
Abstract
Despite its prevalence, the health care burden of co-occurring physical, psychological, and cognitive (PPC) disorders remains unclear. This study examines impact of different PPC-multimorbidity patterns on health care utilization and costs among 12 643 middle-aged and older Chinese adults using longitudinal data (China Health and Retirement Longitudinal Study 2011-2020). We measured outpatient/inpatient utilization (any visit/number of visits) and out-of-pocket (OOP) costs via self-reports. Binary, count, and censored outcomes were analyzed using mixed-effects logistic, negative binomial, and Tobit regressions, respectively. Results showed that PPC-multimorbidity significantly increased outpatient/inpatient utilization and OOP costs (ORoutpatient visit = 1.43, IRRoutpatient visit number = 1.41, ORinpatient visit = 1.73, IRRinpatient visit number = 1.53, IRRhospitalization days = 1.71, βoutpatient costs = 24.96, βinpatient costs = 353.02; P < .001). Increasing coexisting PPC types progressively amplified health care burden (dose-response P-trend < .001). Pattern-specific analyses demonstrated heterogeneous impacts, with nearly all PPC-multimorbidity combinations elevating health care demands. In conclusion, PPC-multimorbidity imposes a substantial health care burden. These findings advance multimorbidity conceptualization beyond simple disease counts, emphasizing the need to address distinct multimorbidity patterns and their complex interactions.
What We Already Know
Multimorbidity prevalence rises sharply with aging.
Traditional multimorbidity definitions overlook psychological-cognitive interactions.
PPC-multimorbidity risk factors are emerging but consequences remain unclear.
What This Article Adds
PPC-multimorbidity resulted in significantly higher health care use and costs.
A dose-response link exists between coexisting disease types and health care burden.
Distinct PPC-multimorbidity patterns had differential impacts on health care outcomes.
Introduction
The acceleration of global population aging coincides with an epidemiological transition characterized by a rising burden of chronic non-communicable diseases (NCDs), including cardiovascular diseases, malignant neoplasms, chronic respiratory diseases, musculoskeletal diseases, and neurological and mental disorders.1,2 Multimorbidity (≥2 concurrent chronic conditions) has emerged as a major public health challenge. 3 It is important to note that this rising burden is primarily an absolute increase driven by population aging. However, trends in age-adjusted prevalence, which remove the confounding effect of age structure, reveal that the increase is not solely due to demographic shifts; rather, the epidemiology of multimorbidity is also influenced by changes in risk factor exposures over time, showing a gradual increase in recent years.4,5 A recent systematic review estimated the global prevalence of multimorbidity was estimated at 37.2% among community-dwelled adults, 4 rising to over 50% in older adults aged 60 and older. 4 This challenge is particularly acute in China, home to the world’s largest aging population, where approximately 56.73% of middle-aged and older people are affected by comorbid conditions, 6 placing exceptional strain on its health care system. 7 Although the specific list of chronic diseases used to define multimorbidity varied across studies, consensus exists that multimorbid interactions amplify disease complexity, leading to adverse outcomes like higher mortality or disability, diminished quality of life, and elevated health care costs.8,9
Traditionally, disease diagnosis and management have been restricted to single physical disorders and their corresponding treatments, often excluding psychological and psychiatric factors, which can significantly complicate the comprehensive disease management process. Despite extensive literature exploring the prevalence, risk factors, and consequences of multimorbidity, available studies still simplistically count coexisting conditions across some or all of the physical, psychological, and cognitive (PPC) domains, without considering the specific patterns of these disease combinations. Physical-psychological-cognitive multimorbidity, defined as a simultaneous presence or intersection of 3 disease types (PPC disorders), represents a pressing yet understudied area of aging. Integrating psychological and cognitive dimensions is crucial, as their co-occurrence with physical conditions forms a distinct, high-burden phenotype with complex interactions. 10 Although still rare, a growing body of recent research has started to explore PPC-multimorbidity, identifying certain risk factors contributing to its incidence such as lower socioeconomic status, unhealthy lifestyle behaviors, and indoor solid-fuels use.10-12 However, the potential consequences associated with specific combinations of PPC-multimorbidity remain poorly understood.
Traditionally defined multimorbidity is recognized as a significant obstacle for international health systems. 13 Numerous studies have revealed that the co-occurrence of 2 or more chronic diseases is significantly associated with higher outpatient visits, hospital admissions, emergency department visits, long-term care services, and medical costs compared with having a single or no chronic disease.14-16 However, existing literature has predominantly adopted a narrow definition of multimorbidity, focusing on physical multimorbidity (eg, diabetes coupled with hypertension)16-18 while marginalizing psychological and cognitive dimensions. Little is known about how PPC-multimorbidity patterns longitudinally affect health care utilization and costs despite high disease clustering (PPC disorders amplifying complexity, complicating management, and exacerbating disparities). In China, the nationwide implementation of the diagnosis-related groups and diagnosis-intervention packet payment systems, alongside broad coverage of basic medical insurance, has fundamentally reshaped health care financing and reduced patients’ overall financial burden.19,20 Because a significant portion of institutional costs is now absorbed by the insurance pool, it is imperative to evaluate the residual economic impact on individuals, measured by the out-of-pocket (OOP) payment ratio. Characterizing multimorbidity by both condition count and specific interaction patterns is therefore crucial for understanding how distinct PPC disease clusters drive health care resource use and determine patients’ final OOP costs. To address this gap and inform precision health policies, this study investigates the longitudinal associations of distinct PPC-multimorbidity profiles with health care utilization and costs using a nationwide sample of Chinese middle-aged and older adults.
Methods
Study Design and Participants
This prospective cohort study used data from the China Health and Retirement Longitudinal Study (CHARLS), a nationally representative longitudinal survey of community-dwelled Chinese people aged 45 years or older. The CHARLS recruited participants from 150 counties or districts and 450 villages or urban communities across 28 provinces of China, using the multistage stratified probability-proportionate-to-size sampling. 21
Wu utilized data from 5 CHARLS waves (2011-2020), with baseline data collected in 2011 and follow-ups in 2013, 2015, 2018, and 2020 (see Supplementary Figure 1 for inclusion flowchart). After excluding participants aged <45 years, those with non-2011 baseline data, individuals lacking ≥1 follow-up, and cases with incomplete key variables, 12 643 eligible subjects were included. For each participant, all study variables were repeatedly measured at every available survey wave from 2011 to 2020. The study protocol was approved by the institutional ethics review committee (grant number: IRB00001052-11015), and informed consent was obtained from study participants.
Measurements
Physical-Psychological-Cognitive Multimorbidity
The independent variable of interest was PPC-multimorbidity, which was measured in accordance with previous studies.10,12 Specifically, physical disorder was ascertained if the participants self-reported doctoral diagnosis of at least one of the following 7 physical chronic diseases: hypertension, diabetes, stroke, heart disease, arthritis, lung disease, and cancer. Psychological disorder was evaluated using the 10-item Center for Epidemiological Studies Depression Scale (CESD-10), assessing key symptoms of depression. The total CES-D score ranged between 0 and 30, and participants were defined as having depressive symptoms when their score was equal to or above the cutoff value of 10. Cognitive disorder was assessed using the Telephone Interview for Cognitive Status (TICS), measuring episodic memory and mental intactness. The total TICS score ranged from 0 to 30, and participants were defined as having cognitive disorder if their score was 11 or fewer.
We considered 3 formats of the PPC-multimorbidity variable, to account for the complexity and variations in influences from PPC-multimorbidity. First, according to the presence of PPC-multimorbidity, individuals with all 3 types of disorders (PPC) were defined as “PPC-multimorbidity,” otherwise “non PPC-multimorbidity.” Second, according to the number of disease types in an individual, PPC-multimorbidity was categorized into “no disorder,” “one-type disorder alone,” “two-type disorders,” and “three-type disorders.” Third, according to the distinct disease patterns, 8 categories were constructed to measure PPC-multimorbidity: “physical disorder only,” “psychological disorder only,” “cognitive disorder only,” “physical-psychological multimorbidity,” “physical-cognitive multimorbidity,” “psychological-cognitive multimorbidity,” “physical-psychological-cognitive multimorbidity,” and “no above-mentioned disorders.”
Health Care Utilization and Costs
Following previous literature,16-18 the outcomes were indicators of health care utilization and costs for both outpatient and inpatient services. Health care utilization was assessed based on self-reported any visit and number of visits to outpatient clinics in last month and inpatient clinics over last year. For inpatient use, data on their length of stay in hospital during their most recent hospitalization in last year were additionally collected. Because our economic analysis specifically focuses on individual and household financial burdens, health care costs were ascertained according to self-reported total OOP spending (after deducting the reimbursed expenses, in Chinese Yuan [CNY]) for their outpatient visits during the past month and inpatient stays during the past year. To enhance international interpretability, all CNY estimates for health care costs were also converted to US dollars (USD) using the 2023 purchasing power parity conversion factor for China (1 USD = 6.92 CNY) published by the World Bank. The converted USD amounts are presented alongside the primary CNY results in the text and relevant tables.
Covariates
We considered the following covariates: age (45-59, and ≥60 years old), sex (male vs female), marital status (married vs others), education (illiterate, primary school, middle school, and above), residence (rural vs urban), health insurance (no insurance, Urban Employee Basic Medical Insurance, Urban Resident Basic Medical Insurance, New Rural Cooperative Medical Scheme, and other insurances), alcohol consumption (never, <once/week, and ≥once/week), smoking status (never, past, and current), and annual household income (categorized into 4 quartiles).
Statistical Analysis
Descriptive characteristics were summarized using numbers and percentages for categorical variables, or means and standard deviations for continuous variables. Chi-square tests or Kruskal-Wallis tests were used when appropriate to compare sociodemographics and health care use/costs across levels of PPC-multimorbidity.
A panel data approach of mixed-effects regression models was performed to examine the associations of PPC-multimorbidity (3 formats of measurements, respectively) with health care use and costs outcomes. As an observational cohort study, our statistical models described below focus on exploring longitudinal associations, and the findings should be interpreted accordingly without implying direct causality. Mixed-effects models are applicable to analysis for longitudinal data with repeated measurements, as they can account for correlations across repeated observations within each subject to obtain robust risk estimates.22,23 To be specific, mixed-effects logistic models were conducted for binary outcomes (any outpatient/inpatient visit), with results reported as odds ratio (OR) and 95% confidence interval (CI). Mixed-effects negative binomial regression models were employed for outcomes (number of outpatient/inpatient visits and hospitalization days), with results reported as incidence rate ratio (IRR) with 95% CI. Mixed-effects Tobit regression models were employed for health care expense outcomes including outpatient OOP cost and inpatient OOP cost, with results presented as coefficients (β) with 95% CI. 24 The above models were conducted in 2 ways: one crude model without adjustment for any covariates and a full model adjusting for predefined covariates. In addition, we performed trend tests when examining PPC-multimorbidity according to the number of disease types, to confirm whether there was a constant trend toward higher health care risks along with increasing number of disorder types. We also assessed potential interactions among the components of PPC-multimorbidity on both additive and multiplicative scales. Additive interactions were quantified by calculating the relative excess risk due to interaction (RERI), the attributable proportion due to interaction (AP), and the synergy index (SI), with 95% CIs estimated via the delta method. Multiplicative interactions were evaluated by incorporating product terms of the respective disorders into the models. All data analyses were carried out with Stata version 17.0 (Stata Corp LP, College Stata, Texas), and a 2-sided P< .05 was considered statistically significant.
Results
This study analyzed 12 643 participants (mean baseline age 58.51 ± 8.98; 55.03% female), with baseline characteristics detailed in Supplementary Table 1. Among them, 12.67% were affected by PPC-multimorbidity, 16.55% of physical-psychological multimorbidity, 3.16% of physical-cognitive multimorbidity, 10.34% of psychological-cognitive multimorbidity, 28.22% of physical disorder only, 4.76% of psychological disorder only, 6.08% of cognitive disorder only, and 18.22% without any defined disorders. Participants who were female, in older age group, other than married, with lower educational attainment, rural residents, had no insurance or insurance type for urban and rural residents, never smoked cigarettes or drunk alcohol, and had more disadvantaged household income were generally more likely to encounter multimorbidity of PPC conditions simultaneously (all P < .001).
Supplementary Figures 2 and 3 depict the descriptive summary of health care use and costs according to PPC-multimorbidity status and survey waves. In each wave, the outcomes relating to health care utilization and costs varied significantly by levels of PPC-multimorbidity (all P < .05). The individuals were consistently found to have higher outpatient/inpatient utilization (any visit/number of visits) and higher health care costs, along with the increasing number of disease types that they exhibited.
Table 1 reveals that middle-aged and older adults with concurrent PPC disorders (PPC-multimorbidity) had substantially elevated health care utilization and costs compared with those without all 3 disease types. In fully adjusted models controlling for potential confounders, the PPC-multimorbidity group showed significantly increased outcomes (any outpatient visit: OR = 1.43, 95% CI 1.32-1.56; number of outpatient visits: IRR = 1.41, 95% CI 1.30-1.52; any inpatient visit: OR = 1.73, 95% CI 1.57-1.90; number of inpatient visits: IRR = 1.53, 95% CI 1.42-1.65; inpatient hospital days: IRR = 1.71, 95% CI 1.49-1.97; outpatient costs: β = 24.96 [≈3.61 USD], 95% CI 17.61-32.31; inpatient costs: β = 353.02 [≈51.01 USD], 95% CI 277.80-428.23; all P < .001). Results from crude models were similar as above (all OR/IRR>1 or β > 0, P < .001).
Longitudinal Associations of Physical-Psychological-Cognitive Multimorbidity (According to Presence of PPC-Multimorbidity) With Health Care Use and Costs.
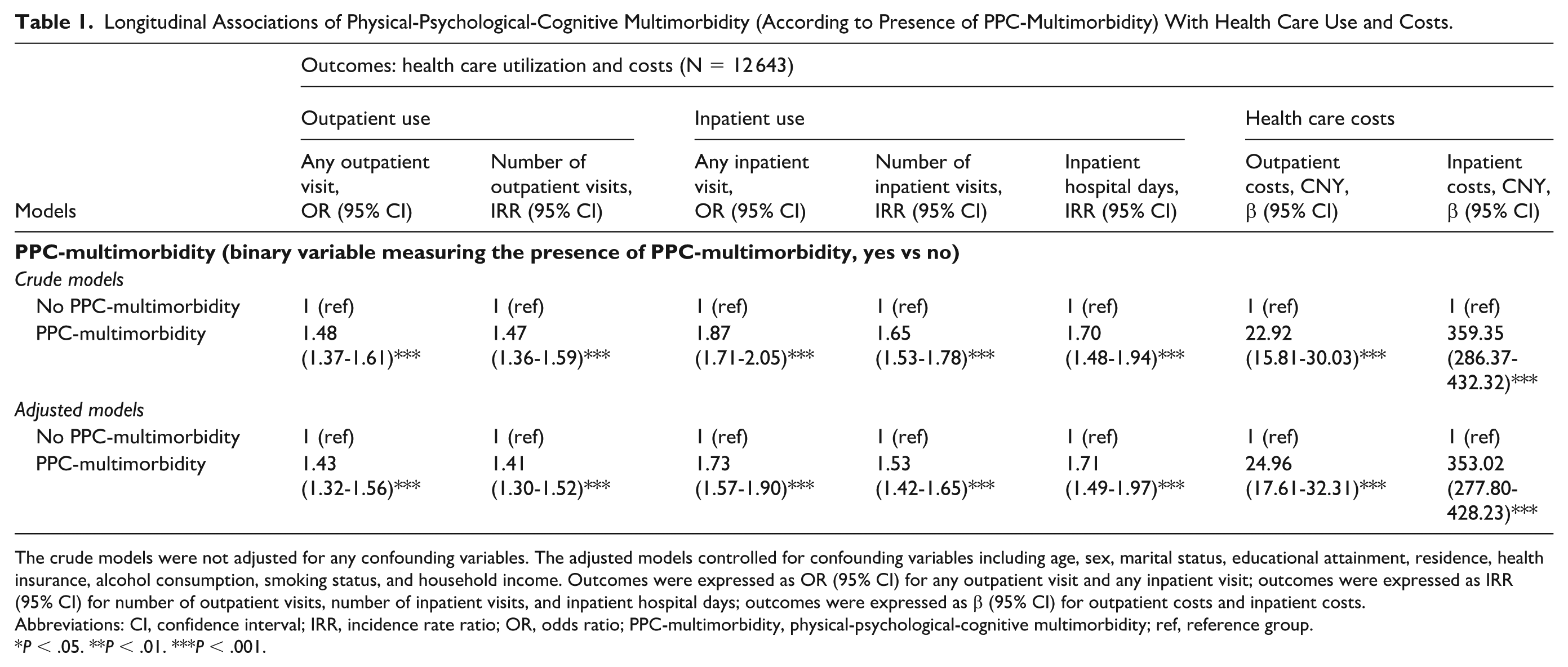
The crude models were not adjusted for any confounding variables. The adjusted models controlled for confounding variables including age, sex, marital status, educational attainment, residence, health insurance, alcohol consumption, smoking status, and household income. Outcomes were expressed as OR (95% CI) for any outpatient visit and any inpatient visit; outcomes were expressed as IRR (95% CI) for number of outpatient visits, number of inpatient visits, and inpatient hospital days; outcomes were expressed as β (95% CI) for outpatient costs and inpatient costs.
Abbreviations: CI, confidence interval; IRR, incidence rate ratio; OR, odds ratio; PPC-multimorbidity, physical-psychological-cognitive multimorbidity; ref, reference group.
P < .05. **P < .01. ***P < .001.
Table 2 reveals that individuals with increasing PPC-multimorbidity types (1/2/3 disorders) consistently showed higher health care utilization/costs versus disorder-free controls across models (all OR/IRR>1 or β > 0, P < .001). Notably, 3-type disorders resulted in the highest risks of inpatient/ outpatient use and costs than either 1- or 2-type disorders (in adjusted models, eg, any outpatient visit: ORs for 3-type disorders = 3.03 vs ORs for 1- or 2-type disorders = 1.73-2.54; number of outpatient visits: OR = 2.94 vs 1.68-2.49; any inpatient visit: OR = 4.43 vs 1.97-3.22; number of inpatient visits: IRR = 3.82 vs 1.94-2.98; inpatient hospital days: IRR = 3.58 vs 1.72-2.63; outpatient costs: β = 53.32 [≈7.71 USD] vs 16.93-39.69 [≈2.45-5.74 USD]; inpatient costs: β = 628.67[≈90.85 USD] vs 169.22~383.69 [≈24.45-55.45 USD]). Results from trend analyses indicated progressively increasing health care risks in terms of all studied endpoints, along with a rising number of coexisting disorder types (all P for trend < .001).
Longitudinal Associations of Physical-Psychological-Cognitive Multimorbidity (According to Number of Disease Types) With Health Care Use and Costs.
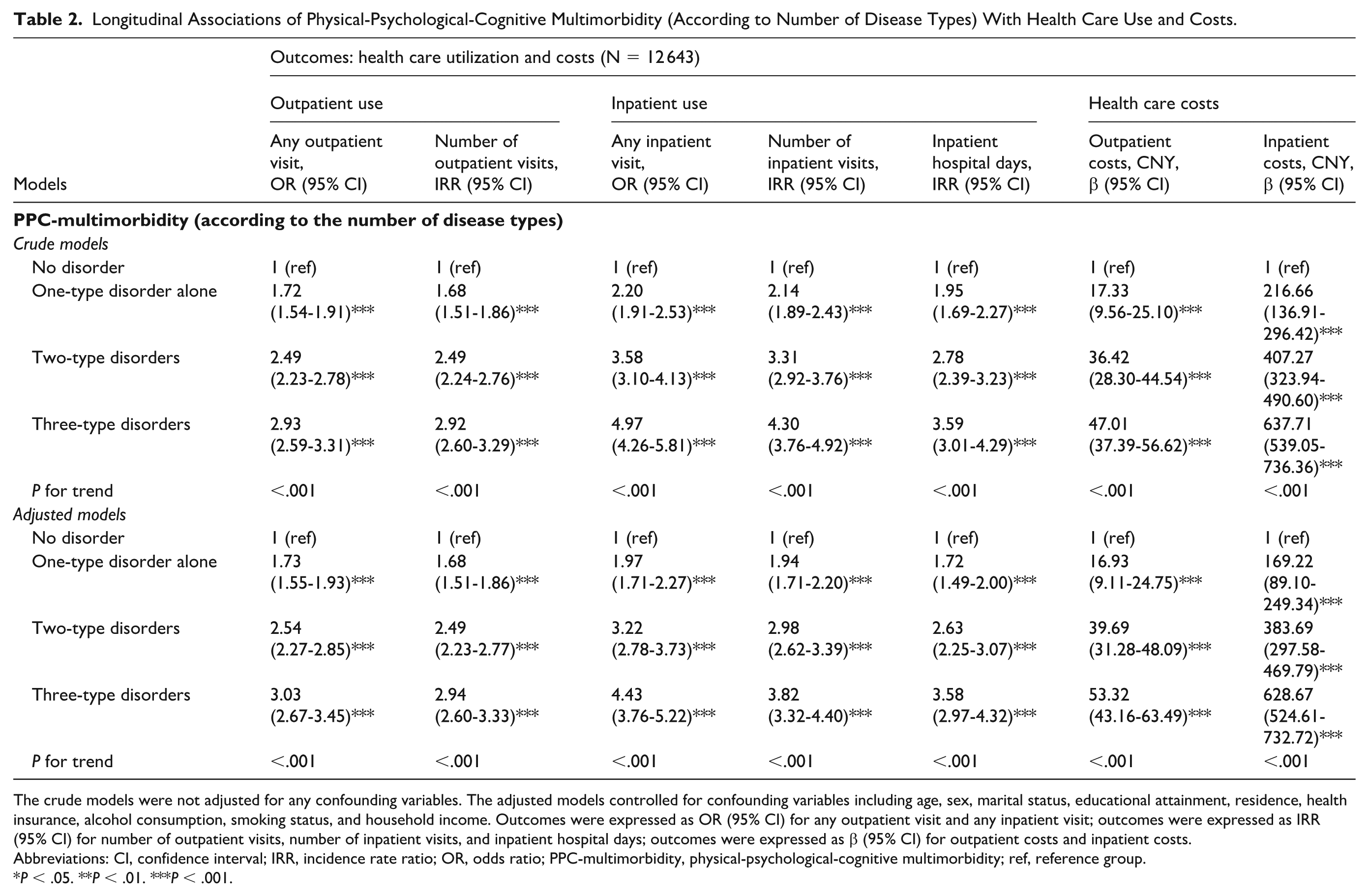
The crude models were not adjusted for any confounding variables. The adjusted models controlled for confounding variables including age, sex, marital status, educational attainment, residence, health insurance, alcohol consumption, smoking status, and household income. Outcomes were expressed as OR (95% CI) for any outpatient visit and any inpatient visit; outcomes were expressed as IRR (95% CI) for number of outpatient visits, number of inpatient visits, and inpatient hospital days; outcomes were expressed as β (95% CI) for outpatient costs and inpatient costs.
Abbreviations: CI, confidence interval; IRR, incidence rate ratio; OR, odds ratio; PPC-multimorbidity, physical-psychological-cognitive multimorbidity; ref, reference group.
P < .05. **P < .01. ***P < .001.
Table 3 demonstrates that all PPC-multimorbidity groups (excluding cognitive disorder-only) showed significantly higher health care utilization and costs versus disease-free controls (all OR/IRR > 1 or β > 0, P < .05). Individuals suffering from 3 disease types simultaneously or physical-psychological multimorbidity appeared to exhibit the highest health care use and costs (any outpatient visit: ORs for these 2 categories = 2.86-3.19 vs ORs for other categories = 0.92-1.90; number of outpatient visits: IRRs = 2.79-3.06 vs 0.92-1.85; any inpatient visit: ORs = 3.71-4.28 vs 0.82-2.85; number of inpatient visits: IRRs = 3.37-3.74 vs 0.92-2.67; inpatient hospital days: IRRs = 2.91-3.36 vs 0.81-2.23; outpatient costs: βs = 49.77-56.02 [≈7.19-8.10 USD] vs −4.92 to 21.41 [≈–0.71 to 3.09 USD]; inpatient costs: βs = 454.30-615.20 [≈65.65-88.90 USD) vs 28.76-320.53 [≈4.16-46.32 USD]). Notably, individuals with PPC-multimorbidity often showed the highest risk for inpatient-related outcomes (PPC-multimorbidity group vs physical-psychological multimorbidity group: OR for any inpatient visit, 4.28 vs 3.71; IRR for number of inpatient visits, 3.74 vs 3.37; IRR for inpatient hospital days, 3.36 vs 2.91; β for inpatient costs, 615.20 [≈88.90 USD] vs 454.30 [≈65.65 USD]), while those with physical-psychological multimorbidity generally had the greatest risk for outpatient-related outcomes (physical-psychological multimorbidity group vs PPC-multimorbidity group: OR for any outpatient visit, 3.19 vs 2.86; IRR for number of outpatient visits, 3.06 vs 2.79; β for outpatient costs, 56.02 [≈8.10 USD] vs 49.77 [≈7.19 USD]). The above results remained consistent in crude models. Further interaction analyses (Supplementary Table 2) revealed that physical-psychological multimorbidity exhibited significant positive additive interactions across most outcomes (all RERI > 0, AP > 0, SI > 1, P < .05), with the exception of inpatient hospital days. Physical-cognitive multimorbidity demonstrated significant positive additive interactions exclusively for inpatient-related outcomes, but not for outpatient services. In contrast, psychological-cognitive and 3-domain multimorbidities generally lacked significant additive interactions. Notably, the absence of significant multiplicative interactions for most outcomes suggests that health care utilization does not compound exponentially beyond the product of individual disease risks.
Longitudinal Associations of Physical-Psychological-Cognitive Multimorbidity (According to Disease Patterns) With Health Care Use and Costs.
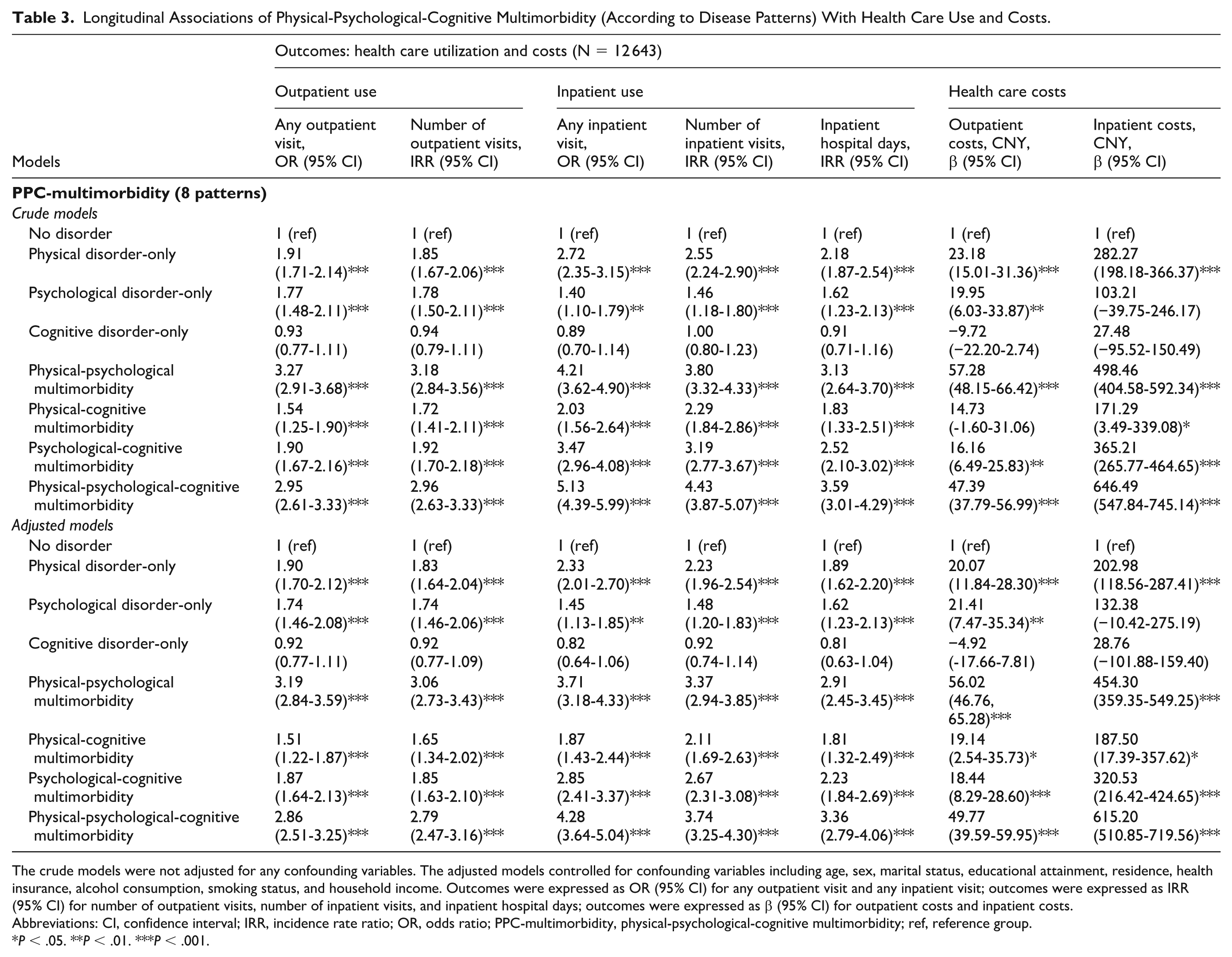
The crude models were not adjusted for any confounding variables. The adjusted models controlled for confounding variables including age, sex, marital status, educational attainment, residence, health insurance, alcohol consumption, smoking status, and household income. Outcomes were expressed as OR (95% CI) for any outpatient visit and any inpatient visit; outcomes were expressed as IRR (95% CI) for number of outpatient visits, number of inpatient visits, and inpatient hospital days; outcomes were expressed as β (95% CI) for outpatient costs and inpatient costs.
Abbreviations: CI, confidence interval; IRR, incidence rate ratio; OR, odds ratio; PPC-multimorbidity, physical-psychological-cognitive multimorbidity; ref, reference group.
P < .05. **P < .01. ***P < .001.
Discussion
Our study analyzed PPC disorders, and their multimorbidity based on 12 643 community-dwelling participants aged ≥45 years across China. Moving beyond a conventional disease-counting approach to define multimorbidity, we identified 3 multimorbidity patterns: 39.06% single disorder, 30.05% 2-type multimorbidity, and 12.67% concurrent PPC impairments. This PPC-multimorbidity framework better reflects real-world clinical complexity, as relying solely on a physical-disease lens underestimates the impact of mental and cognitive issues on treatment adherence and health care-seeking behaviors. Multimorbidity is similarly highly prevalent, partly because these diseases frequently co-occur due to shared risk factors and underlying pathological mechanisms. Prior studies focused on physical multimorbidity (relaxed criteria, no cross-domain requirement), complicating comparability. To our knowledge, few studies have reported pattern-specific multimorbidity data comparable with ours. One multi-region study 10 estimated multimorbidity prevalence (≥2 disorder types) at 24.5% for high-income countries, 33.9% for upper-middle-income countries, and 8.1% for lower-middle-income country, which were lower than our estimate at 42.72%. Another study 11 from Henan Province of China reported a prevalence of 16.74% for co-occurring PPC-multimorbidity among older hypertensive population, exceeding our estimate of 12.67%. Discrepancies stemmed from population characteristics, disease definitions, health care systems, and diagnostic criteria. We recommend harmonizing definitions and multidisciplinary screening protocols for cross-regional comparability.
We found that individuals with 3-type multimorbidity across PPC domains exhibited the highest health care use and costs, followed by those with 2-type and single-type conditions. This finding aligns with previous research17,18,25 showing that multimorbidity (co-presence of 2 or more chronic diseases), in general, is associated with increased outpatient and inpatient visits, longer hospitalization stays, and greater medical expenditures, although prior studies relied on simple disease counts and focused mainly on physical comorbidities like diabetes-hypertension dyads. Driven by demographic shifts toward an aging population, modern epidemiological concepts and the advent of molecular medicine underscore the necessity of diagnosing and managing the co-occurrence of multiple-type diseases. This study offers a novel perspective by delineating health care burden attributable specifically to the simultaneous occurrence of PPC disorders and the number of coexisting disease types.
Our study reveals distinct impacts of PPC-multimorbidity patterns on health care outcomes. Compared with disease-free individuals, all patterns except isolated cognitive impairment significantly increased health care utilization and costs. Such results partially coincide with previous findings that have supported higher health care utilization and costs associated with single-domain multimorbidity (eg, single mental multimorbidity 26 ), 2-domain multimorbidity (eg, physical multimorbidity together with depression, 24 physical-psychological multimorbidity, 27 schizophrenia and cognitive multimorbidity 28 ), and multimorbidity without domain specification (eg, the presence of at least 2 concurrent conditions spanning physical, psychiatric, and memory-related disorders, regardless of disorder type 6 ). In contrast, our results suggested that cognitive disorders alone might not be as impactful on health care utilization and costs as when they coexisted with physical or psychological conditions. This finding is somewhat inconsistent with previous literature emphasizing the significant health care burden associated with cognitive disorders. 29 Several reasons may explain this discrepancy: (1) untreated mild cognitive impairments (stigma/aging attribution/limited specialist access); (2) cultural family caregiving delaying formal care; and (3) under-resourced cognitive services causing under-recognition. The coexistence of different disease types may amplify or alter health care needs through complex interactions.
We found that physical-psychological multimorbidity most significantly increased outpatient service demands, while PPC-multimorbidity predominantly elevated hospitalization risks, a pattern not previously documented with unclear mechanisms. This discrepancy may stem from distinct disease interaction mechanisms and systemic health care gaps. Because NCDs largely dictate the location of treatment—such as outpatient versus inpatient care—and the concurrent hospital costs incurred, their longitudinal progression must be carefully monitored. Physical-psychological multimorbidity raises outpatient burdens through psychological distress somatization (eg, anxiety-induced physical symptoms), complex medication adjustments (eg, antidepressant-antihypertensive interactions), reduced treatment adherence, and fragmented multispecialty care-seeking. Conversely, PPC drives hospitalizations via cognitive impairment-mediated cascades, including diminished self-management capacity (eg, medication nonadherence worsening chronic conditions), heightened acute complication risks (eg, delirium-induced falls/infections), and caregiver reliance on crisis-driven inpatient care rather than routine outpatient management. Notably, PPC’s lower outpatient utilization may reflect systemic diagnostic overshadowing (cognitive deficits masking treatable physical/mental symptoms) and structural barriers (eg, inadequate cognitive assessment resources in clinics), redirecting unmet needs toward reactive hospitalizations.
To further elucidate these patterns, our formal interaction analyses revealed that the combined impact of multimorbidity on health care utilization is primarily additive rather than multiplicative. The general absence of multiplicative interactions suggests that health care utilization does not compound exponentially beyond the product of individual disease risks. However, on an additive scale, physical-psychological multimorbidity exhibited significant positive synergism across most outcomes, indicating that this specific co-occurrence drives absolute health care demands significantly greater than the sum of their individual effects. This additive synergism likely reflects the profound bidirectional interference between somatic symptoms and psychological distress, which complicates routine management and inflates overall care needs. Furthermore, physical-cognitive multimorbidity demonstrated additive synergism exclusively for inpatient-related outcomes. This highlights how cognitive impairments may not necessarily drive routine outpatient visits but can severely compromise the self-management of physical conditions, ultimately precipitating acute health crises and reactive hospitalizations. In contrast, the lack of significant interactions in other combinations suggests their burdens are largely independent and cumulative.
Our observed relationships revealed cumulative PPC-multimorbidity burden on health care systems, which can be explained through both behavioral and biological pathways. Behaviorally, unhealthy lifestyles and socioeconomic disadvantages (eg, low social participation, limited support) fuel a vicious cycle: physical illness exacerbates psychological and cognitive decline, while mental and cognitive impairments hinder self-care and treatment adherence. These health, behavioral, and social parameters act as risk factors moderating the transition from isolated physical conditions to complex PPC-multimorbidity, thus invoking an increased health burden. Biologically, these specific multimorbidity patterns may be rooted in accelerated aging processes, such as chronic low-grade inflammation (“inflammaging”), cellular senescence, and oxidative stress. These pathophysiological changes related to aging should be continuously monitored and compared across different ages. These mechanisms share complex, bidirectional links with depressive symptoms and cognitive decline, ultimately compromising neurovascular and immune integrity. 30 Although these mechanistic inferences could not be directly tested due to the lack of biomarker data, it is evident that the co-occurrence of multiple disease types amplifies biological dysregulation and functional decline. Consequently, this complexity exacerbates symptoms and complicates clinical management, escalating health care demands and economic burdens in a primarily cumulative and additively synergistic manner. Although delaying disease onset using molecular techniques and modern medical therapies is not yet fully realized for clinical use, it holds significant promise for delaying the onset of multimorbidity and aging as a whole.
Our findings suggest that while simple comorbidity counts serve as robust predictors of health care utilization, recognizing specific disease interaction patterns—particularly the additive synergism of physical-psychological multimorbidity—provides critical complementary value. A more nuanced approach to managing multimorbidity is necessary, complementing a generalized focus on the number of chronic conditions with an understanding of specific disease combinations. Policymakers should prioritize integrated multidisciplinary care for PPC interactions in community-dwelling adults, strengthening primary care for early detection/care coordination, mitigating cognitive disorder stigma, and improving specialist access. As understanding of molecular mechanisms deepens, future precision interventions targeting pathways like inflammation may hold potential for delaying multimorbidity progression, a direction for future research. While our micro-level study design limited direct linkage to aggregate population indicators, it provides essential clues for broader assessments. Future research must standardize definitions/methodologies, investigate mechanisms linking multimorbidity patterns to outcomes, and develop targeted interventions for unique profiles-addressing the multifaceted nature of PPC-multimorbidity to align with health care system demands. Crucially, to fully capture the longitudinal dynamics of multimorbidity and its macro-level impact, future studies should employ multi-source data fusion, correlating these clinical findings with morbidity and mortality statistics, timely population censuses, and national insurance and retirement data.
Our study is subject to several limitations. First, reliance on self-reported data may introduce recall bias and fail to capture undiagnosed conditions. Although the measures used in CHARLS have been validated in previous literature,10,12,16-18 potential variations in recall accuracy and diagnostic sensitivity across survey waves may still affect our estimates. Second, although we adjusted for key behavioral and socioeconomic covariates, we did not formally examine their mediating pathways between PPC-comorbidity and medical outcomes. We cannot completely rule out residual confounding or potential reverse causality. Third, the limited range of chronic conditions assessed may underestimate multimorbidity prevalence and its health care burden. Fourth, our economic evaluation focused exclusively on OOP spending rather than comprehensive health system or broader societal costs. Fifth, the absence of biomarker data precluded the direct testing of the underlying biological mechanisms discussed. Future research should integrate multi-source data, utilize objective clinical indicators, encompass a broader spectrum of diseases, and incorporate biomarker data to better elucidate causal mechanisms and refine health care burden assessments. Exploring targeted interventions through precision and molecular medicine will also be a crucial next step.
Conclusions
This study highlights the substantial health care burden associated with PPC-multimorbidity among middle-aged and older adults in China. People with all 3 disorder types exhibit higher health care utilization and costs. More coexisting disease types are associated with a heavier health care burden. Notably, most PPC-multimorbidity patterns (except cognitive disorders alone) are consistently associated with elevated health care risks. Moving beyond simple disease counts, our longitudinal findings suggest that specific disease combinations—particularly the co-occurrence of physical and psychological conditions—are associated with distinct health care utilization patterns and costs. These results underscore the value of investigating specific multimorbidity patterns across PPC domains. Understanding these complex interactions may provide useful insights for transitioning from traditional, single-disease management toward targeted, multidisciplinary care approaches, ultimately optimizing resource allocation and improving health outcomes for aging populations.
Supplemental Material
sj-docx-1-aph-10.1177_10105395261458501 – Supplemental material for Longitudinal Association of Physical-Psychological-Cognitive Multimorbidity With Health Care Utilization and Costs Among Middle-Aged and Older People in China
Supplemental material, sj-docx-1-aph-10.1177_10105395261458501 for Longitudinal Association of Physical-Psychological-Cognitive Multimorbidity With Health Care Utilization and Costs Among Middle-Aged and Older People in China by Xiaohan Qu, Qian Wang, Hui Xue, Meng Li, Wei Du, Aihua Shen and Lijun Fan in Asia Pacific Journal of Public Health
Footnotes
Acknowledgements
The authors sincerely acknowledge the CHARLS team for collecting and publicizing the research data, and also thank all the participants and investigators involved in CHARLS survey.
Ethical Considerations
This study involves human participants and was approved by Biomedical Ethics Review Committee of Peking University (IRB00001052-11015). Participants gave informed consent to participate in the study.
Author Contributions
Xiaohan Qu: Writing – review & editing, Writing – original draft, Methodology, Data curation. Qian Wang: Writing – review & editing, Validation, Methodology. Hui Xue: Writing – review & editing, Validation, Methodology. Meng Li: Writing – review & editing, Validation, Methodology, Supervision. Wei Du: Writing – review & editing, Validation, Methodology, Supervision. Aihua Shen: Writing – review & editing, Validation, Supervision. Lijun Fan: Writing – review & editing, Validation, Supervision, Project administration, Conceptualization.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Social Science Foundation of China (grant number: 23CGL072). The funder had no role in study design, data collection, data analysis, data interpretation, or writing of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.