
Abstract
Introduction
Soft tissue tumors of the hand and digits are often small and clinically non-specific, leading surgeons to omit preoperative imaging. Magnetic resonance imaging is traditionally considered the reference standard for soft tissue tumors, but its role in the evaluation of small lesions in this anatomic region is not well defined. Ultrasound, as a readily available and cost-effective modality for superficial lesions, offers potential advantages. This study evaluates the diagnostic accuracy of preoperative ultrasound in soft tissue tumors of the hand and digits.
Materials and methods
A retrospective analysis was performed on patients who underwent surgical excision of soft tissue tumors of the hand in a tertiary referral center between January 1st, 2013, and December 31st, 2020. Demographic data, preoperative imaging reports, and histopathological diagnoses were collected. Histopathology served as the reference standard. Imaging data were re-analyzed per-modality by one radiologist blinded to the final diagnosis. Sensitivity, specificity, and overall accuracy of ultrasound and magnetic resonance imaging were calculated.
Results
A total of 194 patients were included. Most lesions were benign (91%, 177/194), whereas 8% (15/194) were intermediate and 1% (2/194) malignant. Predictors of intermediate/malignant histology included larger tumor size (p < 0.001), palmar location (p = 0.015), distal finger location (p = 0.022), and poorly defined borders on ultrasound (p = 0.022). Ultrasound demonstrated a sensitivity of 77.1%, specificity of 47.1%, and an overall accuracy of 74.5%. Magnetic resonance imaging showed a sensitivity of 45.7%, specificity of 83.3%, and an overall accuracy of 51.2%. In the subgroup of patients who underwent both ultrasound and MRI, agreement between modalities was moderate (weighted kappa = 0.529).
Conclusion
Ultrasound is an indispensable tool in the preoperative work-up of soft tissue tumors of the hand and digits. Given its sensitivity and overall accuracy, it should be considered the primary initial imaging modality, with magnetic resonance imaging reserved for cases with suspicious findings.
Introduction
Soft tissue tumors of the hand and/or digits present a diverse spectrum of cases. 1 Despite accounting for only 2% of the total body surface area, the hands are involved in approximately 15% of all soft tissue tumors.2,3 While the majority of these lesions is benign, 4 about 2% of soft tissue tumors of the hand and/or digits are malignant. 5 Due to their comparably small size and mostly non-specific appearance, clinical diagnosis may be difficult. 6 The superficial localization of these tumors may lead some surgeons to forgo a thorough preoperative evaluation. Nonetheless, an accurate preoperative assessment is crucial to ensure the optimal surgical approach given the close proximity of critical anatomical structures within the hand.
Ultrasound (US) is the primary method used for evaluating superficial lesions. 7 It assists in surgical planning by providing real-time functional testing and information about the tumor’s characteristics and topography. 8 Compared to magnetic resonance imaging (MRI), known advantages of US include its non-invasiveness, widespread accessibility, and cost-effectiveness. According to the European Society of Musculoskeletal Radiology (ESSR)-approved guidelines, MRI is recommended for lesions that appear potentially malignant on US. 9 To date, MRI is routinely preferred by clinicians for assessing musculoskeletal masses, yet its contribution in the management of small tumors of the hand and/or digits is not clearly defined and may be limited by technical restrictions in this anatomical region.10,11 In addition, the relative diagnostic performance and clinical utility of US compared to MRI in the preoperative evaluation of these tumors have not been distinctly established.
This study aims to investigate the accuracy of ultrasound in comparison with histopathology and its role relative to MRI in diagnosing and managing soft tissue tumors of the hand and digits.
Material & methods
Patients
A single-center, retrospective data analysis was conducted. Patients, who underwent surgical excision of soft tissue tumors found in the hand and/or digits at our department between January 1st, 2013, and December 31st, 2020, were included.
The area of the hand was defined as the area distal to the radiocarpal joint to exclude tumors of the wrist. Additionally, patients with recurring soft tissue tumors of the hand and/or digits were excluded to reduce examination bias. Finally, cases without preoperative US examination or postoperative histopathological work-up were excluded.
Retrospective medical chart review included: patient demographics (age, sex), clinical tumor localization (hand region, finger region, radial vs ulnar, and palmar vs dorsal), and final histopathological tumor size and diagnosis. Histopathological tumor diagnoses were classified as benign, intermediate, or malignant according to the 2020 WHO Classification of Soft Tissue Tumors and Bone. 12 Histopathological tumor diagnoses served as the reference standard.
Imaging data
All included patients (n = 194) had undergone preoperative ultrasound examination. Thereof, 46 patients (46/194, 41.4%) had undergone preoperative MRI. Patients varyingly presented prior to surgery with externally performed imaging or were referred to the Department of Radiology within our hospital. Due to the retrospectivity of this study and the heterogeneity in initial patient assessment (both outside and within the hospital), the clinical rationale for obtaining preoperative MRI could not be determined conclusively, yielding interobserver variability and the absence of a standardized MRI indication protocol. Suspected tumor diagnoses by US and by MRI were documented and classified as benign, intermediate, or malignant according to the 2020 WHO Classification of Soft Tissue Tumors and Bone. 12 To address interobserver variability, imaging data were re-analyzed per-modality by one radiologist blinded to the histopathological results and other modality’s findings. Ultrasound images were evaluated for tumor size, border definition (sharp, partially diffuse, or diffuse), echogenicity (hypoechoic, isoechoic, or hyperechoic compared to muscle), and Duplex vascularity (none [no vessels detected], moderate [sparse vascular content], or strong [high vascular content]). MRI images were evaluated for tumor size, border definition, T1-weighted (T1w) signal intensity, T2-weighted (T2w) signal intensity, Short-TI Inversion Recovery (STIR) signal intensity, overall contrast enhancement, contrast enhancement distribution, and diffusion restriction.
Statistics
Data are presented as mean (± standard deviation [SD]) where applicable or if not stated otherwise. Contingency tables were analyzed by χ2 test. p-values ≤0.05 were rated statistically significant.
Correlation between continuous variables was calculated via linear correlation analysis, results are given as slope, R2, and p-value. Classification performance of US and MRI were measured as sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and overall accuracy (OA), including 95% confidence intervals. Intertest agreement between US and MRI for the imaging classification as benign, intermediate, or malignant according to the 2020 WHO Classification of Soft Tissue Tumors and Bone 12 was calculated as weighted kappa. Results are given as kappa with 95% confidence intervals. Data for these calculations were dichotomized into benign versus non-benign, combining intermediate and malignant categories (intermediate/malignant). Additionally, a subgroup analysis of all patients who undewent US and MRI was performed to address potential selection bias for this subgroup.
A Bayes Network with a 100-fold cross-validation was used to determine covariate influence on tumor classification (benign vs intermediate/malignant). Model results include overall accuracy (OA), mean absolute error (MAE), relative absolute error (RAE), and weighted average for the true positive rate (TPavg), false positive rate (FPavg), and precision (Pavg). A gain-ratio feature evaluation with a gain-ratio merit-based ranker algorithm (WEKA, Waikato Environment for Knowledge analysis) was used to generate a covariate ranking. 13 For a full list of the included parameters, please refer to Supplemental Table 1. Results include rank, gain ratio merit (GRM), and standard errors of the mean (SEM).
Results
Patients
Between January 1st, 2013, and December 31st, 2020, 305 cases were identified in our database. Following data compilation, 111 cases (111/305, 36.4%) had to be excluded due to the following reasons: In 89 cases (89/305, 29.2%) preoperative US data and images were not available, in 16 cases (16/305, 5.2%) histopathological diagnosis was not documented, and in 6 cases (6/305, 2.0%) patients were presenting with a recurring tumor. The remaining 194 cases (n = 194) underwent surgical excision of a soft tissue tumor of the hand and/or digits after preoperative US evaluation and were included for final analysis. Average age at surgery was 48.6 (±19.2) years (median 49.5 years, range 5.3 to 93.3 years). Sex distribution was equal with 49.5% (96/194) female and 50.5% (98/194) male patients, respectively.
Tumor characteristics
Histopathological diagnoses of soft tissue lesions.
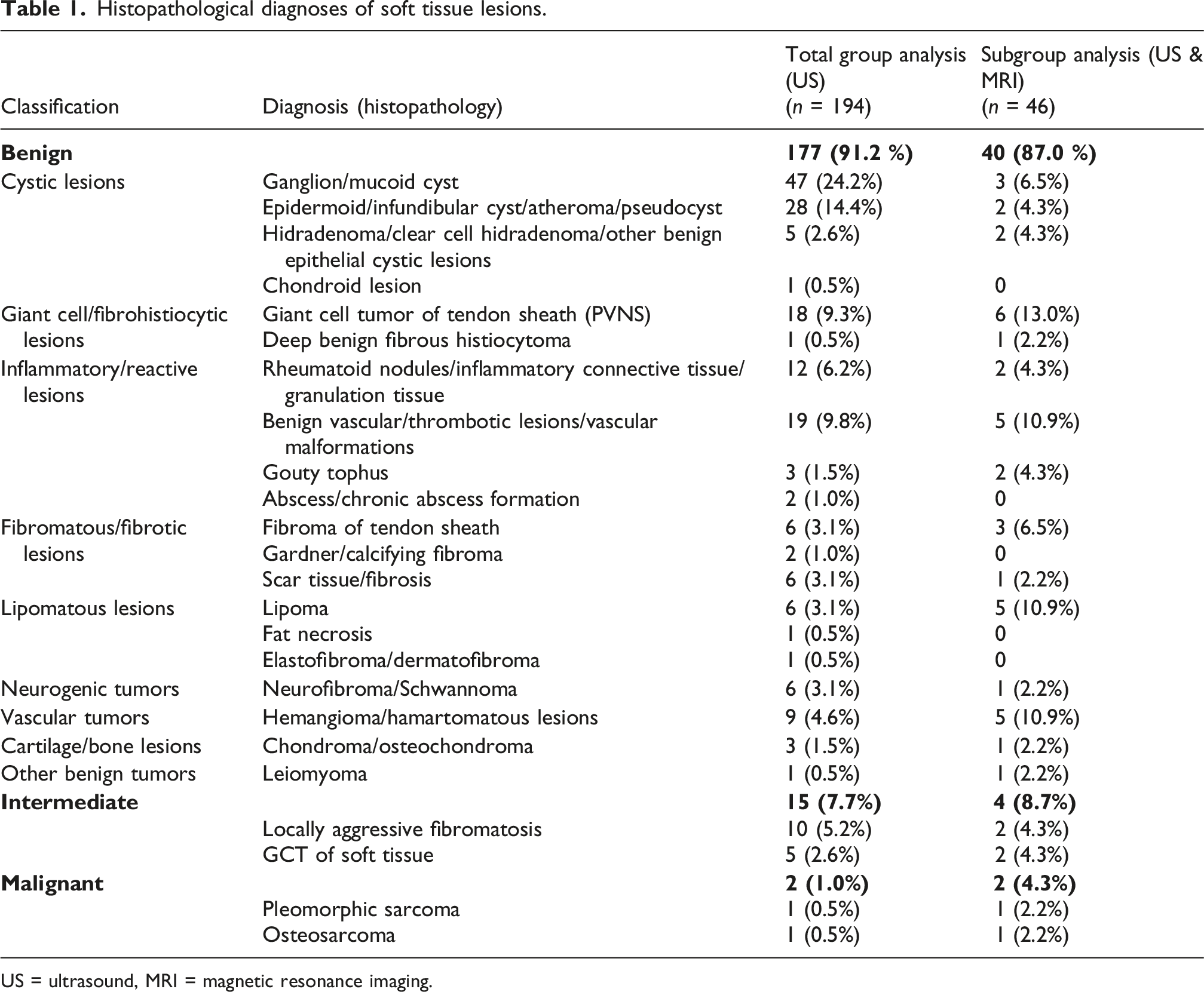
US = ultrasound, MRI = magnetic resonance imaging.
Regarding age distribution, most lesions presented between the age of 50 and 60 years with incidence peaks for intermediate/malignant tumors in children (<10 years) and in the elderly (>70 years) (see Supplemental Figure 1).
The average tumor size measured by histopathology after tumor resection was 14.1 (±12.1) mm (median 10.0 mm, range 3–90 mm) with the majority of lesions smaller than 20 mm and the malignant tumors measuring >30 mm in size. Tumor size showed a significant difference regarding benign versus intermediate/malignant tumor classification (p = 0.001, Figure 1(a)). Tumor classification grouped by tumor size (a) and rate of tumor proximity to functional structures according to ultrasound documentation (b).
In 56 cases (56/194, 28.9%), US documentation suggested tumor proximity to and/or involvement of functional structures such as nerves, vessels, or ligaments, which could lead to complications or surgical difficulty. The rate of preoperative diagnosis of tumor proximity to functional structures did not differ depending on tumor classification (p = 0.647, Figure 1(b)).
Tumor localization
Most tumors were localized at the digits (136/194, 70.1%), followed by the metacarpal region (39/194, 20.1%). Overall, tumor distribution regarding the hand region differed significantly by benign versus intermediate/malignant tumor classification (p = 0.001, Figure 2(a)). In affected digits, most intermediate/malignant lesions occurred at the middle or distal phalanx or the distal interphalangeal joint (p = 0.022, Figure 2(b)). Radial or ulnar localization did not correlate with the tumor classification (p = 0.571, Figure 2(c)), while palmar localization was significantly associated with an intermediate/malignant tumor classification (p = 0.015, Figure 2(d)). Tumor classification grouped by hand region (a), finger region (b), radial or ulnar localization (c), and palmar or dorsal localization (d).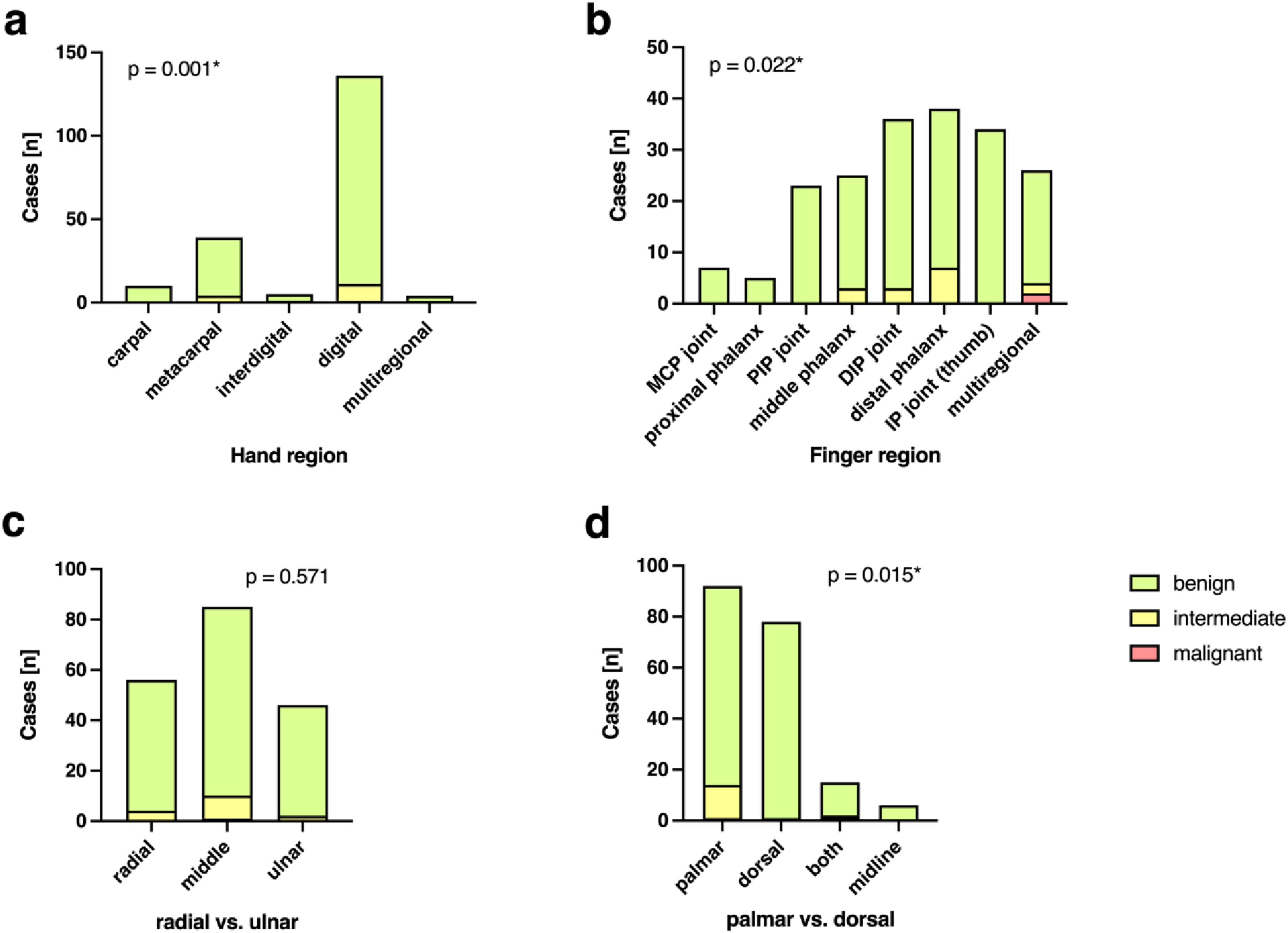
Imaging findings
Ultrasound examinations revealed a significant difference in the occurrence rate of (partially) diffuse border definition with intermediate/malignant lesions all having at least a partially diffuse border definition (p = 0.022, Figure 3(a)). Echogenicity (p = 0.191, Figure 3(b)) and Duplex vascularity (p = 0.482, Figure 3(c)) did not differ significantly depending on tumor classification. Tumor classification grouped by ultrasound findings: border definition (a), echogenicity (b), and vascularity (c).
No significant difference in border definition of benign versus intermediate/malignant lesions could be observed on MRI (p = 0.068, Figure 4(a)). T1w SI (p = 0.829, Figure 4(b)), T2w SI (p = 0.453, Figure 4(c)), STIR SI (p = 0.208, Figure 4(d)), presence of contrast enhancement (p = 0.775, Figure 4(e)), contrast enhancement distribution (p = 0.635, Figure 4(f)), and diffusion restriction (p = 0.551, Figure 4(g)) showed no significant difference by tumor classification. Tumor classification by MRI findings: border definition (a), T1-weighted (T1w) signal intensity (SI) (b), T2-weighted (T2w) signal intensity (SI) (c), Short-TI Inversion Recovery (STIR) signal intensity (SI) (d), overall contrast enhancement (e), contrast enhancement distribution (f), diffusion restriction (g).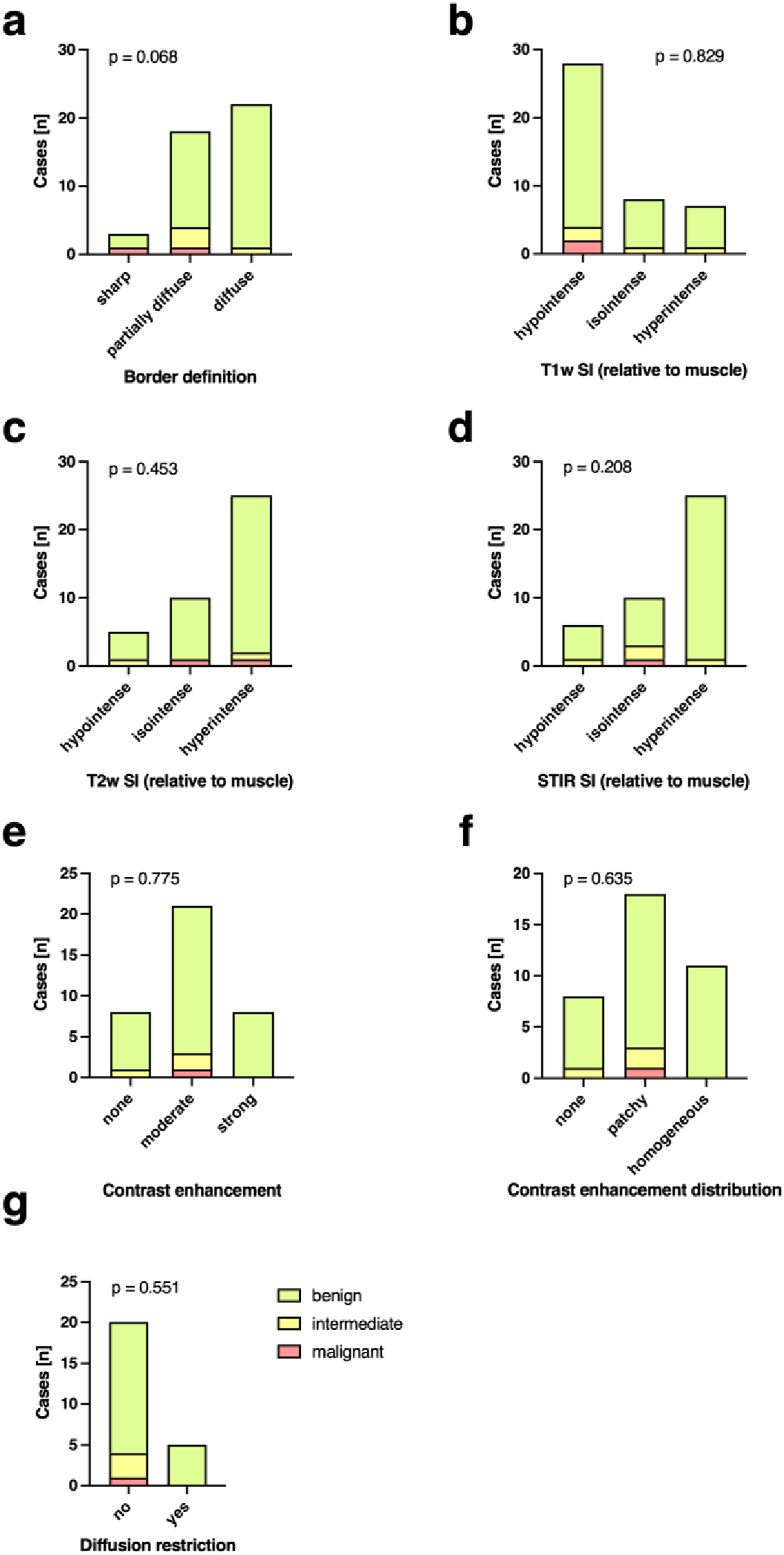
Diagnostic accuracy of ultrasound and MRI
Forty-six cases had undergone both US and MRI (46/194, 23.7%). A clinical example is depicted in Figure 5. Soft tissue tumor found in the palm of the hand: Clinical appearance (a), intraoperative appearance (b), MRI appearance incorrectly classified as a schwannoma (c) and US appearance correctly classified as a tumor of vascular origin (d).
For detection of intermediate/malignant tumor classification, US exhibited a sensitivity of 77.1% (95% CI: 70.0% to 82.7 %), a specificity of 47.1% (95% CI: 26.2% to 69.0%), a PPV of 93.8% (95% CI: 88.6% to 96.7%), and a NPV of 16.7% (95% CI: 8.7% to 29.6%) at an OA of 74.5%. MRI exhibited a sensitivity of 45.7% (95% CI: 30.5% to 61.8%), a specificity of 83.3% (95% CI: 43.7% to 99.2%), a PPV of 94.1% (95% CI: 73.0% to 99.7%), and a NPV of 20.8% (95% CI: 9.2% to 40.5%) at an OA of 51.2% (Figure 6). Imaging findings on sensitivity (a), specificity (b), and overall accuracy (c) grouped by imaging modality: ultrasound (US) versus magnetic resonance imaging (MRI).
Subgroup analysis
In a subgroup analysis of all patients who underwent both US and MRI (n = 46; average age 43.9 ± 20.7 years, 45.7% female), 40 lesions (40/46, 87.0%) were of benign, four lesions (4/46, 8.7%) were of intermediate and two lesions (2/46, 4.3%) of malignant differentiation. All diagnoses are listed in Table 1.
Diagnostic parameters of ultrasound and MRI after subgroup analysis.

Covariate analysis
The Bayes network covariate analysis of the covariate influence on tumor classification yielded 90.2% OA, 0.14% MAE, 84.7% RAE, and 90.2% TPavg, 80.7% FPavg, and 86.9% Pavg. Supplemental Table 1 provides an overview of the ranked covariates according to gain ratio merit (GRM) with palmar localization (average GRM 0.035 ± 0.005), US-based classification estimation (0.03 ± 0.005), and US-based estimation of tissue of origin (0.012 ± 0.001) exhibiting the greatest influence on the presence of an intermediate/malignant lesion, while patient age and tumor dimensions did not yield any gain ratio merit (GRM 0.0 ± 0.0, respectively). While T1w and T2w signal intensities alone did not confer information (0.0 ± 0.0), only diffusion-weighted imaging showed some discriminatory contribution (GRM 0.001 ± 0.0).
Discussion
The superficial localization and relatively small size of tumors found in the hand and/or digits often entice surgeons to forgo thorough preoperative diagnostics. To mitigate severe complications or local recurrence in cases of malignancy, preoperative evaluation supported by imaging should be routinely employed. 9 However, our data showed that in 89 out of 305 cases (29.2%), surgeons did not arrange a preoperative ultrasound (US) examination.
In the 194 cases included in this study, the likelihood of benignancy was confirmed at 91.2%. 4 Only two out of 194 tumors (1.0%) were diagnosed as malignant by histopathology, underlining the rarity of malignancy in the hand. While the main incidence peak of soft tissue tumors of the hand and digits was observed in individuals aged 50–60 years, both malignant diagnoses correlated with known age-related incidences.14,15 One 72-year-old woman was diagnosed with pleomorphic sarcoma, which typically occurs in patients over the age of 50, and one 8-year-old boy was diagnosed with osteosarcoma, the most common primary bone malignancy in children.14–16
Although malignant subtypes are rare, the possibility of malignancy should not be disregarded, as soft tissue sarcomas can mimic benign entities in certain cases. 17 As described in our study, even osteosarcoma may present as a soft tissue tumor in clinical appearance. During preoperative evaluation, surrogate parameters are often key in distinguishing between benign and malignant lesions. 18 For instance, tumor size and localization may indicate a higher risk for intermediate or malignant growth.6,19 In this study, tumors of intermediate classification were significantly larger, at least 10 mm, while both malignant tumors were over 30 mm. Large tumor size and rapid tumor growth are known characteristics for malignant differentiation.6,20 Additionally, the multiregional localization of malignant tumors in this study may again be attributed to the large tumor size. Furthermore, palmar localization was significantly associated with intermediate/malignant tumor classification explained by the palm’s tissue composition giving rise to soft tissue giant cell tumors or aggressive fibromatosis. 12
Important surrogate parameters may also be defined by preoperative imaging. This study found statistical significance for the presence of diffuse tumor borders on US, while echogenicity and Duplex vascularity did not differ significantly for tumor classification. In comparison, MRI only showed a trend toward diffuse borders in intermediate and malignant lesions. Apart from surrogate parameters such as tumor size and localization, border definition and vascularity are important tumor characteristics and may suggest intermediate or malignant differentiation.21,22 While US easily and reliably visualizes tumor vascularization, 23 US contrast application plays a rather confined role compared to MRI. Technical difficulties regarding specific sound frequencies in the field of the hand and digits and further developments in Duplex methods diminish its necessity. However, contrast enhancement provides further phenotypic information assumably equivalent to MR contrast imaging. 24 In this study, MRI evaluation regarding contrast enhancement, contrast enhancement distribution, and diffusion restriction showed no significant difference between tumor classifications.
While MRI is still considered the gold standard for soft tissue imaging, we observed that in this cohort, where MRI was selectively applied, the imaging sensitivity and the overall accuracy for MRI was lower than that for universally applied US and within our subgroup analysis. This may be attributed to a superior US resolution, outweighing MRI’s low signal yield and susceptibility to field heterogeneity encountered around small peripheral structures surrounded by air (e.g. the fingers). 25 Similar findings supporting US for small, peripheral lesions have been described in several case series.9,26 For instance, Lakkaraju et al. found US efficient in triaging soft tissue masses when sarcoma was suspected. 26 Furthermore, high-resolution sonography utilizing transducers in the range of 15 MHz and above has proven to show accuracy in the evaluation of superficial soft tissue tumors and the differentiation between benign and malignant phenotypes. 27 As one of the highest ranked covariates in this study, US-based definition of topography and tissue of origin showed a significant influence on the presence of intermediate/malignant tumors.
However, the higher sensitivity of US was accompanied by lower specificity compared to MRI, indicating a higher rate of false-positive classifications. While this may result in overestimation of malignancy in some benign lesions, it supports the role of US as a sensitive triage tool. According to the current Guidelines of the European Society of Musculoskeletal Radiology (ESSR) on soft tissue tumor evaluation in adults, US is recommended as the initial triage imaging method if the mass is accessible by ultrasound. MRI is recommended for further evaluation as the modality with the best contrast for soft tissue. 9 In cases with suspicious findings on US, subsequent MRI can leverage its higher specificity to refine lesion characterization and guide clinical decision-making. The moderate agreement between US and MRI found in the subgroup analysis (weighted kappa = 0.529) further supports that US demonstrates a reasonable level of consistency with MRI, but that discrepancies remain and the two modalities are not fully interchangeable in the preoperative evaluation of small soft tissue tumors. Therefore, we believe that US as a triage tool improves the appropriateness of subsequent MRI referrals. Although US has lower specificity than direct MRI, its use may help enable initial lesion stratification and identification of clearly benign findings. Consequently, this can reduce unnecessary, invasive and costly MRI examinations of simple benign lesions.
Limitations of this study include its single-center experience and retrospective study design. First and foremost, a considerable number of cases had to be excluded due to missing preoperative imaging and MRI images were only available in a limited number of cases. As a result, we had to accept an unfavorable sample size imbalance when comparing US to MRI and a potential selection bias regarding the cases with MRI. To reduce this limitation, we performed a subgroup analysis of all cases with MRI, which did not confirm selection bias on the grounds of tumor characteristics. However, the small sample size of cases undergone US and MRI imaging may explain the inferiority of MRI compared to US in this study. At the same time, the superiority of US may be attributed to a high pretest probability that soft tissue tumors of the hand and/or digits are benign, while the retrospective study design limited the possibility of incorporating real-time information during US examination. Additionally, the retrospective design resulted in heterogeneous imaging protocols and potential variability in US operator skills, both of which should be acknowledged as limitations. To strengthen our study design and step into the direction of standardizing ultrasound diagnostics, re-analysis of ultrasound findings was performed by protocol by one blinded radiologist. Overall, one might argue that the predominance of benign tumors affected the assessment of preoperative imaging’s utility in determining tumor classification. This also factors into the statistical analysis, as an imbalance in frequencies (i.e. a high prevalence for benign lesions and low prevalence of malignant lesions) can decrease the results’ reliability. 28 To truly challenge MRI’s gold standard status in soft tissue imaging, follow-up studies with reduced examination bias and standardized protocols are highly warranted. However, we believe that a standardized multiparametric US examination may be able to raise the standard of quality in preoperative tumor evaluation and improve indication for MRI referral.
Conclusion
In conclusion, US is an indispensable tool in the preoperative work-up of soft tissue tumors of the hand and/or digits. In this retrospective study, ultrasound demonstrated a high sensitivity and overall accuracy in the detection of soft tissue tumors of the hand and/or digits and may be considered sufficient as preoperative imaging in certain cases. We propose US as the primary initial imaging modality in the preoperative evaluation of small soft tissue tumor of the hand and/or digits with MRI remaining a vital addition in cases with suspicious or equivocal US findings. However, prospective validation of these findings is warranted.
Supplemental material
Supplemental material - Soft tissue tumors of the hand and digits - The role of preoperative ultrasound compared to MRI
Supplemental material for Soft tissue tumors of the hand and digits - The role of preoperative ultrasound compared to MRI by Tina Deutinger, Hannes Gruber, Turkhan Mehdiyev, Leonhard Gruber, Yannick Scharll, Caroline Bauer and Robert Zimmermann in Journal of Orthopaedic Surgery
Supplemental material
Supplemental material - Soft tissue tumors of the hand and digits - The role of preoperative ultrasound compared to MRI
Supplemental material for Soft tissue tumors of the hand and digits - The role of preoperative ultrasound compared to MRI by Tina Deutinger, Hannes Gruber, Turkhan Mehdiyev, Leonhard Gruber, Yannick Scharll, Caroline Bauer and Robert Zimmermann in Journal of Orthopaedic Surgery
Footnotes
Acknowledgements
We sincerely thank K. Langert for the photography. Further, we sincerely thank A. Loizides and G. Pierer for their scientific and clinical support.
Ethical considerations
Ethical Approval was obtained from the institutional ethical review board (EK number: 1051/2020).
Consent to participate
All patients gave their written informed consent for publication of their photographs.
Author contributions
T.D. manuscript writing, figure preparation, data acquisition. H.G. investigation, visualization, manuscript writing, data interpretation, validation. L.G. manuscript editing, figure preparation, statistical analysis. T.M. data acquisition, manuscript revision, visualization. Y.S. data interpretation, data curation. C.B. data acquisition, visualization. R.Z. conceptualization, supervision, manuscript editing, data interpretation.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.