
Abstract
Obesity is a risk factor for hypercholesterolemia; however, evidence of obesity among Orang Asli (OA) adults remains limited. Lifestyle changes, including unhealthy diets and sedentary behavior, may increase vulnerability to noncommunicable diseases. This study examined the sex-specific associations between body mass index (BMI) and hypercholesterolemia using data from the OA Health Survey 2022. A total of 8160 adults aged ≥18 years with complete questionnaires, anthropometric data, and blood data were analyzed. The prevalence of hypercholesterolemia among OA adults was 47.6%; of these, 41.5% were previously undiagnosed. Compared with normal BMI, overweight and obesity were associated with a higher odds of hypercholesterolemia in both sexes. Older age, Senoi tribe affiliation, and diabetes were associated with hypercholesterolemia in both sexes. These findings highlight the need for culturally tailored interventions to strengthen obesity prevention and cholesterol testing in primary care and outreach services to reduce cardiovascular risk in OA communities.
Keywords
What We Already Know
Obesity is a key, modifiable risk factor for hypercholesterolemia, ischemic heart disease, and other cardiometabolic conditions.
The Orang Asli population is undergoing lifestyle transitions, including dietary changes and reduced physical activity, which increase their risk of noncommunicable diseases.
Existing research on Orang Asli health is limited, particularly on how body mass index relates to hypercholesterolemia within this unique genetic and sociocultural group.
What This Article Adds
Confirms a strong association between elevated BMI and hypercholesterolemia among Orang Asli men and women using recent population-based survey data.
Identifies specific high-risk groups, including individuals aged 50 to 59 and members of the Senoi tribe, highlighting the importance of tailored public health strategies.
Reveals a high prevalence of undiagnosed hypercholesterolemia (41.5%), underscoring the urgent need for targeted, culturally sensitive screening and intervention.
Introduction
Cardiovascular disease (CVD) is the leading cause of death worldwide, with ischemic heart disease being responsible for half of deaths due to CVD.1,2 Major risk factors for CVD include dyslipidemia, high blood glucose level, high blood pressure, and other factors. 2 In Malaysia, findings from the National Health and Morbidity Survey 2023 showed an increasing prevalence of diabetes over the past decade, accompanied by similar increases in overweight, obesity, and abdominal obesity.3 -5
Orang Asli (OA), Indigenous peoples of Peninsular Malaysia, experience distinct sociocultural, economic, and health-related challenges, and they may also have unique demographic and genetic characteristics.6,7 Traditionally, OA engage in subsistence farming, hunting, gathering, and agriculture. 8 Over time, they have transitioned to a more modern lifestyle through government incentives aimed at improving access to education, health care, and economic well-being. 8 These demographic shifts have led to epidemiological transitions, contributing to an increase in noncommunicable diseases (NCDs). 8 Increasing exposure to unhealthy diets and sedentary lifestyles may predispose OA communities to obesity and related metabolic disorders, including hypercholesterolemia.9 -11
Although the government has introduced structured resettlement programs, many OA communities remain in remote ancestral areas with limited access to health care, nutritional services, and health promotion. 9 This restricted access may limit prevention, screening, early detection, and management of hypercholesterolemia, obesity, and other NCDs. Hypercholesterolemia is a key modifiable risk factor for CVD, and this relationship is well established in the general population. 1 Although obesity and metabolic disorders are increasing among OA communities, few studies have specifically examined this population. Understanding the association between body mass index (BMI) and hypercholesterolemia, along with other associated factors, is essential for developing culturally appropriate prevention and screening programs to reduce cardiovascular risk in this vulnerable population. Therefore, this study aimed to examine the association between BMI and hypercholesterolemia and identify other factors associated with elevated cholesterol levels in sex-stratified analyses.
Methods
Data Source and Population
This study used secondary data obtained from the OA Health Survey 2022, a cross-sectional population-based survey conducted from July 20, 2022, to September 13, 2022. 12 Orang Asli respondents aged 18 years and older were included.
This study was conducted across 9 states in Peninsular Malaysia, focusing on marginalized OA communities. The sampling framework was derived from the Department of Orang Asli Development (JAKOA). The states included Selangor, Perak, Kedah, Melaka, Negeri Sembilan, Johor, Kelantan, Terengganu, and Pahang. In total, 853 Orang Asli villages were identified in Peninsular Malaysia, of which 68 villages were randomly selected using a stratified sampling approach. 12 The primary stratum comprised 3 localities: urban, fringe, and remote areas across 9 states in Peninsular Malaysia where the OA reside. 12 The secondary stratum was based on tribal affiliation and consisted of the Senoi, Proto-Malay, and Negrito tribes. 12 A total of 4141 living quarters and 15 950 respondents completed the survey, yielding an overall response rate of 89.8%. Further details on the survey methodology and sampling design have been published elsewhere. 12
All living quarters in the selected villages were included in this study. Individuals who had resided there for at least 2 weeks prior to data collection were considered eligible for the study.
Instrument
The questionnaire was adopted from the following validated instruments:
The World Health Organization (WHO) STEPwise Approach to NCD Risk Factor Surveillance questionnaire,12,13
The Alcohol Use Disorders Identification Test for alcohol consumption,12,14 and
A modified version of the Global Adult Tobacco Survey for tobacco use. 12
Data collection was performed face-to-face and via self-administration. For clinical assessments, the calibrated CardioChek PA device (PTS Diagnostics), a validated point-of-care analyzer, was used to measure fasting capillary glucose and cholesterol levels. Its diagnostic accuracy for lipid measurement in epidemiological surveys has been previously reported. 15 Respondents were instructed to fast for at least 8 hours before blood sampling. 12 For anthropometric measurements, height was measured using the SECA 213 stadiometer, weight was assessed using the SECA 813 weighing scale, and waist circumference was measured using the SECA 201 measuring tape. 12 All devices were calibrated according to the manufacturers’ specifications prior to data collection.
Indicator Definitions
The main exposure variable was BMI, which was calculated using the following formula: BMI = weight in kilogram/height in meters 2 . According to the WHO 1998 classification, BMI was categorized as underweight (<18.5 kg/m2), normal (18.5-24.9 kg/m2), overweight (25.0-29.9 kg/m2), and obese (≥30.0 kg/m2). 12
Hypercholesterolemia was defined as either a self-reported prior diagnosis by a health care professional or total cholesterol (TC) ≥5.2 mmol/L among respondents without a prior diagnosis at the time of the survey. The outcome was coded as a binary variable (1 = hypercholesterolemia, 0 = no hypercholesterolemia). 12
Other sociodemographic and lifestyle characteristics were considered as potential confounders a priori. The variables retained in the final sex-stratified multivariate models are listed in the statistical analysis section. Diabetes was defined as having a fasting blood glucose level ≥7.0 mmol/L or, for participants who were not fasting, a random blood glucose level ≥11.1 mmol/L at the time of survey. 12 Current tobacco use was defined as currently using any tobacco product (manufactured cigarettes, hand-rolled cigarettes, kretek, cigars, shisha, bidis, tobacco pipes, e-cigarettes, and chewed tobacco/snuff). 12 Current drinkers were defined as those who had consumed any alcoholic beverage in the past 12 months. 12 Tobacco and alcohol variables were considered as potential behavioral covariates because they are established risk factors for cardiovascular and metabolic diseases. 16
Quality Control Measures
Quality control was a crucial component of the survey. A training workshop for the data collectors was organized to clarify the study objectives, standardize the completion of survey forms via mobile applications using tablets, and familiarize field teams with the survey protocols. 12
The questionnaire included programmed skip patterns and validation rules to ensure that only appropriate responses were accepted, thereby reducing data entry errors. An offline Survey Creation System was used for data collection, enhancing data accuracy and security. 12 Comprehensive training was provided to minimize bias and maintain high standards of data collection.
Statistical Analysis
Missing data were handled using a complete case analysis. Complex sample logistic regression analysis was used to account for the survey design using a complex sample plan file. Categorical variables were analyzed using the complex sample crosstabs procedure, and associations were assessed using the design-based Wald F-test. Sex-specific analyses were performed by fitting separate multivariable models for men and women (sex-stratified models) to estimate the adjusted odds ratios (aORs) and 95% confidence intervals (CIs). The final multivariate models included age group, BMI category, tribe, diabetes status, and marital status (sex-stratified). Potential 2-way interactions were explored by adding interaction terms one at a time and evaluating design-based Wald F-tests. Interaction terms were retained only if they were statistically meaningful and interpretable. Statistical Product and Service Solutions (version 29.0; IBM Corp.) was used for data cleaning and analysis. A P value of <.05 was considered statistically significant.
Ethical Considerations
Information sheets were provided to all eligible respondents, and written informed consent was obtained before the interview sessions. Ethical approval was obtained from the Medical Research and Ethics Committee (approval number: KKM/NIHSEC/P-19-2592[11]) of the Ministry of Health Malaysia and JAKOA. 12
Results
Respondent Characteristics
The study initially included 8823 OA respondents aged 18 years and older. After excluding those with incomplete data, 8160 respondents were retained for analysis, comprising 3559 men (43.2%) and 4601 women (56.8%) (Table 1).
Characteristics of the Orang Asli Adult Population by Hypercholesterolemia Status (N = 8160).
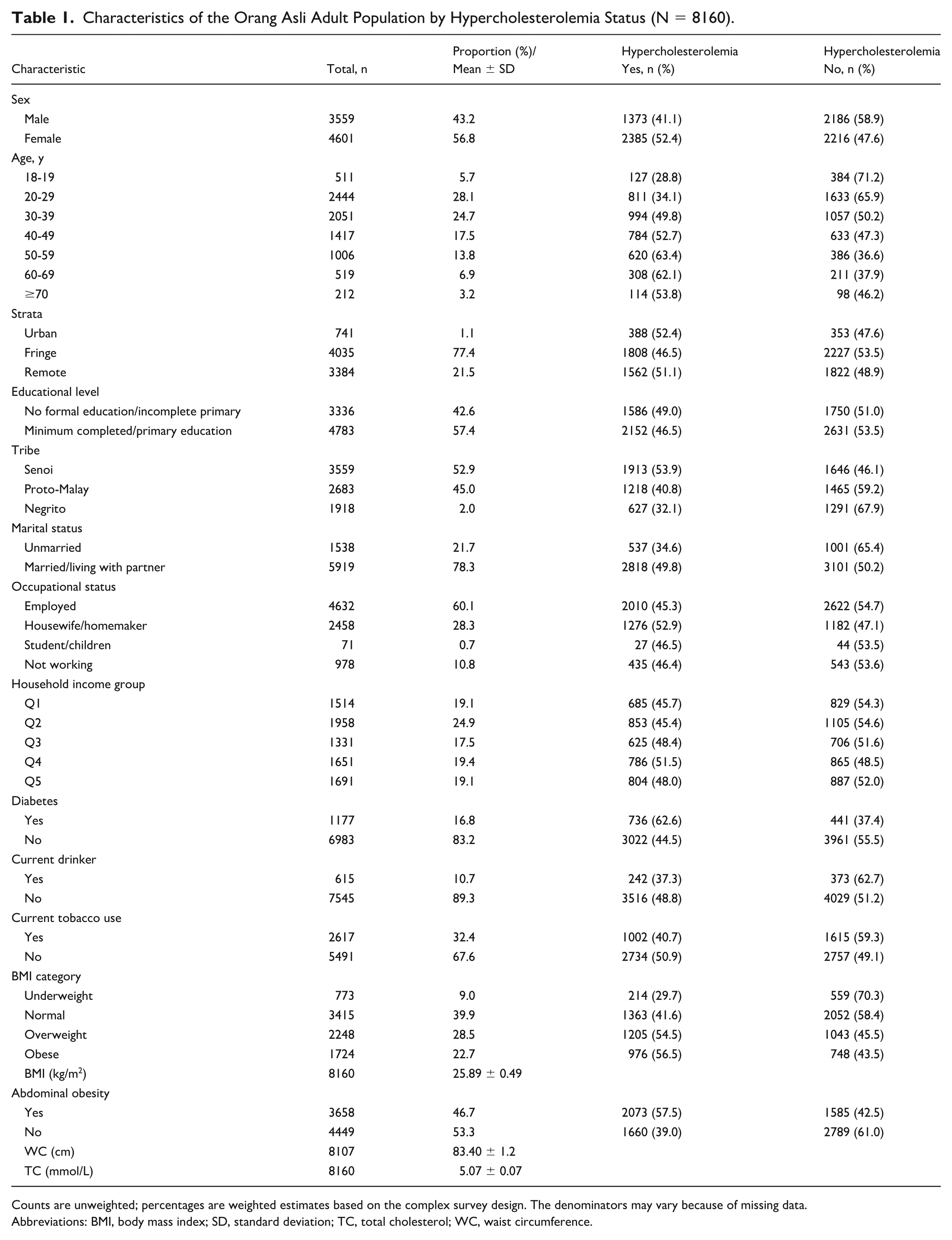
Counts are unweighted; percentages are weighted estimates based on the complex survey design. The denominators may vary because of missing data.
Abbreviations: BMI, body mass index; SD, standard deviation; TC, total cholesterol; WC, waist circumference.
More than half (52.8%, n = 4495) of the respondents were aged 20 to 39 years, belonged to the Senoi tribe (52.9%), and had completed at least one primary education (57.4%). Most respondents were married or living with a partner (78.3%) and were employed (60.1%) (Table 1).
Prevalence of Hypercholesterolemia
The prevalence of hypercholesterolemia among OA adults was 47.6%. Of these, 6.1% were previously diagnosed, and 41.5% were undiagnosed.
Factors Associated With Hypercholesterolemia
As shown in Table 2, the Wald F-test revealed significant differences in the prevalence of hypercholesterolemia according to sex, age group, tribe, marital status, occupation, diabetes status, current tobacco use, current drinking status, and BMI (all P < .05). Conversely, strata, education level, and household income quintiles showed no significant differences (all P > .05). According to BMI categorization, more than half of the overweight (54.5%) and obese (56.5%) respondents had hypercholesterolemia compared with those in the normal (41.6%) and underweight (29.7%) categories.
Univariate Analysis Results of Variables Associated With Hypercholesterolemia Among Orang Asli Adults (N = 8160).
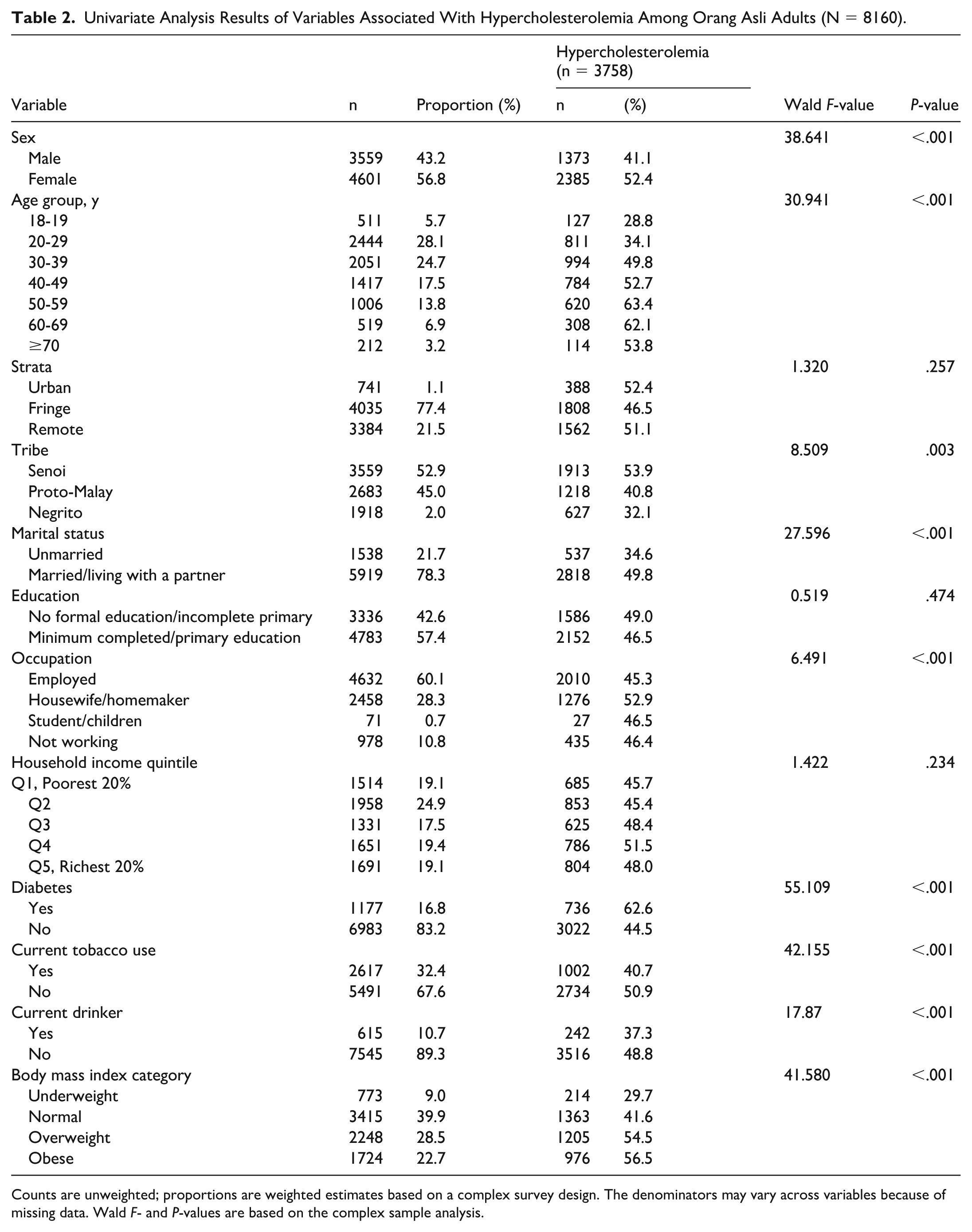
Counts are unweighted; proportions are weighted estimates based on a complex survey design. The denominators may vary across variables because of missing data. Wald F- and P-values are based on the complex sample analysis.
Association Between BMI and Hypercholesterolemia by Sex
Multiple logistic regression analysis demonstrated an association between the BMI category and odds of hypercholesterolemia after adjusting for age, tribe, marital status, and diabetes status in sex-stratified models (Table 3).
Factors Associated With Hypercholesterolemia According to Sex Among Orang Asli Adults (N = 8160).
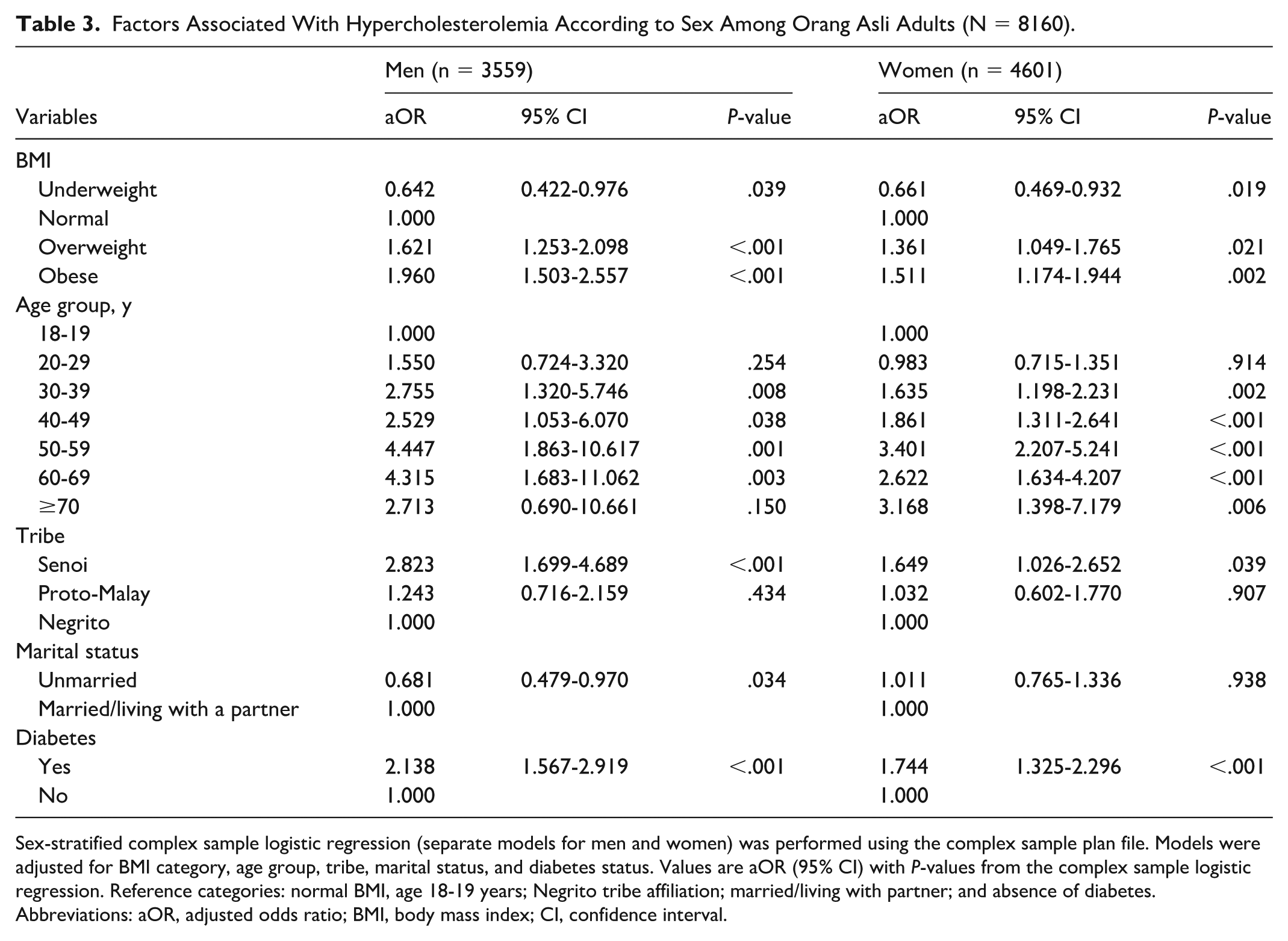
Sex-stratified complex sample logistic regression (separate models for men and women) was performed using the complex sample plan file. Models were adjusted for BMI category, age group, tribe, marital status, and diabetes status. Values are aOR (95% CI) with P-values from the complex sample logistic regression. Reference categories: normal BMI, age 18-19 years; Negrito tribe affiliation; married/living with partner; and absence of diabetes.
Abbreviations: aOR, adjusted odds ratio; BMI, body mass index; CI, confidence interval.
Body mass index was significantly associated with hypercholesterolemia in both sexes (Table 3). Compared with men with normal BMI, overweight men (aOR = 1.62, 95% CI [1.25-2.10]) and obese men (aOR = 1.96, 95% CI [1.50-2.56]) had markedly higher odds of hypercholesterolemia. Similarly, overweight women (aOR = 1.36, 95% CI [1.05-1.77]) and obese women (aOR = 1.51, 95% CI [1.17-1.94]) showed significantly higher odds.
Other Associated Covariates
Several covariates were associated with hypercholesterolemia. The odds increased with age, peaking among those aged 50 to 59 years for both sexes. The Senoi tribe had significantly higher odds than the Negrito tribe, and the odds were higher among respondents with diabetes. Among men only, being married was associated with a higher odds of hypercholesterolemia. Education level, strata, and household income quintiles were not significantly associated with hypercholesterolemia in univariate analysis and were not retained in the final multivariate models.
Discussion
This study demonstrated that nearly half of OA adults had hypercholesterolemia, a prevalence considerably higher than that of the general Malaysian population (33.3%). 4 Of particular concern, 41.5% of OA adults had undiagnosed hypercholesterolemia, indicating a substantial gap in screening and detection. 12 This undiagnosed burden appears higher than that reported in the general Malaysian adult population (18.1%), suggesting that OA communities may face a double burden of elevated cardiometabolic risk and limited access to early detection and preventive care.4,12
Several contextual factors might have contributed to this pattern. Despite government efforts to improve health, education, and employment access, cultural beliefs and traditional practices still strongly influence health behaviors and treatment-seeking patterns. 9 Simultaneously, lifestyle transitions associated with modernization, including less healthy diets and sedentary lifestyles, have been linked to increasing metabolic disorders among OA communities and other Indigenous populations.9-11,17 Together, these factors may increase cardiometabolic risk while limiting opportunities for early detection.
The key finding of this study is the strong association between BMI and hypercholesterolemia in both sexes, suggesting that BMI is an independent factor associated with hypercholesterolemia among OA adults. Compared with those with normal BMI, overweight and obese adults had significantly higher odds of hypercholesterolemia, with obesity nearly doubling the odds among men and increasing by 50% among women. This pattern is consistent with that in other Malaysian studies showing higher odds of hypercholesterolemia among overweight and obese adults, although effect sizes vary by population and sex.18,19 The somewhat stronger association observed among men may reflect sex-related differences in the metabolic response to obesity. Evidence suggests that, in the presence of obesity, men may have lower adipocyte insulin sensitivity, reduced antilipolytic response to insulin, and higher basal lipolysis than women, which may partly explain the sex differences in metabolic risk. 20 However, these mechanisms were not directly examined in the present study. Biologically, excess adiposity may contribute to dyslipidemia through insulin resistance, increased free fatty acid flux, and hepatic overproduction of lipids. 21 Obesity is also associated with chronic low-grade inflammation, oxidative stress, and atherogenic alterations in lipoprotein metabolism, which may further worsen lipid profiles and contribute to hypercholesterolemia risk.21 -24 Overall, these findings reinforce obesity as a central and modifiable target for preventing hypercholesterolemia among OA adults.
Other factors were also associated with hypercholesterolemia; however, BMI showed the strongest and most consistent association with hypercholesterolemia. The higher odds observed among Senoi compared with Negrito may reflect heterogeneity in cardiometabolic profiles across Orang Asli tribes and sub-tribes, as previous studies have shown that risk patterns vary by sub-tribe, settlement type and degree of urbanization.8,11 This may be partly explained by differences in urbanization and socioeconomic conditions. Some Senoi sub-tribes, particularly those in resettled or urban-exposed areas, may have greater exposure to sedentary lifestyles and dietary change, whereas the Negrito groups are more often described as inland or traditionally hunter-gatherer communities, with some groups remaining more remote and maintaining traditional subsistence practices.8,9,11 Age was associated with hypercholesterolemia, with adults aged 50 to 59 years showing the highest odds in our analysis, which may reflect cumulative metabolic exposure and age-related changes in lipid metabolism and regulation.25,26 Diabetes was also associated with hypercholesterolemia in both sexes, consistent with the clustering of cardiometabolic risk factors and shared underlying mechanisms, particularly insulin resistance and diabetes-related dyslipidemia.21,27,28
Among men, being married was associated with higher odds of hypercholesterolemia; however, this finding should be interpreted cautiously as the cross-sectional design does not permit conclusions regarding the direction or underlying mechanism of this association. In addition, residual confounding factors cannot be excluded.
From a public health perspective, the high prevalence and substantial undiagnosed burden highlight the need to strengthen cholesterol screening and cardiovascular risk prevention in OA communities. Interventions should prioritize healthy weight management and early cholesterol testing, with particular attention to higher risk groups, such as adults aged 50 to 59 years and communities with higher risk profiles. Outreach-based screening and linkages to care may be particularly important in rural and remote settlements with limited access to services. Therefore, integrating cholesterol screening with the prevention and control of diabetes is critical. These programs should be culturally tailored and supported by partnerships with OA communities to improve acceptability, feasibility, and sustainability. 10
Limitations and Future Research
This study has some limitations. Its cross-sectional design precludes causal inference between BMI and hypercholesterolemia. Total cholesterol was assessed using point-of-care capillary testing rather than laboratory-based venous assays, which are the reference method for lipid measurement.12,15 As agreement between capillary and venous measurements has been reported to be only moderate (0.64-0.67), 15 some degree of measurement error or misclassification may have occurred. In addition, some behavioral factors (eg, smoking and alcohol consumption) were self-reported and may be subject to recall or reporting bias. Although multiple covariates were adjusted, residual confounding from unmeasured variables could not be ruled out. Finally, the findings are specific to the OA population and provide important insights for Indigenous health policy in Malaysia. However, given the distinct sociocultural and genetic background of OA communities, the results should be interpreted in this context and are not intended to be generalized to other populations in Malaysia.
The findings of the present study highlight the need for culturally tailored interventions to strengthen obesity prevention and cholesterol testing in primary care and outreach services to reduce cardiovascular risk in OA communities. Future longitudinal studies are needed to establish temporal and causal relationships. Further work exploring the genetic, cultural, and environmental determinants relevant to Orang Asli communities would also provide deeper insights into the mechanisms underlying the risk of hypercholesterolemia. Finally, intervention-based studies are warranted to evaluate the effectiveness of culturally tailored strategies in reducing obesity and improving lipid profiles in this population.
Footnotes
Acknowledgements
We would like to thank the Director General of Health Malaysia for permission to publish this article. We also acknowledge Sage Author Services for providing English language editing assistance to improve the clarity and readability of the manuscript.
Ethical Considerations
Ethical approval was obtained from the Medical Research and Ethics Committee (approval number: KKM.NIHSEC/P-19-2592(11)) of the Ministry of Health Malaysia and Department of Orang Asli Development.
Consent to Participate
An information sheet was provided to all eligible respondents, and written informed consent was obtained from the respondents who agreed to participate in the survey before the interview session commenced.
Author Contributions
HMR contributed to the conceptualization, methodology, visualization, original draft writing, analysis, and final manuscript review and editing. WKS contributed to the conceptualization, methodology, analysis, and review and editing of the final manuscript. HI, TGRL, KHA, and MRR contributed to manuscript review and editing. All the authors contributed to the manuscript and approved the submitted version.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This survey was funded by the Ministry of Health Malaysia research grant.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data supporting this study are available from the Institute for Public Health, Ministry of Health, Malaysia; however, access is restricted because the data are not publicly available. They can be obtained upon reasonable request and with permission from the Director General of Health Malaysia.