was defined as multimorbidity.
Cognitive Assessment
The Chinese version of the MMSE was used to measure cognitive function. It was adapted from the original MMSE developed by Folstein et al in 1975 to suit the Chinese elderly population, 20 and its validity and reliability have been verified. 21 The MMSE comprises 6 dimensions—orientation, registration, naming, attention and calculation, recall, and language—across a total of 24 items. 22 The total score ranges from 0 to 30, with higher scores indicating better cognitive function. An MMSE score below 24 was defined as cognitive impairment. 20 Dementia was assessed based on self- or proxy-reported doctor diagnoses.
Mortality
During follow-up surveys, the mortality status of the participants was collected through interviews with their closest relatives.
Covariates
The covariates in this study included age, sex, education, marital status, living arrangement, and exercise behavior. Age was treated as a time-varying covariate. Educational level was categorized into 3 groups: illiterate, primary school, and middle school or above. Marital status was classified as married (including those cohabiting and living with their spouse) or single (separated, divorced, widowed, or never married). Living arrangement was divided into living with family, living alone, or living in an institution. Exercise behavior was classified based on participants’ self-reported regular exercise behavior (yes or no).
Statistical Analysis
In this study, K-Means clustering analysis was performed on the baseline data of 8778 participants with multimorbidity to identify multimorbidity patterns. The analysis included 14 chronic conditions, with each condition treated as a binary variable (present/absent). First, multiple correspondence analysis (MCA) was applied to summarize the information contained in the various categorical variables into a low-dimensional space. This method allows the relationships among a set of binary or categorical variables to be represented in a multidimensional space, thus enabling the examination of potential associations among the 14 individual chronic conditions.
Next, the K-Means algorithm was used to define the clusters, resulting in the final multimorbidity patterns. The optimal number of clusters (k = 3) was determined by evaluating the average silhouette width and the Calinski-Harabasz (CH) index across a range of solutions (k = 2-5). k = 3 was selected as it provided the most clinically meaningful patterns. In this approach, patients were assigned to the group whose center was closest. The average values of the observations assigned to each group were calculated, and the process was iterated until no further reassignments occurred between clusters. To assess internal cluster quality, the stability of the optimal solution was analyzed using Jaccard bootstrap coefficients (100 runs). The mean Jaccard similarities for the three identified clusters were 0.54, 0.51, and 0.68, respectively, indicating that the clusters captured robust, reproducible patterns within the complex dataset.
Using the R package msm, 23 a multistate Markov model was constructed to evaluate transitions across different cognitive states and death. The multistate Markov model is used to describe the movements of individuals among different states over continuous time. We defined 3 cognitive states, and the model comprised 4 states (normal cognition as state 1, cognitive impairment as state 2, dementia as state 3, and death as state 4), with death designated as the absorbing state. Individuals may transition between different cognitive states, but dementia cannot revert to cognitive impairment or normal cognition. Individuals may die from any state; however, once the absorbing state is reached, no further transitions occur. Specific transition pathways are shown in Supplemental Figure 2. At time t, the individual is in state S(t). The transition intensity represents the instantaneous risk of moving from state r to state s at time t and is defined as:

All intensities form a matrix
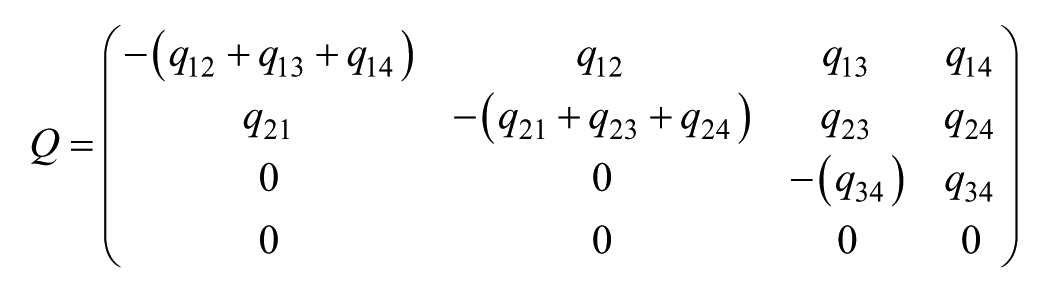
Under the Markov assumption, the transition intensities are estimated by maximizing the likelihood function using the quasi-Newton iterative method. Based on the model, HRs and 95% confidence intervals for cognitive state transitions under different disease patterns were reported. The model was adjusted for several covariates, including age, sex, education, marital status, living arrangement, and exercise behavior.
The R package elect 24 was used to estimate sojourn times. Based on the parameters from the multistate Markov model, sojourn times were calculated for individuals with each multimorbidity pattern for the transitions from normal cognition to cognitive impairment, from cognitive impairment to dementia, and from dementia to death. Sojourn times were also calculated separately for men and women of different ages, assuming average levels of education (illiterate), marital status (single), living arrangement (living with household member), and no exercise behavior.
All statistical analyses were performed using R (version 4.4.0).
Results
K-Means Clustering
A total of 8778 elderly individuals with multimorbidity were included in the study at baseline. K-Means clustering analysis identified 3 clusters (Figure 1). The top 5 most prevalent conditions within each cluster are presented in Supplemental Table 1. Based on these condition profiles, 3 multimorbidity patterns were determined: cardiovascular pattern (25%), sensory pattern (40%), and multisystem pattern (35%). Among these, the sensory pattern was the most prevalent one, whereas the cardiovascular pattern was the least common one.
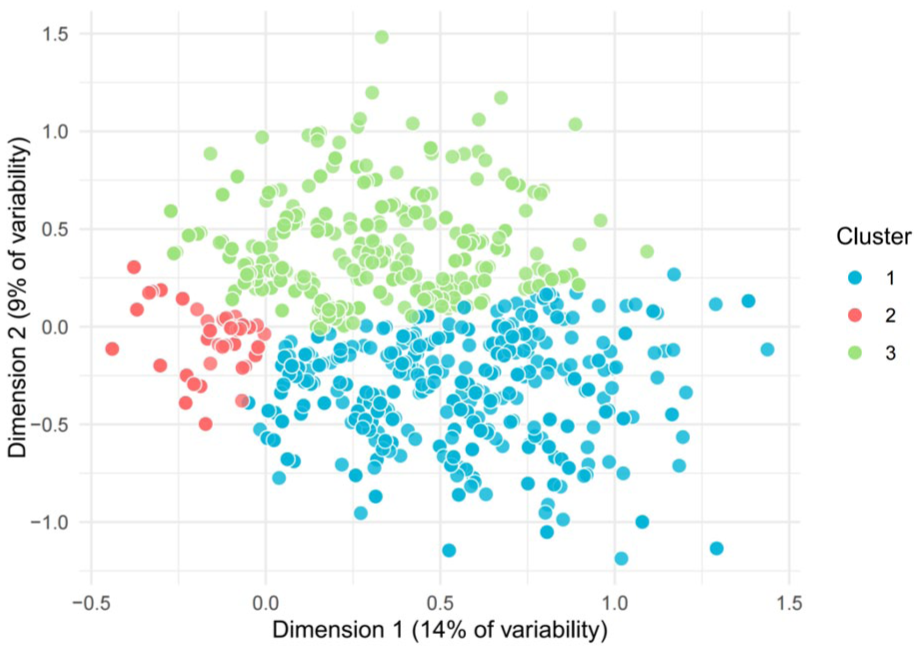
The visualization of K-Means clustering.
Baseline Characteristics
Supplemental Table 2 presents the baseline characteristics of participants by multimorbidity patterns. The 8778 participants had a mean age of 89.4 (SD 11.9), of whom 63.4% were female and 36.5% were male. Overall, participants were more likely to have lower educational levels (70.1% illiterate), be single (74.8%), live with household member(s) (83.9%), and lack exercise behavior (75.2%). Participants in the cardiovascular pattern (25.8 [SD 4.7]) and multisystem pattern (25.3 [SD 4.8]) had similar cognitive function scores, whereas those in the sensory pattern had lower scores (20.7 [SD 5.7]).
Cognitive Transitions in Multimorbidity Patterns
A total of 8778 participants completed a baseline survey and 2 follow-up assessments. Figure 2 presents the transitions observed during follow-up from the current cognitive state to the subsequent state. Compared to the sensory pattern, individuals in the cardiovascular pattern (HR 0.45, 95% CI [0.34, 0.60]) and the multisystem pattern (HR 0.48, 95% CI [0.37, 0.63]) had a lower risk of progressing from normal cognition to cognitive impairment. The cardiovascular pattern was associated with a 47% reduced risk of transitioning from dementia to death compared to the sensory pattern (95% CI [0.30, 0.94]). No significant differences were observed in the transition from cognitive impairment to normal cognition among individuals in the cardiovascular and multisystem patterns, using the sensory pattern as the reference (HR 0.83, 95% CI [0.60, 1.14]; HR 0.87, 95% CI [0.62, 1.22]).
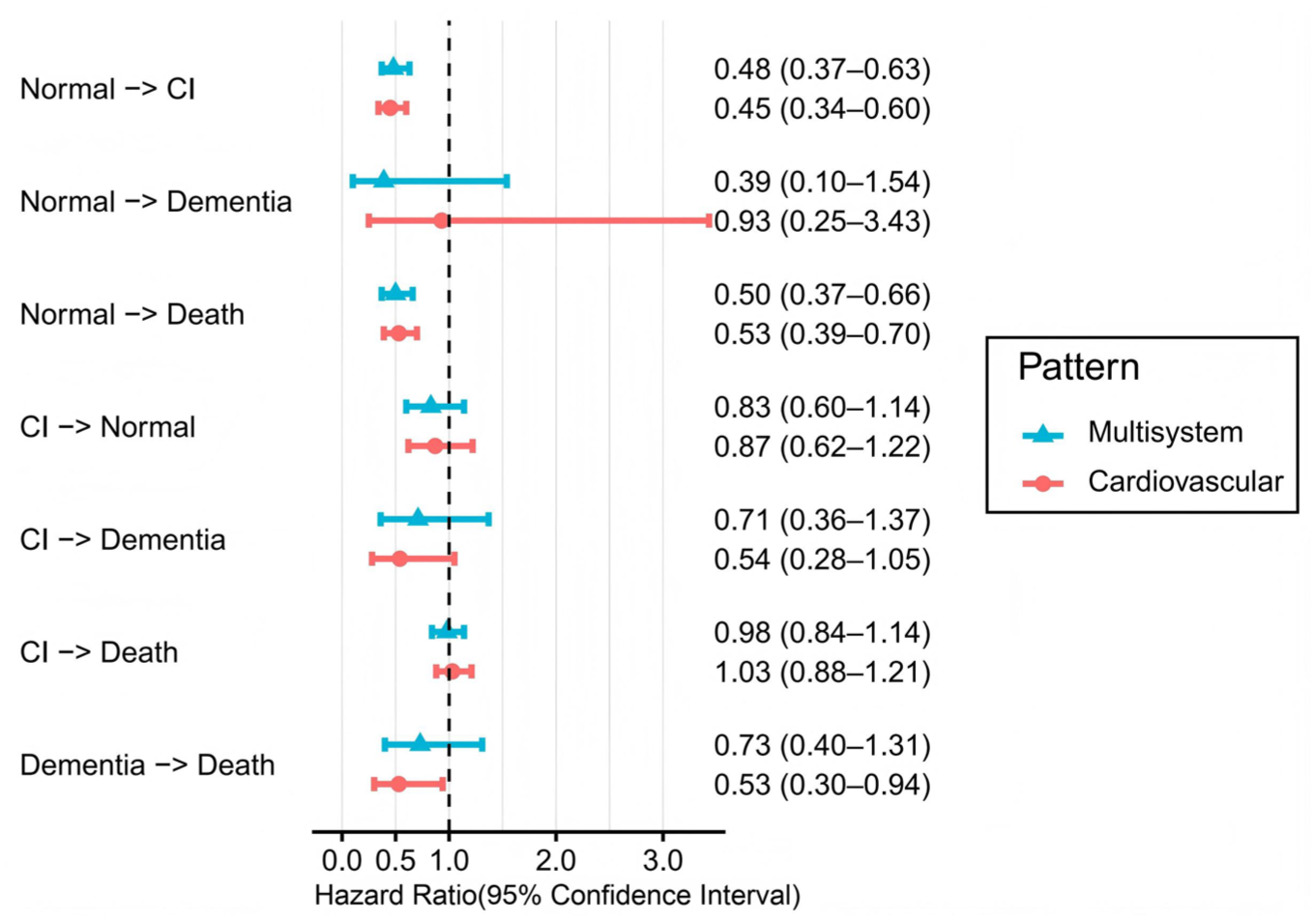
Effect of multimorbidity patterns on transitions across cognitive stages and death.
Sojourn Time of Cognitive Stages Across Multimorbidity Patterns
Figure 3 illustrates the sojourn times for participants with normal cognition who transition to cognitive impairment and dementia, stratified by disease pattern, age, and gender. We estimated these sojourn times for an average elderly individual—defined as someone who is illiterate, single, living with family members, and not engaging in exercise. Overall, compared to females with similar characteristics, males across all disease patterns generally experience shorter sojourn times in both the cognitively normal stage and in the progression to cognitive impairment or dementia, with these estimations being consistent across different age groups. In terms of disease patterns, among both males and females of different ages, the sojourn time for the cognitively normal stage in the sensory pattern is shorter than that in the cardiovascular and multisystem patterns. In the sensory pattern, the sojourn time in the cognitive impairment stage is longer in 80-year-old individuals (using females as an example: 1.96 years, 95% CI [1.89, 2.15]) compared to the other patterns (1.42 years, 95% CI [1.38, 1.61]; and 1.55 years, 95% CI [1.52, 1.73]). However, for individuals aged 90 and 100, the duration of cognitive impairment gradually converges with that observed in the other disease patterns. All estimated sojourn times from dementia to death are very short.
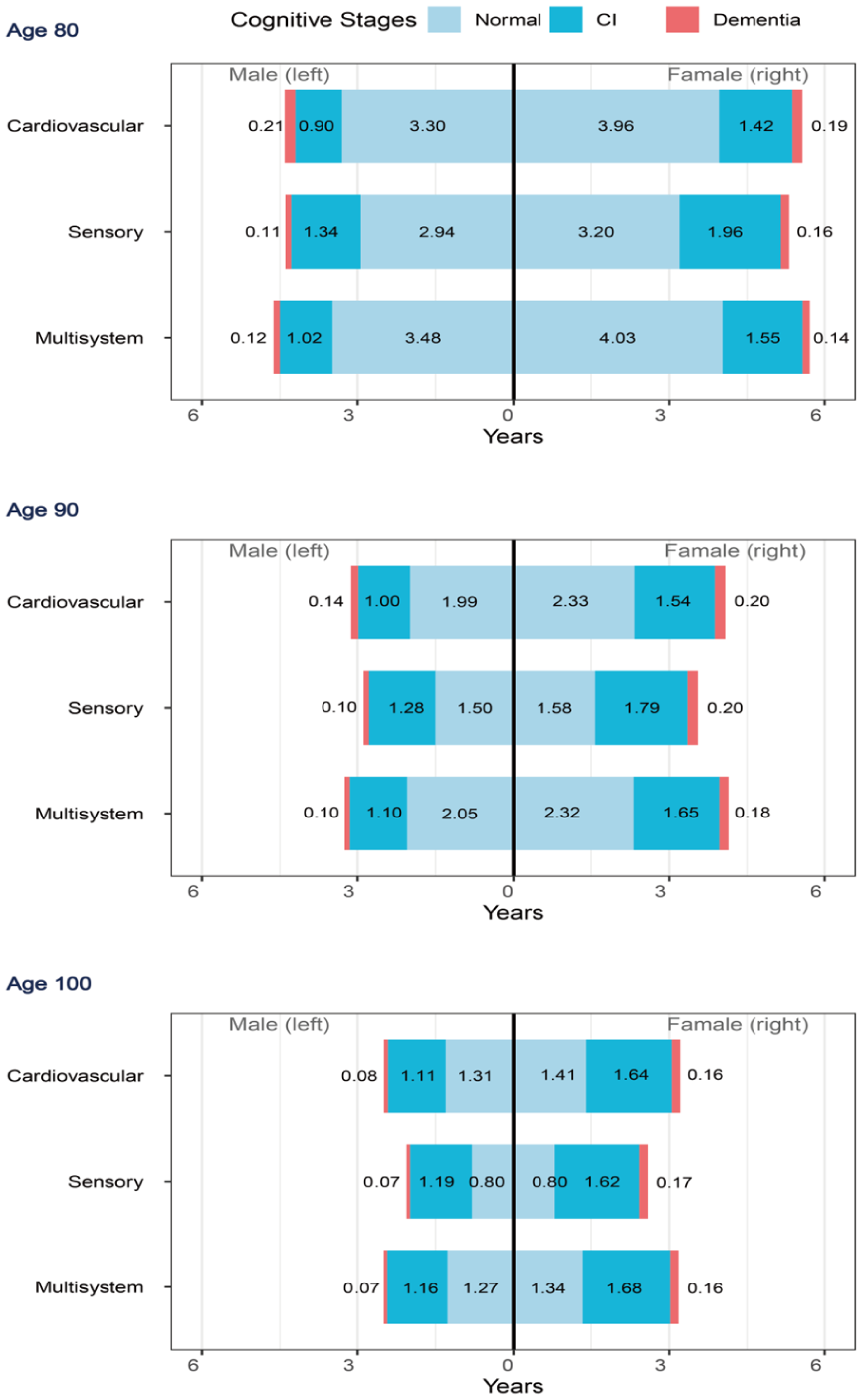
The estimated sojourn time of each cognitive stage.
Discussion
This study identified 3 multimorbidity patterns among the elderly populations in China. We investigated the risk of cognitive state transitions across these multimorbidity patterns, as well as estimated the sojourn times for progression through 3 stages—from normal cognition, to cognitive impairment, and finally from dementia to death.
The sensory pattern, characterized by visual impairment and hearing loss, exhibited a distinctive trajectory of cognitive decline among patients with multiple coexisting diseases. The substantially higher risk of transitioning from normal cognition to cognitive impairment in the sensory pattern is consistent with previous research among the elderly in China. 19 This may be closely related to the sensory-deprivation hypothesis, which posits that chronic lack of sensory input accelerates cognitive decline through multiple pathways. First, the additive loss of both visual and auditory input may lead to cortical atrophy in sensory and association areas, as reduced neural stimulation diminishes synaptic density and accelerates neurodegeneration. 25 Second, hearing loss might lead to impairments in cognitive and sensory functions mediated by the prefrontal cortex and auditory cortex, implicating potential structural and molecular mechanisms. 26 Third, individuals with dual sensory impairment often experience reduced social engagement, which further depletes cognitive reserve by limiting the complex cognitive demands of social interaction. In addition, the estimated sojourn time in the normal cognition stage was shorter in the sensory pattern, indicating that the loss of sensory function might hasten the initiation of cognitive decline. However, once cognitive impairment has developed, individuals in the sensory pattern tend to experience a longer duration of cognitive impairment than those in the other patterns. This finding may be partially explained by the fact that 74.7% of individuals in the sensory pattern were female. Previous studies have shown that females tend to experience a longer duration of cognitive impairment than males, 27 which implies that women may endure a longer period of symptomatic cognitive decline.
Patients in the cardiovascular pattern exhibited a lower risk of cognitive deterioration and mortality when compared to the sensory pattern, which is inconsistent with the results reported by Valletta et al. 28 A Swedish longitudinal study with an average participant age of 73.6 years found that individuals with a cardiovascular pattern had a 70% increased risk of progressing from “cognitive impairment, no dementia” to dementia (95% CI [1.15, 2.52]). This discrepancy may be attributed to survivor bias. Our study focused on Chinese elderly individuals, with an average age of 83 years in the cardiovascular pattern group. This suggests that these participants may represent robust survivors who possess stronger antiaging biological characteristics, such as better mitochondrial function, 29 and may have experienced less-severe cardiovascular conditions. Moreover, patients in the cardiovascular pattern often benefited from more standardized medical monitoring and treatment, including antihypertensive and lipid-lowering medications, which may exert neuroprotective effects by maintaining cerebral perfusion and reducing vascular damage to the blood-brain barrier. For instance, randomized trials have confirmed that intensified blood pressure management can reduce the risk of dementia by preserving cerebrovascular integrity. 30 Such health management may mitigate the negative impact of a single disease, suggesting that the overall risk associated with multimorbidity patterns is not merely a simple accumulation of individual disease risks but results from the interactions between disease combinations and behavioral factors.
The findings for the multisystem pattern were similar to those for the cardiovascular pattern, which may be due to the similar demographic characteristics observed in both clusters. A higher proportion of married individuals and those with regular exercise habits was noted in the multisystem pattern. Existing research indicates that being married, especially accompanied by a spouse, is associated with better cognitive function, while unmarried individuals, including those who are single, divorced, or widowed, exhibit a higher risk of cognitive impairment. 31 In addition, long-term physical exercise can delay the progression of cognitive decline in patients with mild cognitive impairment (MCI) or dementia, with significant benefits observed in overall cognition, executive function, and memory. 32 From a mechanistic standpoint, systemic inflammation likely plays a role in the multisystem pattern. The co-occurrence of respiratory and metabolic conditions typically induces a chronic inflammatory state (e.g., elevated IL-6, CRP), which damages the blood-brain barrier and promotes neurodegeneration.
It is unsurprising that the sojourn times from dementia to death were very short across all disease patterns, aligning with previous studies. 25 However, the sojourn times estimated in the present study were even shorter, which may relate to the demographic variables chosen when calculating these durations. Specifically, the computations were based on the average levels of each variable—namely, individuals who were illiterate, single, living with household member(s), and lacking exercise habits. These factors might have contributed to the shorter sojourn times observed.
This study is the first to utilize data from CLHLS, a prospective longevity cohort, to explore the impact of multimorbidity patterns on cognitive states through a multistate Markov model among the Chinese elderly. Our research confirmed the existence of 3 disease patterns and quantified the risks of transitions between various cognitive states associated with each pattern. This study also has several limitations. First, the study participants were followed up every 3 years; thus, we were unable to capture the exact onset times of disease, limiting our ability to pinpoint the precise timing of cognitive state transitions. Second, although potential confounding factors such as age, gender, and education were incorporated when fitting the multistate Markov model, there may still be unmeasured confounding variables. Finally, we employed a multistate Markov model which assumes that the probability of future transitions depends solely on the current state (Markov assumption). While we relaxed the time-homogeneity assumption by including age as a time-dependent covariate to reflect changing risks over the life course, we did not perform formal goodness-of-fit tests. This remains a common limitation in similar epidemiological modeling.
Conclusion
In this study, using a multistate Markov model, we confirmed that the effects of different multimorbidity patterns on cognitive state transitions among the elderly are heterogeneous, with the sensory pattern representing a high-risk type for cognitive decline. The findings not only deepen our understanding of the relationship between multimorbidity and cognition but also provide actionable stratified intervention targets for managing cognitive health in older adults.
Supplemental Material
sj-docx-1-aph-10.1177_10105395261456803 – Supplemental material for Multimorbidity Patterns and Cognitive Transitions Among the Elderly in China: The Longitudinal Evidence From CLHLS
Supplemental material, sj-docx-1-aph-10.1177_10105395261456803 for Multimorbidity Patterns and Cognitive Transitions Among the Elderly in China: The Longitudinal Evidence From CLHLS by Jinglin Huang, Jixiang Yang, Yiren Song, Haochen Zhai, Kexin Guo, Fangyu Zhou, Xiaojun Hu and Zhihao Xu in Asia Pacific Journal of Public Health
Supplemental Material
sj-docx-2-aph-10.1177_10105395261456803 – Supplemental material for Multimorbidity Patterns and Cognitive Transitions Among the Elderly in China: The Longitudinal Evidence From CLHLS
Supplemental material, sj-docx-2-aph-10.1177_10105395261456803 for Multimorbidity Patterns and Cognitive Transitions Among the Elderly in China: The Longitudinal Evidence From CLHLS by Jinglin Huang, Jixiang Yang, Yiren Song, Haochen Zhai, Kexin Guo, Fangyu Zhou, Xiaojun Hu and Zhihao Xu in Asia Pacific Journal of Public Health
Supplemental Material
sj-docx-5-aph-10.1177_10105395261456803 – Supplemental material for Multimorbidity Patterns and Cognitive Transitions Among the Elderly in China: The Longitudinal Evidence From CLHLS
Supplemental material, sj-docx-5-aph-10.1177_10105395261456803 for Multimorbidity Patterns and Cognitive Transitions Among the Elderly in China: The Longitudinal Evidence From CLHLS by Jinglin Huang, Jixiang Yang, Yiren Song, Haochen Zhai, Kexin Guo, Fangyu Zhou, Xiaojun Hu and Zhihao Xu in Asia Pacific Journal of Public Health
Supplemental Material
sj-jpg-3-aph-10.1177_10105395261456803 – Supplemental material for Multimorbidity Patterns and Cognitive Transitions Among the Elderly in China: The Longitudinal Evidence From CLHLS
Supplemental material, sj-jpg-3-aph-10.1177_10105395261456803 for Multimorbidity Patterns and Cognitive Transitions Among the Elderly in China: The Longitudinal Evidence From CLHLS by Jinglin Huang, Jixiang Yang, Yiren Song, Haochen Zhai, Kexin Guo, Fangyu Zhou, Xiaojun Hu and Zhihao Xu in Asia Pacific Journal of Public Health
Supplemental Material
sj-jpg-4-aph-10.1177_10105395261456803 – Supplemental material for Multimorbidity Patterns and Cognitive Transitions Among the Elderly in China: The Longitudinal Evidence From CLHLS
Supplemental material, sj-jpg-4-aph-10.1177_10105395261456803 for Multimorbidity Patterns and Cognitive Transitions Among the Elderly in China: The Longitudinal Evidence From CLHLS by Jinglin Huang, Jixiang Yang, Yiren Song, Haochen Zhai, Kexin Guo, Fangyu Zhou, Xiaojun Hu and Zhihao Xu in Asia Pacific Journal of Public Health
Footnotes
Acknowledgements
We gratefully acknowledge the CLHLS for providing data and all participants for their contributions.
Ethical Considerations
This study was based on publicly available data from the Chinese Longitudinal Healthy Longevity Survey (CLHLS). The CLHLS study was approved by the Ethics Committee of Peking University (IRB00001052–13074).
Consent to Participate
All participants or their representatives in the CLHLS study signed the informed consent.
Consent for Publication
Not applicable.
Author Contributions
Jinglin Huang: conceptualization, methodology, formal analysis, writing–original draft; Jixiang Yang: methodology, formal analysis; Yiren Song: formal analysis; Haochen Zhai: editing; Kexin Guo: data processing; Fangyu Zhou: data processing; Xiaojun Hu: conceptualization, writing—review & editing, supervision; Zhihao Xu: conceptualization, writing—review & editing, supervision.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Vanguard Leading Goose Project of Zhejiang Provincial Department of Science and Technology (2025C02105).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Supplemental Material
Supplemental material for this article is available online.
Any Other Identifying Information Related to the Authors and/or Their Institutions,Funders,Approval Committees,etc,That Might Compromise Anonymity
This information has been removed.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.