
Abstract
Purpose
To investigate the level of miR-550a-3p in patients with osteoporosis (OP), osteoporotic fractures (OPF), and healthy controls, and diagnostic value for OP, OPF, and fracture healing.
Methods
246 OP patients (120 OP, 126 OPF) and 113 healthy controls were enrolled. Serum miR-550a-3p levels were detected by reverse transcription-quantitative polymerase chain reaction (RT-qPCR). Pearson analysis assessed correlations with T-score, 25-(OH) Vitamin D, receptor activator of nuclear factor-κB ligand (RANKL), and osteoprotegerin (OPG). OPF patients were followed for 6 months (normal/delayed healing groups). Receiver operating characteristic (ROC) curves and logistic regression analyzed diagnostic value.
Results
miR-550a-3p expression was significantly lower in OP and OPF groups than in controls, with the lowest level in OPF patients. It effectively distinguished OP from controls (AUC = 0.899) and OPF from OP (AUC = 0.911). miR-550a-3p was positively correlated with T-score, 25-(OH) Vitamin D, and OPG, and negatively correlated with RANKL. In OPF patients, miR-550a-3p was lower in the delayed healing (DH) group (AUC = 0.851) and identified as an independent factor for delayed healing.
Conclusion
miR-550a-3p exhibits potential as a biomarker for diagnosing OP and OPF, and for predicting fracture healing outcomes in OPF patients, providing a novel tool for clinical management of osteoporotic fractures.
Introduction
Osteoporosis (OP) is a systemic metabolic bone disease characterized by low bone mass and deterioration of bone microstructure, with its core hazard being increased bone fragility and susceptibility to fractures. 1 The incidence of osteoporosis is increasing year by year with the aging of the population, and it is particularly common in postmenopausal women, having become one of the major global public health problems. 2 Osteoporotic fracture (OPF), as the most serious complication of this disease, occurs mostly in the hip, spine, and wrist. 3 It not only leads to impaired limb function and a significant decline in patients’ quality of life but also substantially increases the medical burden on families and society. 4 However, in clinical practice, some patients with osteoporotic fractures may experience poor healing phenomena such as delayed fracture healing or nonunion. 5 Poor fracture healing will further prolong the treatment cycle and increase the disability and mortality rates.6,7 Therefore, exploring the key regulatory factors affecting OPF healing and potential diagnostic biomarkers—including biomarkers for OP diagnosis and predictors for fracture normal healing/delayed healing—is of great clinical significance for optimizing the diagnosis and treatment strategies of osteoporotic fractures.
MicroRNA (miRNA), as a class of endogenous non-coding RNA, plays a key role in physiological and pathological processes such as bone metabolism, osteoblast differentiation, osteoclast activity, and fracture healing by targeting and regulating the expression of target genes. 8 For example: overexpression of miR-1224-5p can slow down RANKL-induced osteoclast differentiation, and promote osteoblast differentiation; at the same time, it can significantly promote fracture healing and alleviate the progression of osteoporosis caused by estrogen deficiency or aging. 9 Downregulation of miR-30b-5p can enhance the expression of osteogenesis-related markers (ALP, OCN, RUNX2) and promote calcium deposition, thereby regulating the osteogenic differentiation of human Bone Marrow Mesenchymal Stem Cells (hBMSCs). 10 Overexpression of miR-34c can significantly promote osteoclast differentiation and regulate the NF-κB and glycogen synthase kinase 3-β signaling pathways during osteoclast differentiation. 11 In addition, both miR-422a 12 and miR-194-5p 13 show differential expression in postmenopausal women with osteoporosis and can serve as potential miRNA biomarkers for postmenopausal osteoporosis. Notably, as a miRNA with potential regulatory functions, miR-550a-3p has been confirmed in studies to be positively correlated with mineral apposition rate (MAR) and trabecular bone volume fraction (BV/TV). 14 It is also downregulated in patients with low-trauma fractures (a typical feature of OPF), 15 suggesting that it may be involved in bone metabolism and the pathological process of OPF. Furthermore, miR-550a-3p has been found to be associated with hematopoietic function, cell migration, and apoptosis, 16 but its specific role and diagnostic value in osteoporotic fractures remain unclear.
Based on the above background, this study will detect the expression level of miR-550a-3p, analyze its correlation with clinical indicators, evaluate its value in differential diagnosis of OP versus OPF (i.e., distinguishing OPF from OP/healthy controls), and assess its predictive value for delayed healing in OPF patients. It aims to provide new molecular markers and theoretical basis for the early diagnosis and healing assessment of osteoporotic fractures.
Materials and methods
Inclusion of subjects
This study adhered to the principles of the Declaration of Helsinki, obtained approval from the Ethics Committee of Zhucheng People's Hospital, informed patients and their families of the content and purpose of the study, and obtained signed written informed consent. A total of 246 patients with osteoporosis who visited Zhucheng People's Hospital from June 2021 to November 2022 were selected, including 120 patients with osteoporosis and 126 patients with osteoporotic fractures. All included patients had a T-score of ≤ −2.5. Exclusion criteria: 1) Patients with malignant tumors, severe liver and kidney dysfunction, or autoimmune diseases; 2) Those who had received drug therapy affecting bone metabolism within the past 6 months; 3) Those with old fractures (more than 14 days); 4) Those with mental illness, cognitive impairment, or inability to cooperate with follow-up. Meanwhile, 113 healthy people were recruited as the control group.
Cell culture and transfected sample collection
Fasting venous blood (5 mL) was collected from all subjects at 8:00–10:00 AM after overnight fasting (≥8 h) enrollment. The blood samples were allowed to clot at room temperature for 30 min, then centrifuged at 3000 r/min (equivalent to ∼1500×g) for 10 min at 4°C to separate serum. The supernatant was carefully transferred to a new tube without disturbing the cell pellet, followed by a second centrifugation at 12,000 r/min (∼15,000×g) for 10 min at 4°C to remove any remaining cell debris. The clarified serum was aliquoted and stored in a −80°C ultra-low temperature refrigerator, avoiding repeated freeze-thawing, for subsequent experiments.
Follow-up
Patients with OPF were followed up for 6 months. Specific X-ray evaluation time points were scheduled at 1 month, 3 months, and 6 months post-fracture to dynamically monitor callus formation and fracture line changes. All X-ray images were independently reviewed by two radiologists with more than 5 years of experience in orthopedic imaging, who were blinded to the patients’ clinical information and miR-550a-3p expression levels. Discrepancies between the two evaluators were resolved through joint consultation with a senior orthopedic physician. Referring to the clinical definition of fracture delayed healing (i.e., no obvious callus formation or persistent fracture lines 3–6 months after fracture, without signs of nonunion) 17 if X-ray showed clear fracture lines, slow callus growth or no obvious callus formation, and local tenderness or limited activity, they were classified into the delayed healing (DH) group; otherwise, they were classified into the normal healing (NH) group.
RNA extraction and reverse transcription-quantitative polymerase chain reaction (RT-qPCR)
Total RNA was extracted from serum samples using TRIzol reagent (Invitrogen, USA) following the standard protocol described by Chomczynski and Sacchi, 18 and the purity and concentration of RNA were detected by an ultraviolet spectrophotometer (Thermo Fisher Scientific, USA). Reverse transcription was performed using the Mir Reverse Transcription Kit (Biosystems, USA). Subsequently, amplification reactions were carried out on the ABI7500 system (Applied Biosystems, USA) using the SuperReal PreMix Plus (SYBR Green) Kit (TIANGEN, China). The primer sequences used were as follows: miR-550a-3p forward: 5′-GGCTGTCTTACTCCCTCAGG-3′, reverse: 5′-CTCAACTGGTGTCGTGGAGTC-3’; U6 forward: 5′-CTCGCTTCGGCAGCACA-3′, reverse: 5′-AACGCTTCACGAATTTGCGT-3’. U6 was used as the internal reference, and the relative expression level was calculated by the 2-ΔΔCT method. 19
Statistical analysis
Statistical analysis and graphing were performed using SPSS 23.0 and GraphPad Prism 9. Measurement data were expressed as mean ± standard deviation (mean ± SD), and count data were expressed as cases and percentages. Before performing Pearson correlation analysis, the Shapiro–Wilk test was used to verify the normality of the distribution of miR-550a-3p expression levels and clinical indicators (T-score, 25-(OH) Vitamin D, RANKL, OPG). The results showed that all variables conformed to a normal distribution (p > 0.05), meeting the application conditions of Pearson correlation analysis. Pearson correlation analysis was used to explore the correlation between the expression level of miR-550a-3p and clinical indicators. Receiver operating characteristic (ROC) curve was used to analyze the diagnostic value of miR-550a-3p for OP versus Control, OP versus OPF, and NH versus DH, with the area under the curve (AUC), sensitivity, and specificity calculated. Binary logistic regression analysis was used to screen for independent factors affecting delayed healing in the OPF group. A P value < 0.05 was considered statistically significant.
Results
Basic characteristics of the subjects
The demographic and clinical data of the study population (Control group, n = 113; Osteoporosis group, n = 120; Osteoporotic fractures group, n = 126).
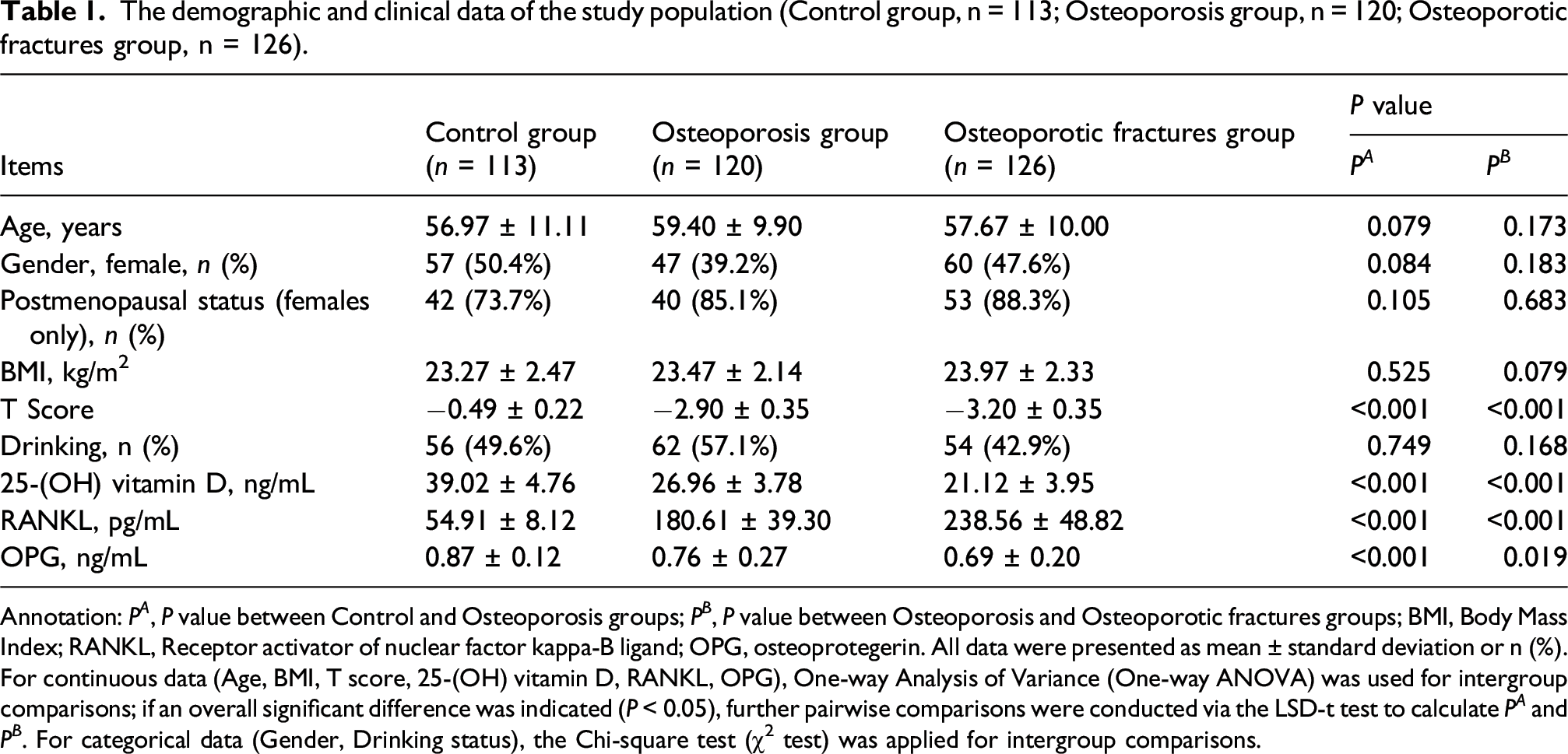
Annotation: P A , P value between Control and Osteoporosis groups; P B , P value between Osteoporosis and Osteoporotic fractures groups; BMI, Body Mass Index; RANKL, Receptor activator of nuclear factor kappa-B ligand; OPG, osteoprotegerin. All data were presented as mean ± standard deviation or n (%). For continuous data (Age, BMI, T score, 25-(OH) vitamin D, RANKL, OPG), One-way Analysis of Variance (One-way ANOVA) was used for intergroup comparisons; if an overall significant difference was indicated (P < 0.05), further pairwise comparisons were conducted via the LSD-t test to calculate P A and P B . For categorical data (Gender, Drinking status), the Chi-square test (χ2 test) was applied for intergroup comparisons.
Expression level and diagnostic role of miR-550a-3p
The results of RT-qPCR showed that compared with the healthy control, the level of miR-550a-3p was decreased in both patients with osteoporosis and patients with osteoporotic fractures, with the lowest level in patients with osteoporotic fractures (p < 0.0001, Figure 1(a)). In addition, the results of ROC curve showed that the AUC value of downregulated miR-550a-3p in distinguishing healthy people from patients with osteoporosis was 0.899, with a sensitivity of 85.00% and a specificity of 78.76% (Figure 1(b)). Meanwhile, miR-550a-3p could effectively distinguish patients with osteoporosis from patients with osteoporotic fractures, with a sensitivity of 77.78% and a specificity of 88.33% (AUC = 0.911, Figure 1(c)). Expression and diagnostic value of miR-550a-3p in patients with osteoporosis.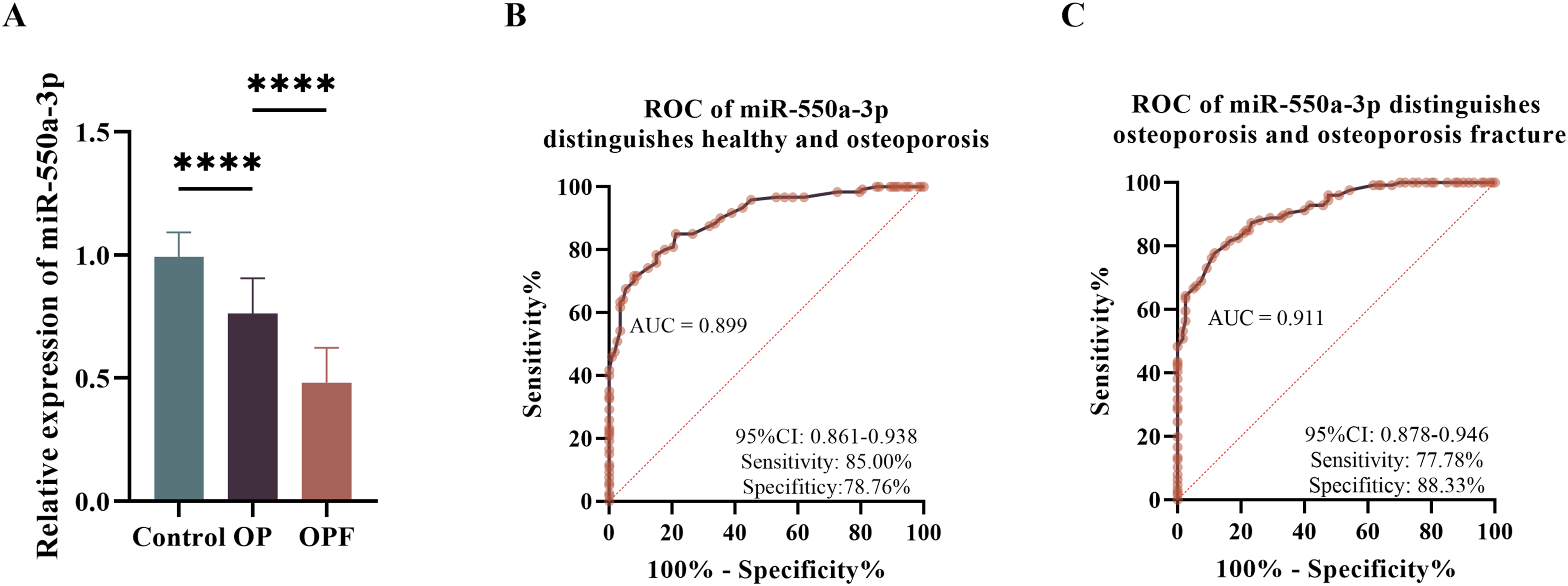
Correlation between miR-550a-3p and various indicators in OP and OPF
Pearson’s analysis of the correlation between miR-550a-3p and various indicators of OP group (n = 120) and OPF (n = 126).
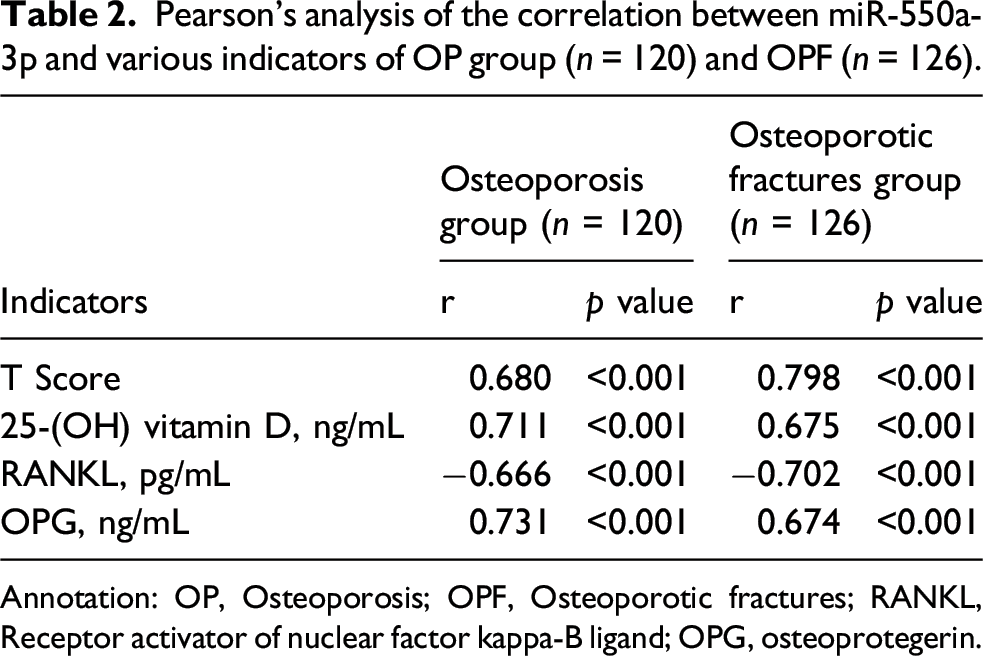
Annotation: OP, Osteoporosis; OPF, Osteoporotic fractures; RANKL, Receptor activator of nuclear factor kappa-B ligand; OPG, osteoprotegerin.
Serum miR-550a-3p level can serve as a biomarker for poor healing
Comparison of indicators in patients with normal (n = 90) versus delayed (n = 36) healing in the OPF group.
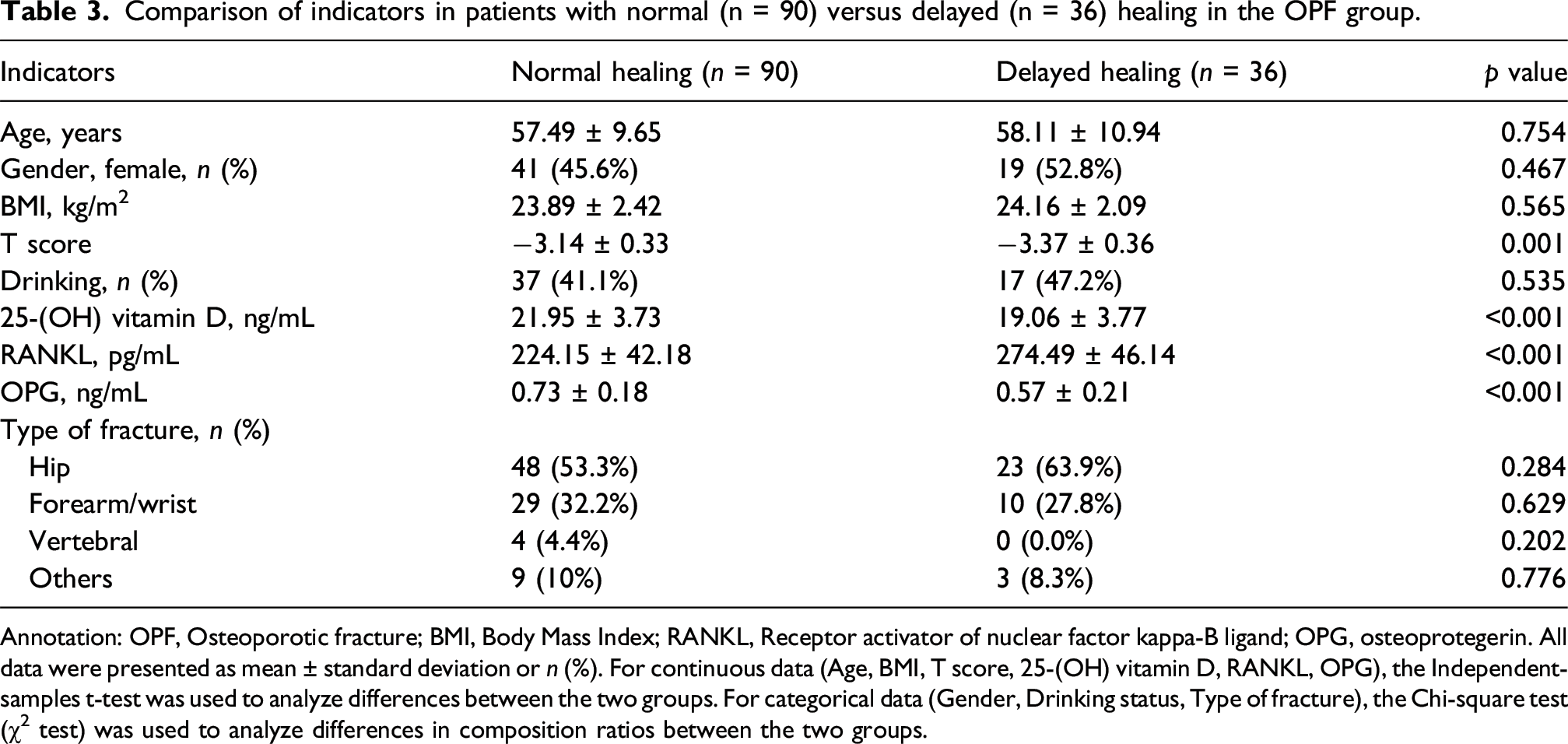
Annotation: OPF, Osteoporotic fracture; BMI, Body Mass Index; RANKL, Receptor activator of nuclear factor kappa-B ligand; OPG, osteoprotegerin. All data were presented as mean ± standard deviation or n (%). For continuous data (Age, BMI, T score, 25-(OH) vitamin D, RANKL, OPG), the Independent-samples t-test was used to analyze differences between the two groups. For categorical data (Gender, Drinking status, Type of fracture), the Chi-square test (χ2 test) was used to analyze differences in composition ratios between the two groups.
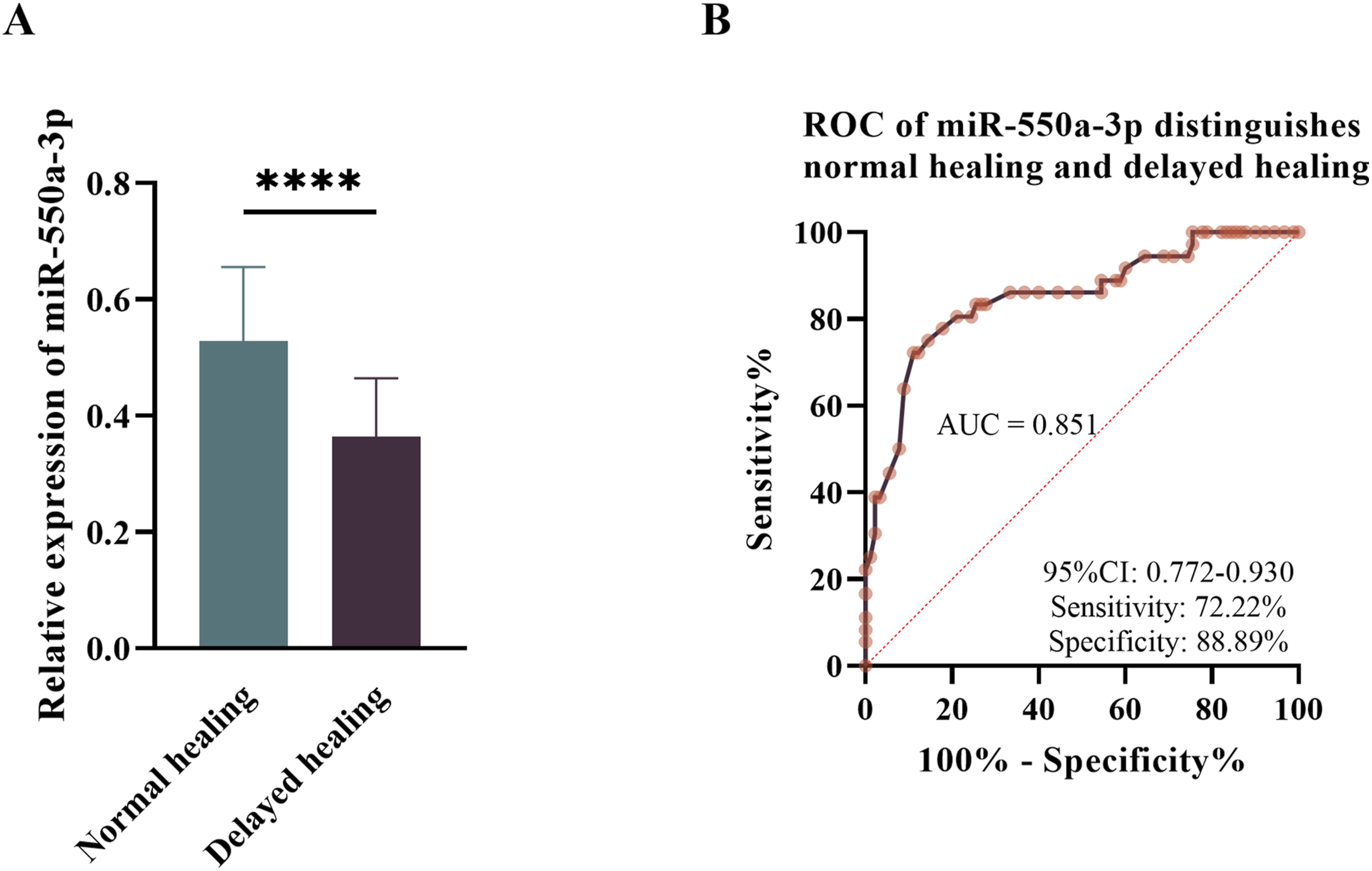
Expression and diagnostic value of miR-550a-3p in OPF patients delayed healing.
Logistic regression analyses of independent influences on delayed healing of OPF (total sample size, n = 126).
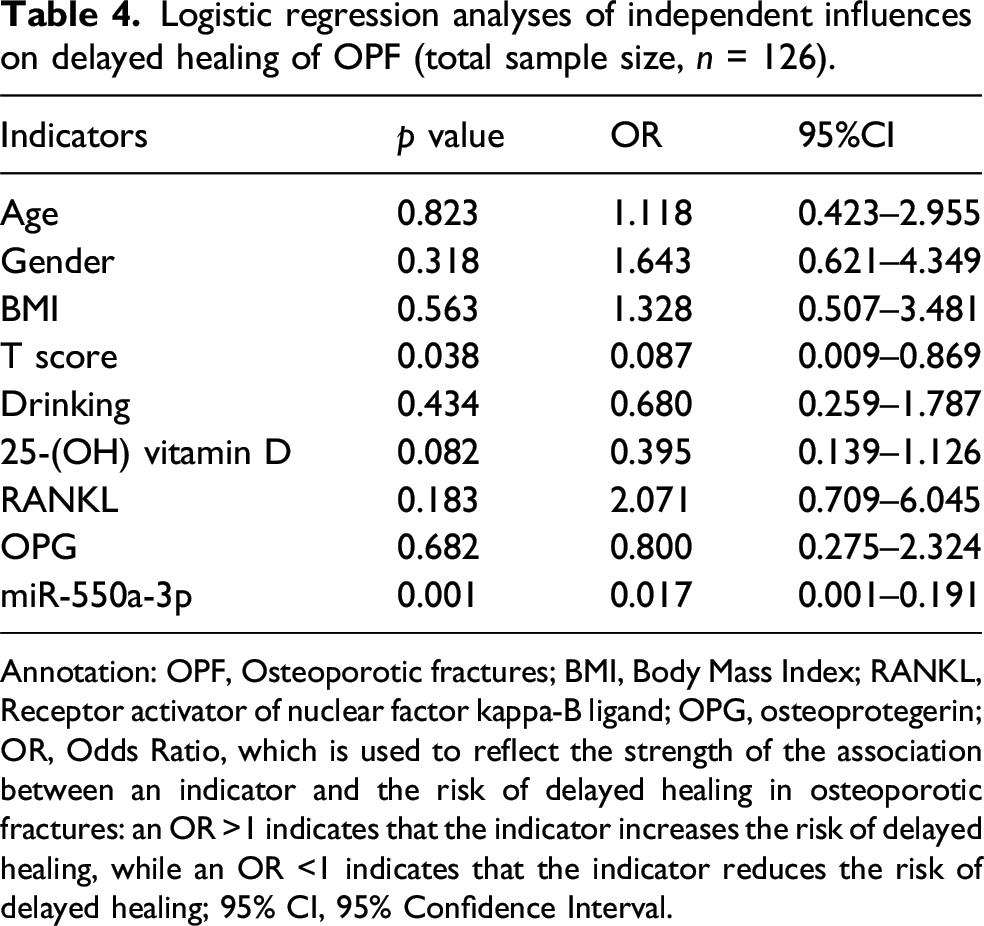
Annotation: OPF, Osteoporotic fractures; BMI, Body Mass Index; RANKL, Receptor activator of nuclear factor kappa-B ligand; OPG, osteoprotegerin; OR, Odds Ratio, which is used to reflect the strength of the association between an indicator and the risk of delayed healing in osteoporotic fractures: an OR >1 indicates that the indicator increases the risk of delayed healing, while an OR <1 indicates that the indicator reduces the risk of delayed healing; 95% CI, 95% Confidence Interval.
Discussion
Osteoporotic fractures result from bone metabolic imbalance caused by osteoporosis20,21 — when the dynamic balance between osteoblasts and osteoclasts is disrupted, bone formation decreases while bone resorption increases, leading to net bone loss, increased bone fragility, and ultimately fractures. 22 Such fractures not only cause a sharp decline in patients' quality of life but also may lead to serious complications such as pulmonary infection, significantly increasing the disability and mortality rates. 23 Meanwhile, the fracture healing process is affected by multiple factors including bone metabolic status and local microenvironment, 24 and approximately 5-10% of fracture patients will experience delayed healing or nonunion, 25 which further prolongs the treatment cycle and increases the social medical burden. 26 Currently, clinical practice mainly relies on bone mineral density detection and X-ray imaging for disease assessment, 27 but bone mineral density detection has limited sensitivity in predicting early fracture risk, and imaging examinations are difficult to accurately judge the prognosis in the early stage of fracture healing. Therefore, identifying biomarkers that can accurately reflect disease progression and predict healing outcomes is of great clinical significance for optimizing the diagnosis and treatment strategies of osteoporotic fractures.
As a miRNA with regulatory functions, miR-550a-3p has been confirmed to be involved in the development of many diseases. For example: miR-550a-3p can serve as a prognostic biomarker for diffuse malignant peritoneal mesothelioma. 28 It also shows abnormal expression in non-small cell lung cancer 29 and breast cancer. 30 Previously, miR-550a-3p was found to be downregulated in patients with low-trauma fractures 15 and positively correlated with MAR and BV/TV, 14 suggesting that it may be involved in bone structure maintenance and fracture pathological processes. In this study, it was found that miR-550a-3p is downregulated in OP and OPF, and has a good diagnostic effect in distinguishing between the two. Furthermore, according to the criteria established by the World Health Organization (WHO), the T-score serves as the gold standard for diagnosing osteoporosis. 31 Simply put, a lower T-score indicates that bone mineral density is more significantly below the peak bone mass of healthy young adults, resulting in a more fragile bone microstructure and reduced resistance to external forces, thereby increasing the susceptibility to fractures. 32 RANKL promotes the maturation of osteoclasts and enhances their bone resorption function by binding to RANK (the receptor) on the surface of osteoclast precursors. 33 OPG, secreted by osteoblasts, endothelial cells, and other cell types, competitively binds to RANKL, preventing RANKL from interacting with RANK and thus inhibiting osteoclast activation and reducing bone resorption. 34 In simple terms, OPG “inhibits bone resorption” while RANKL “promotes bone resorption,” and together they maintain the stability of bone mass. In clinical practice, monitoring 25-(OH) Vitamin D levels and maintaining them at adequate levels is one of the key measures for preventing and treating osteoporosis and reducing the risk of fractures. 35 In this study, miR-550a-3p was found to be significantly positively correlated with T-score, 25-(OH) Vitamin D, and OPG, while significantly negatively correlated with RANKL.
Notably, miR-422a and miR-194-5p have been identified as potential biomarkers for postmenopausal osteoporosis.12,13 Comparative analysis reveals distinct advantages of miR-550a-3p: While miR-422a and miR-194-5p showed differential expression in postmenopausal osteoporosis, previous studies reported miR-422a AUC values of 0.72-0.78 for osteoporosis diagnosis, and miR-194-5p AUC of approximately 0.75 in postmenopausal women. In contrast, miR-550a-3p demonstrated superior diagnostic performance in our study with AUC = 0.899 for OP versus Control and AUC = 0.911 for OPF versus OP, alongside sensitivities of 85.00% and 77.78% and specificities of 78.76% and 88.33%, respectively. Furthermore, miR-550a-3p uniquely provides predictive value for fracture healing outcomes (AUC = 0.851 for NH vs DH), a capability not established for miR-422a or miR-194-5p. The complementary functional mechanisms—miR-422a is associated with bone mineral density regulation, miR-194-5p is linked to estrogen deficiency-induced bone loss, and miR-550a-3p exhibits unique characteristics by being positively correlated with MAR and BV/TV. 14 Unlike miR-1224-5p, which coordinates the regulation of osteoblast and osteoclast differentiation, 9 miR-550a-3p appears to primarily affect bone homeostasis through the OPG/RANKL axis and potentially the Wnt/β-catenin pathway. These complementary characteristics suggest that a multi-miRNA panel combining miR-550a-3p, miR-422a, and miR-194-5p may provide enhanced diagnostic accuracy and broader clinical utility.
Based on the correlation results between miR-550a-3p and OPG/RANKL in this study, combined with the core biological processes of fracture healing, the regulatory mechanism of miR-550a-3p is hypothesized as follows (note: these are speculative hypotheses based on clinical correlations and existing literature, not supported by direct experimental evidence from this study): miR-550a-3p may indirectly regulate bone metabolism and fracture healing through multiple pathways: First, miR-550a-3p may target and inhibit negative regulators of chondrocyte maturation (such as transcriptional repressors of SOX9 and COL2A1), 36 thereby indirectly promoting chondrocyte maturation; or suppress negative regulators MMP-13, 37 facilitating MMP-13-mediated degradation and calcification of cartilage matrix, thereby accelerating cartilage callus formation and maturation to meet the repair needs of high-strain regions. Second, optimization of intramembranous ossification and balance of osteoblast-osteoclast: miR-550a-3p may activate the Wnt pathway by inhibiting DKK1, thereby promoting osteoblast differentiation; at the same time, it can inhibit osteoclast activation by upregulating OPG, reducing excessive resorption of callus. 38 As a miRNA, miR-550a-3p primarily exerts inhibitory effects on its direct target genes. The proposed promotional effects of miR-550a-3p on chondrocyte maturation or ossification pathway-related genes in this study are indirect regulatory effects mediated by targeting negative regulators of these pathways, rather than direct upregulation of target genes. This regulatory mode is consistent with the canonical biological function of miRNAs.
In addition to the above pathways, the potential effectors/targets of miR-550a-3p and its role in the basic multicellular unit (BMU)—the functional unit of bone remodeling—provide further clues for its hypothetical regulatory role. 39 Regarding the potential effectors/targets: 1) Previous studies have shown that miR-550a-3p can downregulate TIMP2, 29 a key molecule for extracellular matrix (ECM) remodeling during fracture healing 40 ; it is hypothesized that reduced miR-550a-3p in DH group may lead to the overexpression of TIMP2, impeding ECM turnover and delaying healing. 2) Decreased miR-550a-3p may increase the level of ERK1/2, 30 and the ERK signaling pathway can enhance RANKL-mediated osteoclast maturation. 41 Combined with the negative correlation between miR-550a-3p and RANKL observed in this study, it is speculated that miR-550a-3p may inhibit osteoclast activation by downregulating ERK1/2. Regarding BMU regulation: miR-550a-3p may reduce RANKL-mediated osteoclast maturation by downregulating ERK1/2, and indirectly modulate macrophage/osteomac activity through correlations with OPG (secreted by macrophages), thereby maintaining BMU homeostasis. These are all hypothetical inferences without direct experimental verification in bone cells.
Fracture healing is a precisely regulated process involving multiple stages such as inflammatory initiation, callus formation, and bone remodeling. 42 In recent years, a growing body of research has indicated that miRNAs play an important role in this process, exerting both promotional and inhibitory regulatory effects. For example, miR-193a-3p can promote fracture healing by enhancing osteoblast function 43 ; miR-133a can provide favorable conditions for bone repair by regulating the expression of key factors in osteogenic differentiation 44 ; while miR-203 has been confirmed to inhibit the expression of genes related to osteoblast differentiation, thereby exerting a negative regulatory effect on fracture healing. 45 In this study, the expression of miR-550a-3p in the delayed union group of patients with OPF was significantly lower than that in the normal union group. Moreover, its level was correlated with bone metabolism indicators such as T-score and 25-hydroxyvitamin D. ROC curve analysis showed that the AUC for distinguishing normal union from delayed union reached 0.851, and multivariate logistic regression further confirmed that it was an independent influencing factor for delayed union. These results suggest that miR-550a-3p may act as a miRNA with the potential to promote fracture healing, and its expression level can reflect the healing status of OPF patients, providing a new molecular indicator for early prediction of fracture healing outcomes.
miR-550a-3p exhibits promising clinical translational potential as a biomarker across three key scenarios: (1) Risk stratification, integrating serum miR-550a-3p detection into routine osteoporosis screening for middle-aged/elderly populations (e.g., postmenopausal women) and high-fracture-risk individuals to identify candidates for targeted interventions (e.g., anti-osteoporosis drugs, lifestyle adjustments); (2) Fracture prognosis assessment, where baseline levels guide surgical timing, fixation strategy (internal vs external fixation), and rehabilitation intensity for OPF patients—with high-risk (low-expression) patients potentially benefiting from aggressive fixation and intensive rehabilitation; (3) Healing monitoring, using serial measurements during follow-up to enable early detection of delayed healing risk and proactive interventions (e.g., nutritional supplementation, pharmacologic stimulation) before radiological changes. Potential benefits include reduced re-fracture rates, shortened recovery, optimized resource allocation, and improved quality of life. Key implementation challenges involve standardizing pre-analytical variables (sample collection/processing/storage) for cross-laboratory consistency, establishing validated reference ranges stratified by age, gender, ethnicity, and comorbidities (e.g., diabetes, hypertension) using large multi-center data, demonstrating cost-effectiveness versus existing biomarkers (e.g., 25-(OH) Vitamin D, OPG/RANKL) and imaging (e.g., X-ray, micro-CT), and navigating regulatory pathways for clinical test approval with validation in diverse cohorts—all addressed in future research directions.
In summary, this study is the first to systematically explore the clinical value of miR-550a-3p in OPF. It was found that miR-550a-3p can not only effectively distinguish between healthy controls, OP patients, and OPF patients, but also has an independent predictive effect on the fracture healing outcome of OPF patients. These findings indicate that miR-550a-3p is expected to become a new biomarker for the diagnosis, condition monitoring, and prognosis evaluation of osteoporotic fractures, providing experimental evidence for optimizing clinical diagnosis and treatment strategies.
This study has several limitations that need to be acknowledged. First, this is a single-center observational study with a relatively limited sample size, which may affect the generalizability of the results to other populations or regions. Second, as a clinical observational study, the study only explored the correlation between miR-550a-3p expression and osteoporotic fractures as well as delayed healing, with its regulatory mechanism proposed hypothetically. The specific molecular mechanism awaits verification via further in vitro cell experiments and in vivo animal models, whose absence limits systematic analysis of miR-550a-3p′s in vivo regulatory roles. Third, the follow-up period of this study was 6 months, and the long-term dynamic changes in miR-550a-3p expression and its association with long-term fracture healing outcomes (e.g., 1-year or 2-years re-fracture rate) were not observed. Fourth, the present study only detected the expression of miR-550a-3p in serum, and lacked the detection data of its expression level and spatial distribution in local bone tissues and fracture callus. Fracture healing is a typical local pathological process, and serum miR-550a-3p levels cannot fully reflect the local molecular regulatory dynamics of bone injury sites, which limits the in-depth clarification of its spatial regulatory role in bone metabolism and fracture healing. Fifth, the current mechanistic research relies mainly on clinical correlation analysis and literature inference, lacking direct experimental evidence (e.g., target gene or signaling pathway validation) to confirm miR-550a-3p′s regulatory role in bone metabolism and fracture healing, rendering the proposed mechanism relatively superficial. In future research, we plan to address these limitations by: (1) conducting multi-center, large-sample size studies in collaboration with multiple medical institutions across different regions, including patients of different ethnicities and age groups, to validate the diagnostic and prognostic value of miR-550a-3p in osteoporotic fractures; (2) using in vitro cell models to clarify its regulatory pathways in osteogenic differentiation, osteoclast activation, and ECM remodeling; meanwhile, establishing mouse/rat osteoporotic fracture models to carry out in vivo intervention studies through miRNA agomir/antagomir-mediated overexpression/knockdown experiments. We will assess fracture healing speed and quality via X-ray, micro-CT, and histopathological staining, and detect changes in osteogenic/osteoclastic markers and key signaling pathway molecules to clarify miR-550a-3p′s in vivo regulatory mechanism and support clinical translation. (3) extending the follow-up period to investigate the long-term predictive effect of miR-550a-3p on fracture healing and re-fracture risk, providing more comprehensive evidence for its clinical application; (4) detecting the expression of miR-550a-3p in bone tissue and fracture callus, comparing its expression differences between the systemic circulation and local lesion sites, and further exploring its spatial regulatory mechanism in bone metabolism, and strengthening the correlation between its systemic serum expression and local pathological changes of bone injury; (5) combining multi-omics techniques to screen for other miRNAs or proteins that interact with miR-550a-3p in osteoporosis and osteoporotic fractures, constructing a bone metabolism-related regulatory network, and providing a more comprehensive theoretical basis for the development of targeted therapeutic strategies; (6) Addressing key clinical translation challenges: First, standardizing serum miR-550a-3p detection (e.g., optimizing RT-qPCR protocols, establishing quality control standards) to ensure cross-laboratory consistency and reliability; second, establishing population-specific reference ranges (stratified by age, gender, ethnicity) using large-sample multi-center data to enhance clinical applicability; third, developing targeted interventions (e.g., miRNA mimics/inhibitors) and evaluating their preclinical safety and efficacy to facilitate the transition from biomarker to therapeutic target.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.