
Abstract
Background
Postoperative pain management following unicompartmental knee arthroplasty (UKA) remains a major challenge during the perioperative period. Local infiltration analgesia (LIA) using multimodal cocktail drugs injections has become an effective approach for perioperative pain control in UKA. However, most existing studies have focused on the use of cocktail drugs in total knee arthroplasty (TKA), whereas differences in their intraoperative application between UKA and TKA have rarely been reported.
Methods
This narrative review synthesizes literature identified from three databases. A comprehensive review of recent literature was conducted to summarize the different categories of cocktail drugs, their applications, efficacy, and evolving roles in UKA, and to compare their use with that in TKA.
Results
Local injection of cocktail drugs, as an essential component of multimodal analgesia, has been widely applied during UKA. The cocktail drug approach provides synergistic advantages by combining multiple agents, resulting in enhanced analgesic and anti-inflammatory effects, prolonged duration of pain relief, and hemostatic benefits. At present, the primary method of administration involves intraoperative periarticular local infiltration. In most patients, postoperative pain scores and analgesic requirements during the early postoperative period, particularly within the 1–2 days after surgery, are lower after UKA than after TKA. Therefore, the formulations and dosages of cocktail drugs used in the two operations are not entirely identical.
Conclusions
Cocktail drug therapy is characterized by a simple administration procedure. Current evidence indicates that, for selected UKA patients, periarticular cocktail drugs injections can facilitate postoperative pain control and early functional recovery. Given the significant differences in surgical trauma, pain intensity, and tissue exposure between UKA and TKA, the direct application of TKA formulations to UKA should be approached with caution. However, UKA-specific studies remain limited, and further research is warranted to refine these protocols.
Keywords
Introduction
Knee osteoarthritis (KOA) is a global health problem and one of the most common osteoarticular diseases among middle-aged and elderly individuals. It is primarily attributed to chronic wear leading to degeneration of the knee joint. Clinically, it manifests as knee pain of varying degrees and functional impairment, 1 affecting over 364 million people worldwide. 2
With the increasing adoption of the stepwise treatment concept for knee joint diseases, unicompartmental knee arthroplasty (UKA), as a form of partial knee replacement, has become an established surgical option for patients with advanced KOA when the disease has not yet progressed to the entire compartment. 3 A consensus statement issued during a joint conference of the British Association for Surgery of the Knee (BASK) and the European Knee Society (EKS) recommended that UKA should be considered a successful alternative to total knee arthroplasty (TKA) for eligible joint replacement patients. 4 Clinical studies have demonstrated that the quality of postoperative analgesia following UKA directly influences the duration of hospital stay, significantly affects patient compliance with functional rehabilitation exercises, and may delay postoperative functional recovery. 5 Therefore, precise perioperative analgesia, as a critical component in enhancing clinical satisfaction and implementing enhanced recovery after surgery (ERAS) protocols, has become a major research focus in the field of joint surgery. 6 In recent years, researchers have been working to optimize multimodal analgesic strategies to develop personalized pain management protocols better suited to the characteristics of UKA. 7 Local infiltration analgesia (LIA) is one of the key modalities in multimodal analgesic strategies. 8
Cocktail drugs (also known as multimodal analgesic drugs) represent an increasingly adopted approach in modern clinical practice for LIA. Typically composed of two or more combined medications to achieve synergistic effects, this method is metaphorically termed “cocktail”.
9
Common components include local anesthetics, sympathetic nervous system modulators, corticosteroids, analgesic agents, and other adjuncts such as tranexamic acid and magnesium sulfate. These agents collectively provide analgesic, local anti-inflammatory, and hemostatic effects, thereby reducing postoperative pain.
10
The injection of cocktail drugs is widely recognized as one of the effective methods in multimodal analgesia strategies for UKA. In a study on UKA, 138 ESSKA (European Society for Sports Traumatology, Knee Surgery and Arthroscopy) members from 34 different countries participated in a survey. Over 75% of surgeons reported using periarticular injections or local infiltration analgesia with cocktail drugs during UKA, surpassing the utilization rates of oral medications, preoperative nerve blocks, and postoperative nerve blocks.
11
The application of cocktail drugs for LIA during UKA procedures demonstrates efficacy in improving postoperative pain control during the early postoperative period and enhancing knee functional recovery outcomes (Figure 1). With increasing clinical application, research teams continue to explore the therapeutic efficacy of cocktail drugs based on different drug combinations and ratios, while also expanding their potential indications. Schematic illustration of intraoperative periarticular cocktail drugs administration during UKA.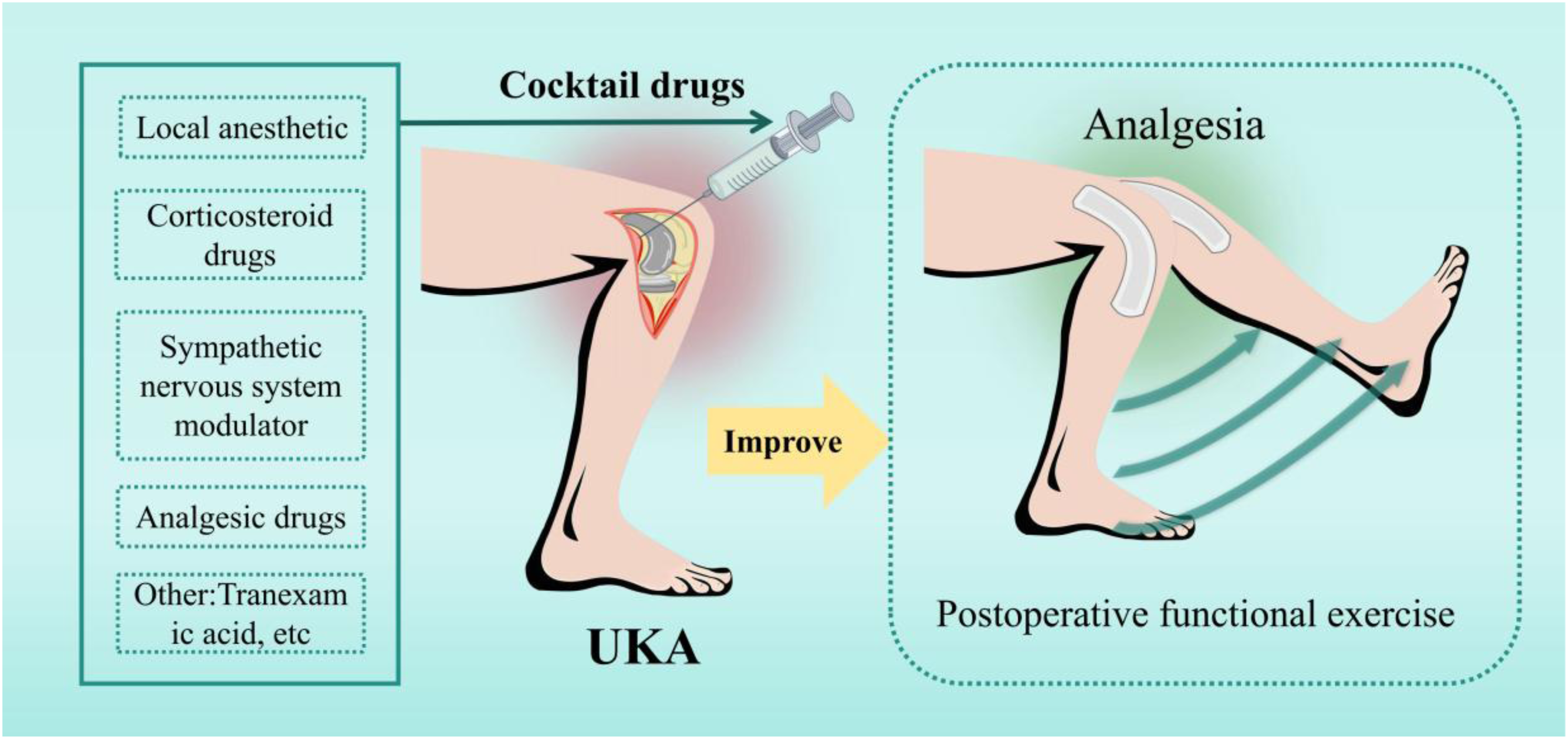
Current research primarily focuses on the application of cocktail drugs with varying compositions in TKA, while their use in UKA has received comparatively less attention. Furthermore, comparative analyses of cocktail drug application between these two surgical procedures are notably scarce. To explore this understudied area, this review examines the recent advancements in cocktail drug applications for UKA, including their composition, delivery techniques, and efficacy. It also compares the differences in cocktail drug usage between UKA and TKA. By evaluating existing studies, this review aims to summarize the current evidence, identify research gaps, and provide a reference for the rational use of cocktail drugs in UKA. In this review, the term LIA is equivalent to periarticular injections (PAI). It specifically refers to periarticular infiltration performed intraoperatively, rather than periarticular injections administered postoperatively.
Research strategy
The literature search was performed in three databases (PubMed, Web of Science, and Embase) up to September 30, 2025. The search strategy combined terms and synonyms related to UKA and cocktail drugs, including ‘UKA,’ ‘unicompartmental knee arthroplasty,’ ‘periarticular infiltration,’ ‘periarticular injections,’ and ‘cocktail drugs.’ An example of the PubMed search strategy was as follows: ((“unicompartmental knee arthroplasty” OR “unicondylar knee arthroplasty” OR “partial knee arthroplasty” OR UKA OR “total knee arthroplasty” OR TKA) AND (“periarticular injection” OR “periarticular infiltration” OR LIA OR “cocktail drugs” OR “cocktail therapy”)). Similar strategies were adapted for Web of Science and Embase using equivalent keywords and database-specific indexing terms. All retrieved records were imported into reference management software and duplicates were removed. Titles and abstracts were screened to identify potentially relevant studies. The full texts of eligible articles were then reviewed. Two authors independently screened the literature and determined the final inclusion, aiming to highlight representative studies of the main findings in the field. Discrepancies were resolved through discussion and consensus.
Overall, 1559 records were initially identified through database searching. After removal of duplicates and screening of titles and abstracts, 113 articles were assessed in full text, and 82 studies were ultimately included in this review (Figure 2). This narrative review does not claim systematic evidence synthesis. The review did not involve the collection of primary patient data; therefore, ethical approval was not required. In addition, only articles published in English were included, which may introduce language bias and potentially exclude relevant studies published in other languages. Flow diagram of literature search and study selection.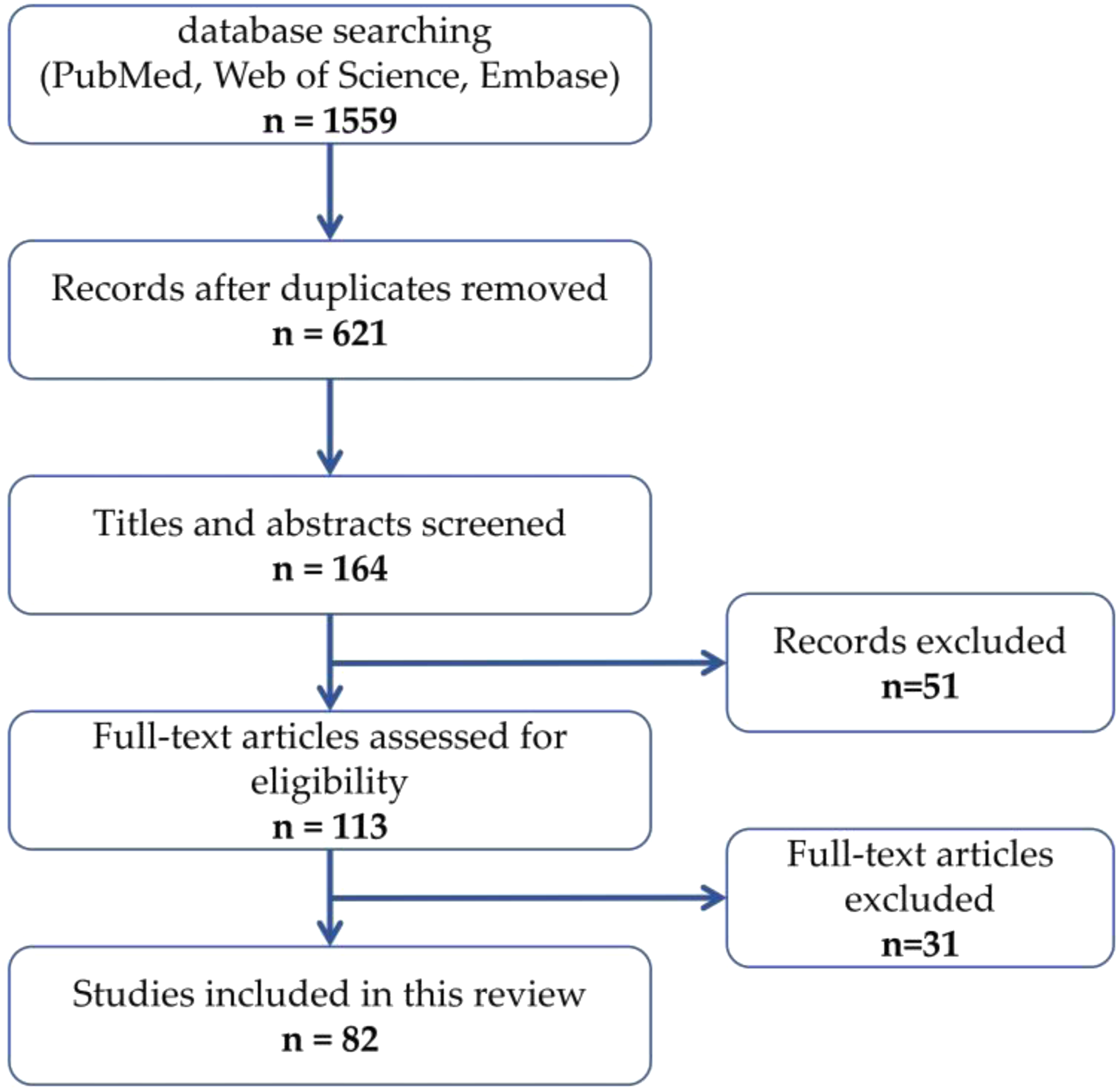
As a narrative review, this article synthesizes evidence without formal meta-analysis. To enhance transparency when summarizing the literature, included studies were grouped according to study size categories rather than formal evidence grading. The categories were defined as follows: Category A: Systematic review and Meta-analysis; Category B: Large human studies (Sample size ≥ 100); Category C: Medium human studies (50 ≤ Sample size < 100); Category D: Small human studies (Sample size < 50). All information is annotated in (Table 3). These categories are presented for descriptive purposes only and do not represent a formal hierarchy of evidence strength.
Types of cocktail drugs
Local anesthetics
Local anesthetics serve as the primary components of cocktail drugs, with commonly used agents including ropivacaine and bupivacaine. Chen et al. 14 demonstrated that incorporating bupivacaine into cocktail drugs for injection facilitates postoperative pain control, enables early mobilization, and reduces hospital stay in joint replacement patients. A study by Nakasone et al. 15 revealed that using bupivacaine as the local anesthetic component in cocktail drugs provides effective analgesia and supports the achievement of enhanced recovery goals. To prolong the duration of action, liposomal bupivacaine has also been incorporated into cocktail drugs, theoretically extending postoperative analgesia to 72 h. 16 Liposomal bupivacaine has been reported to exhibit a prolonged duration of action and reduced peak plasma concentration compared to conventional bupivacaine. 17
However, Bowen et al. 18 found that while liposomal bupivacaine achieves comparable analgesic effects, its high cost suggests that surgeons and hospitals should consider it a potential area for cost savings. A comparative cohort study by Danoff et al. 19 demonstrated that although bupivacaine in cocktail drugs provides certain pain control benefits, ropivacaine is preferred due to its lower cost and fewer adverse effects. Weston-Simons et al. 20 reported that adding ropivacaine to cocktail drugs in knee arthroplasty results in effective postoperative pain management, facilitating early rehabilitation. Ropivacaine exhibits lower central nervous system toxicity and, at low doses, selectively blocks sensory nerves without impairing motor function. This property makes it suitable for patients requiring early postoperative functional exercise. 21 A review by King et al. 22 indicated that ropivacaine’s motor nerve blockade effect is dose-dependent. Studies evaluating concentrations between 0.25% and 0.75% suggest that higher concentrations provide superior pain relief but may increase the risk of nausea and vomiting. Currently, ropivacaine is typically diluted with normal saline to approximately 0.1–0.25% for clinical use, though specific ratios and dosage vary based on individualized needs.
Corticosteroids
Corticosteroids effectively suppress the release of inflammatory factors, reducing edema and exudation caused by inflammatory responses. They can decrease the sensitivity of peripheral nociceptors and neural excitability, thereby alleviating postoperative pain in knee arthroplasty patients. 23 When using corticosteroids clinically, caution is required because of concerns regarding potential infection risk, particularly with systemic administration. However, in cocktail drug therapy, corticosteroids are applied locally, which results in lower systemic exposure compared with systemic administration. Zhong et al. 24 found that adding corticosteroids to cocktail drugs significantly enhanced analgesic effects and promoted early rehabilitation without increasing postoperative infection rates.
Common corticosteroids used in cocktail drugs include dexamethasone, betamethasone, triamcinolone acetonide, and methylprednisolone. Wang 25 observed that adding dexamethasone to cocktail drugs in joint arthroplasty reduced opioid consumption and decreased postoperative nausea and vomiting. Liu et al. 26 evaluated the efficacy and safety of betamethasone in cocktail drugs for UKA, demonstrating its effectiveness in providing early acute analgesia and improving knee function recovery without elevating complication rates. In a controlled study using UKA conducted by Ng et al., 27 the addition of triamcinolone acetonide to LIA reduced postoperative pain and inflammatory response, facilitated early recovery of knee function, and was associated with no major complications. Kulkarni et al. 28 incorporated methylprednisolone into cocktail drugs and found it effectively relieved early postoperative pain while accelerating knee flexion recovery.
The study confirmed that the use of corticosteroid in the cocktail drugs for UKA does not increase inflammatory complications by monitoring inflammatory markers (CRP and ESR).26–28 Although current clinical evidence does not strongly associate local corticosteroid use with significant changes in wound drainage, periprosthetic joint infection rates, or wound healing speed, local administration is considered relatively safe. However, injection sites should be carefully selected to avoid direct needle contact with cartilage tissue.
Sympathetic nervous system modulators
Sympathetic nervous system modulators play a regulatory role in cocktail drug formulations by modulating sympathetic nerve activity, improving blood circulation, and prolonging the intensity and duration of analgesic effects. 29 Commonly used agents include epinephrine and dexmedetomidine.
Edinoff et al. 30 demonstrated that when used as an adjunct in LIA, epinephrine constricts small blood vessels around the knee joint, slowing the absorption of cocktail drugs by surrounding tissues. Essving et al. 12 confirmed its efficacy through a cohort study of epinephrine administered as part of a cocktail therapy regimen for UKA. Chareancholvanich et al. 13 also confirmed that this prolongs drug retention in the surgical area, enhancing and extending the analgesic effect of nerve blockade. Nikhar et al. 31 reported that adding dexmedetomidine to nerve blocks significantly increased the duration of motor blockade, sensory blockade, and analgesia, thereby improving the efficacy and longevity of cocktail drugs. Emerging evidence suggests that magnesium ions may also indirectly reduce excessive sympathetic nervous system activation. 32 In a study by Wang et al., 9 the addition of magnesium sulfate (MgSO4) to traditional cocktail drugs markedly extended analgesia duration and reduced opioid consumption.
Wyns et al. 33 highlighted that chronic pain patients often exhibit sympathetic nervous system dysregulation. Prolonged stress not only exacerbates pain but also contributes to sleep disturbances and mood disorders. Appropriate modulation of sympathetic activity may improve sleep, mood, and overall quality of life.
Analgesic agents
Analgesic agents are primarily used to alleviate pain of varying intensities. Depending on the type and severity of pain, commonly used options include opioids, non-steroidal anti-inflammatory drugs (NSAIDs), and selective COX-2 inhibitors. Burda et al. 34 demonstrated that the rational use of analgesic agents significantly improves patient comfort and plays a crucial role in postoperative recovery. However, the trend in selecting analgesic agents for cocktail drugs has evolved over time, with a growing emphasis today on multimodal and opioid-sparing analgesic strategies.
Frequently employed NSAIDs include flurbiprofen axetil and ketorolac. In a cohort study of joint arthroplasty, Wang et al. 35 incorporated flurbiprofen axetil into cocktail drugs, revealing that it markedly enhanced analgesic efficacy and improved patients’ sleep quality. Laoruengthana et al. 36 observed that adding ketorolac to cocktail drugs resulted in superior postoperative knee flexion and straight-leg raising compared to controls, achieving effective analgesia without adverse effects. Another study comparing the selective COX-2 inhibitor parecoxib with ketorolac found comparable analgesic outcomes. 37 However, caution is warranted: research indicates that NSAIDs (e.g., ketorolac) in cocktail drugs for patients with chronic kidney disease (CKD) undergoing knee arthroplasty may increase the risk of acute kidney injury. 38
Common opioids such as morphine and fentanyl have also been utilized. Luo et al. 39 reported that cocktail drugs containing morphine provided superior and longer-lasting analgesia compared to ropivacaine alone, while also improving sleep quality and accelerating rehabilitation. Campos et al. 40 found that fentanyl as an adjunct in cocktail drugs enhanced postoperative pain control, reduced the need for sustained opioid use, and did not increase postoperative bleeding. Current perioperative analgesia strategies increasingly emphasize opioid-sparing approaches in order to minimize opioid-related adverse effects such as nausea, sedation, and respiratory depression. Consequently, the routine inclusion of opioids in cocktail drugs is not universally recommended. Their use should be considered selectively and balanced against the broader goal of minimizing perioperative opioid exposure.
Other adjunctive agents
In cocktail drug formulations, additional agents such as tranexamic acid (TXA) and sodium bicarbonate (NaHCO3) play significant roles. Tranexamic acid reduces postoperative bleeding by inhibiting fibrinolysis, thereby improving surgical outcomes. 41 A systematic review and meta-analysis by Weng et al., 42 incorporating nine clinical studies involving 744 patients, demonstrated that adding TXA to cocktail drugs during UKA significantly reduced perioperative transfusion rates, primary blood loss, postoperative drainage volume, hidden blood loss, and total blood loss compared to control groups. Wiktor et al. 43 found that local injection of TXA in UKA decreased perioperative blood loss without increasing wound complication risks, while also shortening hospital stays. However, Moorthy et al. 44 reported that although TXA effectively reduced bleeding in UKA patients, it did not significantly improve postoperative knee function. Zhu et al. 45 incorporated NaHCO3 as an adjunct in UKA cocktail drugs, showing that this modified formulation prolonged postoperative analgesia, reduced analgesic consumption, and enhanced functional recovery. These findings were corroborated by similar research from Wang et al. 9
Administration methods of cocktail drugs
Intraoperative local infiltration
In UKA procedures, the predominant method for administering cocktail drugs is periarticular local infiltration. Studies on injection sites reveal that knee joint tissues contain abundant nociceptors.
29
Particularly pain-sensitive structures include the patellar tendon, infrapatellar fat pad, lateral collateral ligament insertion, iliotibial band insertion, suprapatellar bursa, and posterior capsule (Figure 3). Current evidence supports injections into the lateral capsule, collateral ligaments, tendon sheaths, quadriceps tendon, fat pad, and subcutaneous tissues.
46
Tran et al.
47
provided anatomical confirmation of neural distribution within the posterior capsule, theoretically supporting posterior capsular injections for neural blockade. The concentration of nociceptors within the knee joint. QT = quadriceps tendon, PT = patellar tendon, MCL = medial collateral ligament, and LCL = lateral collateral ligament.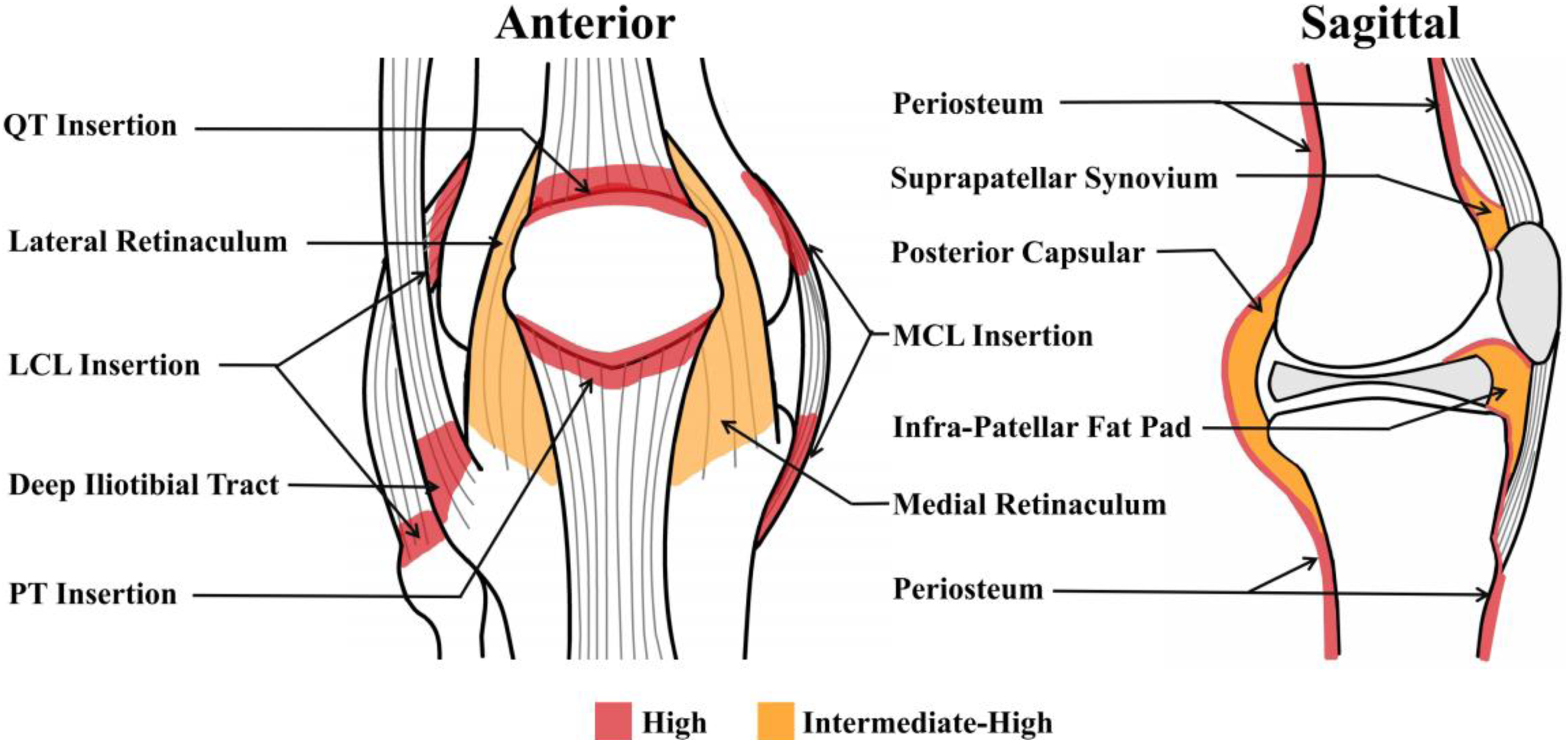
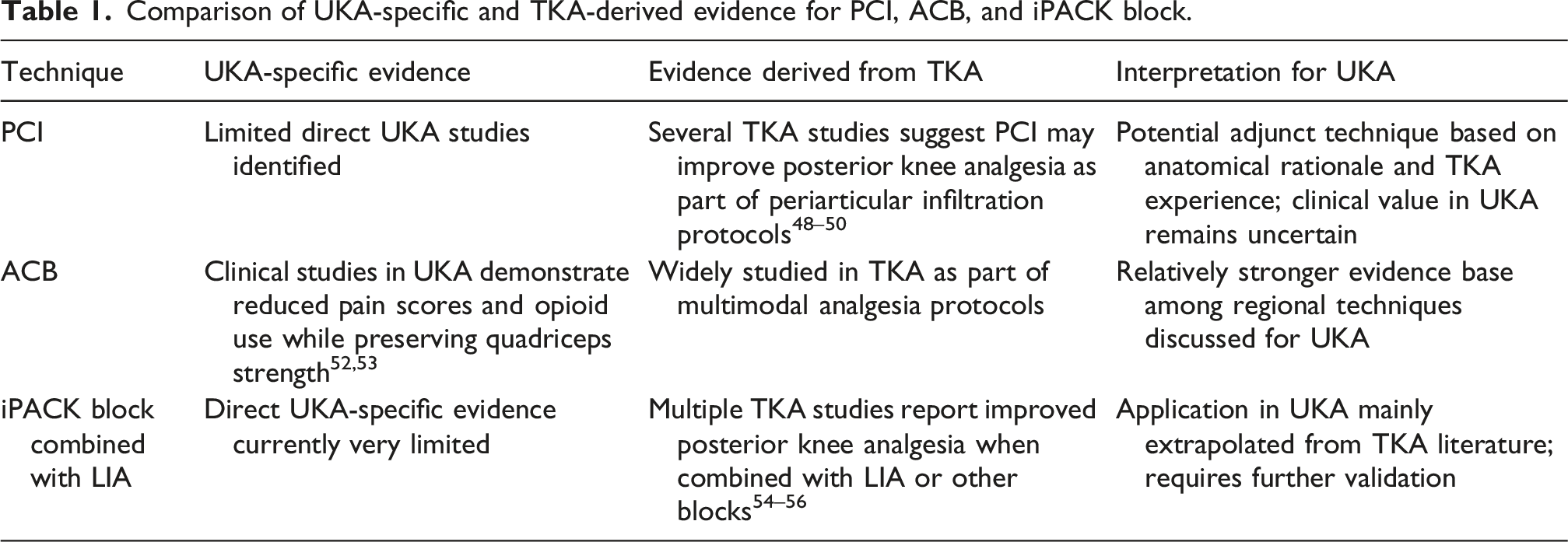
Among the currently available published literature, the posterior capsular injection (PCI) has been predominantly studied in the context of TKA. There is a notable paucity of randomized controlled trials and prospective cohort studies specifically evaluating the role of PCI preservation in UKA. The study by Fang et al. 48 suggests that PCI during TKA can help alleviate postoperative knee pain, but it should avoid the central area of the posterior capsule to prevent proximity to the popliteal vascular and nerve bundles. Schwartz’s 49 review also indicates that the LIA area covering the posterior capsule is gradually being adopted by more people. However, the randomized controlled trial conducted by Pinsornsak et al. 50 shows that PCI in TKA does not significantly improve postoperative pain or the use of opioids, and there is no significant difference compared to using only standard peri-articular infiltration. These different research results remind us to be cautious when choosing PCI, and to combine the surgeon’s familiarity with the anatomical structure to avoid damaging blood vessels and nerves, and avoid injecting excessive amounts of medication.
Currently, in the current surgical practice, there is no unified standard for injection volume and specific sites.
51
Most available data are derived from TKA populations, and direct UKA-specific comparative studies are scarce. The potential role of PCI in UKA is primarily based on anatomical considerations and extrapolations from TKA experience. However, its clinical efficacy and safety in UKA cohorts require further studies. Based on the current understanding of knee joint pain receptors distribution, the following injection scheme may be considered: after the osteotomy step and before the implantation of the artificial prosthesis, ensure safety and consider injecting into the posterior capsule (Figure 4). Then, sequentially inject into the anterior capsule, the quadriceps tendon, the infrapatellar fat pad, and the attachment points of the ligaments. Perform posterior capsule injections of cocktail drugs after osteotomy completion and prior to prosthesis implantation.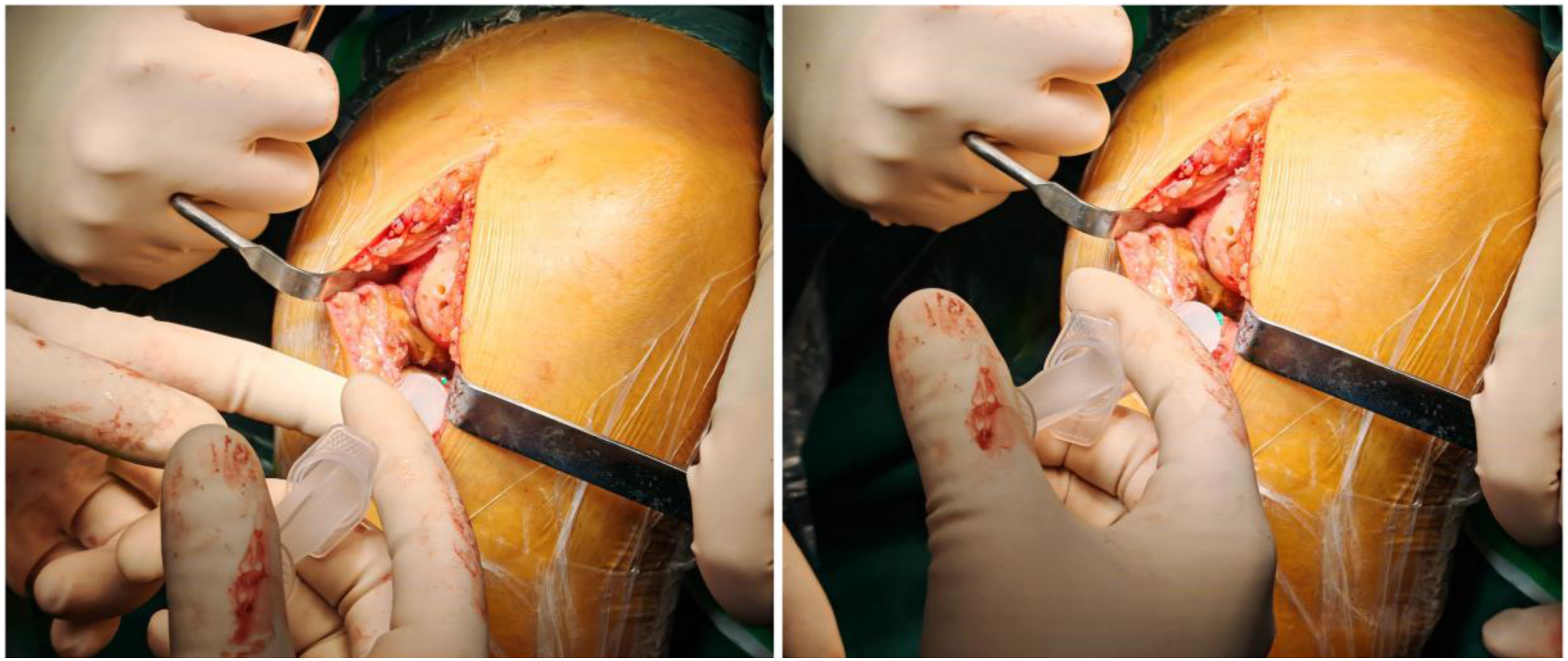
Combine other analgesia methods
Guided by the ERAS guidelines, various different analgesic methods have been developed. Among these, adductor canal block (ACB) has been investigated in both TKA and UKA populations. Clinical studies in UKA have shown that ACB can reduce postoperative pain, decrease opioid usage, without significant reduction in quadriceps muscle strength was observed.52,53
Another technique that has gained attention in knee arthroplasty is the infiltration between the popliteal artery and capsule of the posterior knee (iPACK) block. Poonam et al. 54 suggested that iPACK block has the potential to alleviate postoperative pain in TKA. Zhang et al. 55 and Bohumilik et al. 56 both indicated that iPACK block can enhance the analgesic effect in the posterior part of the knee joint after TKA and accelerate pain relief. However, in the currently available literature, iPACK block is almost exclusively studied in the context of TKA, and there are few reports specifically evaluating the effect of iPACK block in UKA as an operation type. The application of iPACK block in UKA should be considered largely extrapolated from TKA literature. While its anatomical rationale suggests potential benefit for posterior knee pain control, its effectiveness and safety in UKA remain to be validated by future clinical studies.
Comparison of UKA-specific and TKA-derived evidence for PCI, ACB, and iPACK block.
Differences in application between UKA and TKA
Currently, cocktail drugs are widely used for analgesia in UKA, though most clinical teams employ similar formulations to those used in TKA. However, a cohort study by Leiss et al. 57 of 4144 patients demonstrated significantly lower postoperative pain scores in UKA compared to TKA during the early postoperative period, particularly on postoperative days 1–2. During hospitalization, UKA patients required fewer opioids and reported better subjective outcomes. Kalbian et al. 58 also found that UKA patients had reduced analgesic requirements relative to TKA.
Differences between UKA and TKA. (drug formulations and drug dosages are derived from literature-based observations and expert interpretation, not evidence-based recommendations).

Differences in drug formulations
Compared to UKA, TKA involves greater surgical trauma, more extensive tissue exposure, and larger osteotomy areas, resulting in more severe pain. Thus, TKA cocktail drugs emphasize multimodal analgesia and synergistic effects. 62 These regimens commonly incorporate long-acting local anesthetics, corticosteroids, and adjunctive agents (such as epinephrine or morphine) to synergistically alleviate both inflammatory responses and acute postoperative pain.
In contrast, UKA’s smaller trauma profile warrants a focus on targeted local analgesia and minimizing systemic side effects. Since the contralateral compartment retains native cartilage, reducing or avoiding corticosteroids may be preferable. NSAIDs may be considered for inclusion in the formulation to control local inflammatory responses while potentially reducing opioid consumption.
Differences in drug dosages
Wiktor et al. 43 retrospectively analyzed UKA cocktail drugs volumes, noting they are typically half those used in TKA, as excessive fluid may increase wound drainage risks. TKA’s greater postoperative pain often necessitates higher total drug doses. According to the systematic review by King et al., 22 it may be suggested that for TKA procedures where ropivacaine is selected as the local anesthetic, concentrations of (0.25%∼0.5% & 2.5∼5 mg/ml),total doses of approximately (150–200 mg) could be considered. The appropriate use of low-dose corticosteroids may also be recommended. At present, there is no research that directly compares the systematic differences in the local anesthetic concentration design between UKA and TKA. However, by combining the relevant research on TKA, it can be inferred that for UKA, lower ropivacaine concentrations (0.1%∼0.25% & 1∼2.5 mg/ml) or reduced total doses (100–150 mg), minimal corticosteroids, and lower NSAID doses align with the “minimum effective dose” principle. This approach mitigates postoperative nausea or cardiovascular risks while supporting rapid recovery. Dosage adjustments should account for individual pain tolerance and clinical context.
Efficacy of cocktail drugs
Mechanism research and clinical application situation
Existing evidence indicates that LIA and regional anesthesia techniques can mitigate postoperative stress, reduce inflammatory responses, and suppress cytokine release. However, these findings are predominantly extrapolated from TKA and THA studies, with a notable paucity of independent research focusing specifically on UKA. Kuchálik et al. 63 performed LIA with a cocktail of ketorolac and local anesthetics during THA surgery. They found that the interleukin-6 (IL-6) and CRP levels in the experimental group decreased compared to the control group, showing a better anti-inflammatory effect. Wang et al. 64 conducted a randomized controlled trial on TKA in which glucocorticoids were incorporated into the cocktail drugs. The results demonstrated that, 24 h postoperatively, the experimental group exhibited significantly lower levels of IL-6 and CRP, reduced pain intensity, and improved knee range of motion compared to the control group. However, it should be noted that the efficacy of cocktail drugs stems from the combination of several pharmacological mechanisms. Glucocorticoids, NSAIDs, and local anesthetics each exert their effects through different inflammatory pathways. The analgesic effect itself can also reduce postoperative stress responses and the release of cytokines. Therefore, the specific pharmacological mechanism of the cocktail drugs should be determined based on different drug formulations. Evidence specific to UKA remains limited and requires further investigation.
In clinical studies, Meier et al. 65 found that the use of cocktail drugs for LIA during UKA significantly reduced the pain scores of patients during postoperative activities. In the UKA controlled experiment conducted by Essving et al., 12 the experimental group that used cocktail drugs for LIA experienced a significant reduction in pain, a shorter hospital stay, and improved early knee joint range of motion. The studies by Liu et al. 66 and Lan et al. 53 also consistently demonstrated that the use of cocktail drugs for LIA in UKA can reduce the frequency of analgesic drug use and improve the early range of knee joint movement, without affecting motor function. Luo et al. 39 further reported that cocktail drugs formulations can extend analgesic efficacy up to 48 h postoperatively, enhance sleep quality, and accelerate rehabilitation without increasing adverse events. The research findings by Salwan et al. 67 indicate that the cocktail drugs therapy can effectively reduce opioid requirements and shorten the average hospital stays. Furthermore, current evidence reveals no significant negative impact on postoperative infection rates or wound healing time. In summary, existing studies suggest that periarticular cocktail drugs injections may improve postoperative pain control in UKA.
Drug safety and precautions
Cocktail drugs are administered via local injection and generally exhibit favorable applicability and safety profiles. However, in clinical practice, it is not advisable to apply a uniform formulation across all patients; instead, treatment should be tailored by comprehensively considering individual patient conditions and the distinct pharmacological characteristics of the drugs involved.
As the primary component in cocktail drugs combinations, local anesthetics are administered at higher doses during LIA, necessitating vigilance against the risk of local anesthetic systemic toxicity (LAST). Current research supports limiting the total ropivacaine dose to approximately 3 mg/kg during LIA, with a maximum total volume not exceeding 200∼225 mg. 68 The maximum tolerable dose is influenced by patient weight, concomitant epinephrine use, and factors such as multiple injections within a short timeframe or overlapping nerve blocks. During and following LIA, heightened monitoring of patient consciousness, hemodynamics, and cardiac rhythm is essential. Previous reports indicate that although the incidence of LAST associated with LIA is considered low, it is not negligible, particularly in elderly or frail patients and in situations where multiple regional anesthesia techniques are combined. In cases of suspected LAST, treatment should follow established lipid rescue protocols. Current guidelines from the American Society of Regional Anesthesia and Pain Medicine (ASRA) recommend an initial intravenous bolus of 20% lipid emulsion at approximately 1.5 mL/kg, followed by a continuous infusion of 0.25 mL/kg/min. If cardiovascular instability persists, the bolus may be repeated and the infusion rate increased, while respecting recommended maximum cumulative doses. Lipid emulsion should therefore be immediately available wherever large doses of local anesthetics are administered. 69 This precaution is particularly important when periarticular infiltration is combined with additional regional blocks, which may increase the cumulative dose of local anesthetics.
In UKA, a portion of the native articular cartilage is retained, which has raised theoretical concerns regarding potential chondrotoxicity associated with certain agents used in cocktail drugs, particularly local anesthetics and corticosteroids.70,71 It should be emphasized that most experimental and clinical evidence describing chondrotoxic effects originates from studies involving intra-articular exposure, where drugs are directly in contact with cartilage tissue. In contrast, LIA is typically administered in peri-capsular and soft-tissue structures rather than directly within the joint cavity. Although these findings justify cautious drug selection in UKA, the clinical significance of chondrotoxicity associated with periarticular infiltration remains uncertain. At present, there is limited direct evidence linking periarticular cocktail injections in UKA to adverse outcomes such as cartilage deterioration or increased revision risk. Consequently, these concerns should be interpreted primarily as precautionary considerations rather than confirmed clinical risks. Epinephrine is commonly added at low concentrations to induce local vasoconstriction, thereby reducing bleeding and delaying systemic absorption of local anesthetics, which prolongs analgesic duration. However, studies have shown that certain high-volume regimens are associated with an increased incidence of early incision exudation, 72 suggesting that high-dose or high-concentration protocols should be avoided. NSAIDs may precipitate acute renal impairment by inhibiting renal prostaglandin synthesis, 38 especially elderly patients, those with hypovolemia, or those with pre-existing chronic kidney disease. The use of cocktail drugs should be considered to carry potential nephrotoxicity, and thus they should be administered with caution or at reduced dosages. Existing evidence from broader arthroplasty populations suggests that TXA can be used safely in many patients when appropriate perioperative thromboprophylaxis protocols are followed. 73 However, these findings should not be generalized to all patients with thrombotic risk factors. Careful individualized risk assessment remains essential. In particular, patients with recent thromboembolic events, active thrombosis, or severe renal dysfunction may require additional caution or avoidance of TXA according to existing clinical recommendations.
Theoretically, any drug carries potential safety risks; however, the extent of available evidence and degree of clinical attention vary considerably among different agents. Thus, rather than attempting to exhaustively list all possible adverse effects for every drug, this section focuses on briefly discussing several of the more commonly referenced drugs mentioned above, with the aim of reinforcing awareness regarding drug safety.
Discussion
Common classifications of cocktail drugs and their research findings and key safety notes.

Nevertheless, the magnitude of surgical trauma, pain intensity, and tissue exposure differs significantly between UKA and TKA,57–61 and direct transfer of TKA-optimized formulations to UKA should therefore be approached with caution. Pharmacological interventions should adhere to the principle of providing adequate therapeutic efficacy at the lowest possible doses to minimize adverse effects and complications.77,78 For instance, both the Expert Consensus Guidelines on the Perioperative Use of Opioids in the United Kingdom 79 and the Centers for Disease Control and Prevention (CDC) Clinical Practice Guideline for Prescribing Opioids for Pain 80 emphasize that opioids should be reserved for essential indications, with utilization minimized within clinically appropriate boundaries. The ERAS protocols also emphasize the use of multimodal analgesia to reduce reliance on opioids and minimize adverse effects such as nausea, respiratory depression, and delirium, which is one of the core objectives of ERAS. 81 Currently, there are no standardized protocols across studies regarding drug selection, dosing, administration routes, and timing for cocktail drug formulations. Consequently, clinical practice is largely guided by individual surgeon experience and personal preference. A universally recognized optimal formulation for cocktail drug injections in UKA has yet to be established. Individualized regimens based on age, coagulation status, and pain tolerance threshold remain crucial. 82 Throughout the treatment process, drug safety must be comprehensively evaluated, and personalized therapeutic strategies should be formulated according to each patient’s specific conditions.
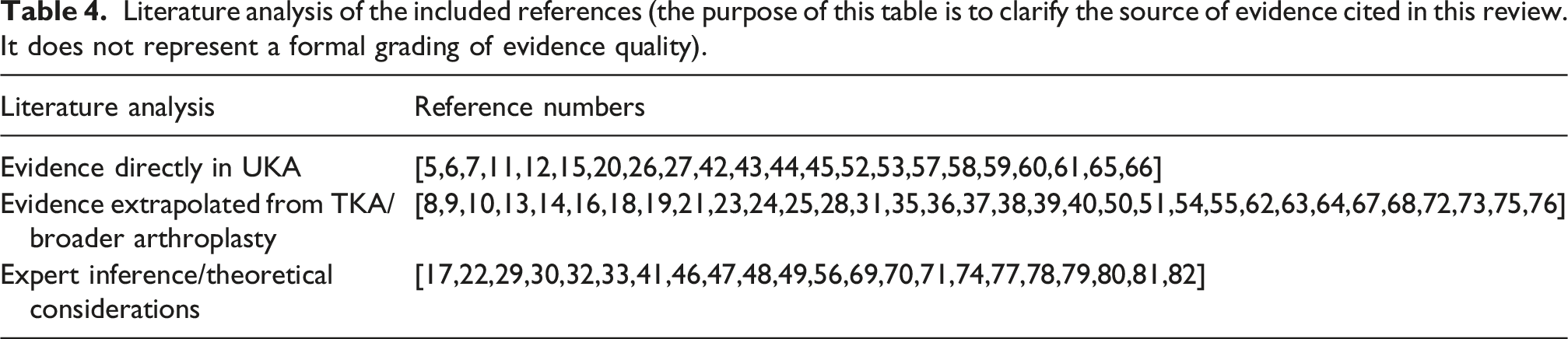
Literature analysis of the included references (the purpose of this table is to clarify the source of evidence cited in this review. It does not represent a formal grading of evidence quality).
Evidence directly in UKA
Evidence directly derived from UKA remains limited but informative. Several UKA-specific trials and cohort studies have reported that periarticular LIA using cocktail drugs is associated with reduced postoperative pain, decreased opioid consumption, and facilitated early functional recovery [11, 12, 52, 53, 65, 66, etc.]. Survey-based data also indicate that periarticular injection is widely adopted in UKA practice, reflecting its perceived clinical utility among experienced surgeons. 11 However, most UKA studies are single-center, involve relatively small sample sizes, and primarily focus on short-term outcomes. Therefore, its findings should be interpreted with caution.
Evidence extrapolated from TKA
Meanwhile, another portion of the pharmacological rationale and technical considerations for the use of cocktail drugs in UKA is extrapolated from studies conducted in TKA. Evidence from TKA consistently demonstrates that periarticular LIA can reduce postoperative pain, inflammatory response, and opioid requirements [9, 14, 19, 22, 39, 62, etc.]. Given the shared surgical field, innervation patterns, and periarticular anatomy, these findings provide a theoretical basis for application in UKA.
Expert inference
As the existing body of literature on UKA remains limited, leaving evidence gaps in certain areas, some of the proposed strategies inherently depend on expert inference. These include proposed modifications to injection sites, drug selection, and dosage adjustments to reflect the smaller surgical trauma and lower postoperative pain burden associated with UKA. Such inferences are supported by pharmacological principles, anatomical considerations, and accumulated clinical experience [30, 32, 47, 56, 68, 70, etc.], but they should not be interpreted as evidence-based recommendations. Further prospective UKA-focused studies are required to validate these assumptions.
Conclusion
Periarticular injection of cocktail drugs represents a commonly used component of multimodal analgesia in UKA. Available evidence indicates that there is no significant pharmacological incompatibility among the components of these formulations, which may contribute to postoperative pain control and early functional recovery in selected UKA patients. As an important part of the ERAS guidelines, it helps to reduce opioid consumption and facilitate early rehabilitation exercises for patients, as well as contribute to the personalized management of pain. Nevertheless, much of the supporting data is extrapolated from TKA, and high-quality UKA-specific evidence remains limited. In the specific clinical practice, it is still recommended to conduct careful and rigorous individualized assessment and decision-making. Conclusions regarding efficacy, safety, and optimal formulations should be interpreted with caution. Future large-scale, multicenter studies focusing specifically on UKA are required to establish evidence-based guidelines and to refine individualized analgesic strategies.
Footnotes
Acknowledgments
We would like to extend our sincere gratitude to the research team led by Professor Wu Jun from the Department of Orthopedics at People’s Hospital of Qianxinan Prefecture for their invaluable technical consultations.
Author contributions
Yuanhao Lv and Wanshun Liu contributed equally to this work. They conceived and designed the article, and then completed its writing.Jun Chen created the figures, Yu Huang assisted in the organization of references and the design of the tables. Xu Zhu revised the manuscript. Qingde Wa provided project support and manuscript review. All authors read and approved the final version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by The Zunyi City Science & Technology Innovation Talent Project (No. [2024] 04).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.