
Abstract
Background
Anterior cruciate ligament reconstruction (ACLR) is a critical surgical intervention for NBA players. While return-to-play (RTP) rates are documented to be high, the long-term impact of ACLR on specific performance metrics and on-court play style remains poorly understood.
Questions/Purposes
The purpose of this study was to (1) evaluate changes in performance and play style in NBA players post-ACLR compared to matched controls and (2) determine if durability or skill loss is the primary limiting factor following surgery.
Methods
This matched case-control study analyzed 38 NBA players who underwent ACLR between 2000 and 2022. Cases were matched 1:2 with 76 control players based on position, experience, and pre-injury performance. Metrics analyzed included minutes per game (MPG), usage rate (USG%), shooting distribution, and optical tracking data.
Results
Post-ACLR players exhibited significant declines in MPG, USG%, and dunk attempt frequency (p < .05) compared to controls, suggesting a reduction in physical explosiveness and offensive involvement. Conversely, no significant differences were observed in average shot distance, shooting distribution, or player tracking data. Notably, players who reached minimum post-surgery participation thresholds maintained pre-injury performance levels relative to controls.
Conclusion
ACLR in NBA players is associated with a reduction in offensive workload and explosiveness; however, skill-based performance remains preserved in those who successfully return to sustained competition. These findings suggest that durability—rather than skill loss—is the primary challenge. Rehabilitation should emphasize workload management and neuromuscular conditioning to optimize career sustainability.
Introduction
Anterior cruciate ligament (ACL) injuries are a major concern in sports medicine, especially among elite athletes, where ligament tears frequently cause season-ending disruptions in athletic careers. The overall incidence of ACL tears among NBA players is estimated to be around 2.7%, with the majority requiring surgical intervention via ACL reconstruction (ACLR) to regain knee function and stability.1–3 After surgery, athletes usually need a significant amount of rest and rehabilitation before returning to professional play.
According to previous research, NBA players have a high return-to-play (RTP) rate following ACLR, ranging from 81 to 95%.4–8 However, performance metrics in the first post-reconstruction year (PRY1) frequently reveal deficits, with players playing an average of 17 fewer games than they did prior to injury. 7 Although several studies have found declines in metrics such as player efficiency ratings (PER) and raised concerns about players’ ability to return to pre-injury performance,4,9,10 a recent meta-analysis found no significant performance deterioration when comparing ACL-reconstructed athletes to non-injured controls. 11
In parallel with performance considerations, understanding play style adaptations following ACL injury has become increasingly relevant. In basketball analytics, “play style” generally refers to an athlete’s characteristic pattern of offensive decision-making and on-court behavior, encompassing factors such as shot distribution, rim-attacking frequency, drive involvement, and ball-handling engagement. These elements reflect both physical capacity and the tactical role assigned within team systems. Despite growing interest, few studies have explicitly examined play style changes after ACLR through a clearly defined conceptual framework. 12
Mechanistically, prior biomechanical research has established that noncontact ACL injuries frequently occur during high-risk actions such as deceleration, landing, and initial steps following ball pickup.13–17 These movements are central components of aggressive rim attacks and drive-based offensive styles in the NBA. Consequently, ACL injury mechanisms may have direct implications for the types of movements players avoid or modify after surgery, eventually causing the change of play type.
Given this context, the present study aims to evaluate changes in performance metrics and play style among NBA athletes following ACLR using a matched case–control design. We hypothesized that postoperative reductions in athletic explosiveness and durability would manifest as diminished frequency of high-impact actions such as drives, layups, and dunks, alongside decreased playing time and usage rate. Similarly, we anticipated a compensatory shift toward perimeter-oriented shot selection—such as mid-range and three-point attempts—which require less vertical explosiveness and impose lower mechanical demands on the reconstructed knee.
Materials and methods
Study cohort
NBA players who had anterior cruciate ligament (ACL) tears and later had ACL reconstruction surgery between January 1, 2000, and December 31, 2022, were included in this retrospective case-control study. Those who had their ACL injury before 2000 or after 2022 were excluded because of a lack of comprehensive performance data. We collected the players’ injury and surgery information from NBA official documentation. This study looked at a four-year period surrounding the injury, referring to the season prior to the injury as the “Index Year” and the injury season as the “Injury Year.” “PRY1” and “PRY2” (Post-Reconstruction Years) were the names given respectively to the first and second season after players returned to the NBA court postoperatively. Furthermore, we defined “pre-surgery period” as the combination of “Index year” and “injury year,” and “post-surgery period” as the combination of “PRY1” and “PRY2”.
To provide sufficient data, our study included only players who played at least 58 games during both the “Pre-surgery period” and the “Post-surgery period. The 58-game limitation is based on the NBA’s “Statistical Minimums to Qualify for NBA League Leaders,” which stipulates that a player must participate in at least 70% of their team’s games, equivalent to 58 games in an 82-game season, to be eligible for statistical leaderboards. 18 This threshold enhances stability of statistical estimates, however it may exclude players with shortened careers or significant postoperative decline, which may bias results toward players with better recovery trajectories. Finally, players who experienced another major injury before returning from surgery were excluded from the study.
Control group
A 1:2 matched control group was formed, composed of NBA players with no history of ACL injury or reconstruction (ACLR). We sourced our control group players from the CraftedNBA website. This platform examines players based on on-court position, height and weight, traditional and advanced analytics, efficiency measures, and offensive and defensive roles to provide a “Similarity Score” in comparison to the experimental group. 19 Although the Similarity Score metric has not been formally validated in peer-reviewed settings, it provides a pragmatic approach for identifying comparable control players based on multidimensional player characteristics.
Control players should adhere to these criteria: (1) Their age differed from that of the experimental players by no more than 1 year during the index season, and (2) their index season happened one season before or after the experimental group’s. This approach helped control for age-related decline and seasonal changes in play style in NBA teams. After determining the control group’s index year, we looked at the following four seasons (including the index year), dividing them into “Pre-surgery period” and “Post-surgery period” (two seasons each) and compared them to the experimental group player. Both periods need at least 58 games to assure data reliability.
Data curation
We obtained demographic and anthropometric information about players from the NBA’s official website (NBA.com), such as their height (in feet and inches), weight (in pounds), and playing position. In addition, information about their injury and surgery was documented, such as the injury season, NBA experience at the time of injury, age at surgery, dates of injury and surgery, games played in the “Pre-surgery period” and “Post-surgery period,” and time (in months) spent returning to play on NBA courts.
Data on player performance were obtained from both NBA.com and Basketball-reference.com. We primarily focused on four aspects of performance measures linked to diminishing explosiveness and player loading: (1) Usage percentage (USG%) and minutes per game (MPG); (2) average shot distance (Avg Dist); (3) frequency percentage (Freq%) and field goal percentage (FG%) of shot area, including restricted area (RA), non-RA paint, mid-range, and three-point line; (4) frequency percentage (Freq%) and field goal percentage (FG%) of shot types, such as dunks, layups, and jump shots. (5) Tracking statistics, such as distance traveled per game, average speed on court, frequency percentage (Freq%), and field goal percentage (FG%) of drives. The fifth category only started collecting data after the 2013-14 season, resulting in small sample sizes. Consequently, these tracking metrics were analyzed separately from the primary performance categories (1-4) to appropriately account for this data limitation. Detailed definitions of basketball-specific terminology and performance metrics are provided in the Supplemental Material.
Statistical analysis
Baseline demographic and anthropometric characteristics (e.g., age, height, weight, NBA experience) between the ACLR group and the control group were compared using independent-samples t-tests for continuous variables and chi-square tests for categorical variables (e.g., playing position). To evaluate changes in performance metrics over time and between groups, 2-tailed paired t tests were performed to evaluate players against themselves across different periods of time. When comparing all ACLR cases to control group players, independent-samples t-tests were used. Additionally, player tracking performance metrics—including travel distance, travel speed, driving rate, and driving field goal percentage—were analyzed using Wilcoxon signed-rank tests to compare pre- and post-surgery performance within the ACLR group. To compare these same metrics between ACLR cases and control group players, Mann-Whitney U tests were performed.
Due to the small sample size for player tracking data (available post-2013-14 season) and their non-normal distribution, these specific metrics (e.g., travel distance, average speed, drive frequency) were analyzed using non-parametric tests. A Wilcoxon signed-rank test was used for within-group (pre-vs post-surgery) comparisons in the ACLR group. A Mann-Whitney U test was used for between-group comparisons of these tracking metrics.
To manage the risk of Type I errors from multiple comparisons, we prespecified three primary outcomes based on our core hypotheses regarding durability and explosiveness: MPG, USG%, and dunk attempt frequency. These primary outcomes were tested for significance without adjustment (p = .05). All other performance metrics (e.g., shot distribution frequencies, other shot types) were classified as secondary, exploratory outcomes. To control the family-wise error rate for these secondary analyses, a Bonferroni correction was applied. The adjusted significance threshold was set at p = 0.05/k, where k represents the number of comparisons within that specific variable family (e.g., k = 4 for the shot area frequencies). All statistical analyses were conducted using IBM SPSS Statistics (Version 30.0.0.0).
Result
Baseline player characteristics
Between 2000 and 2022, 73 NBA players were identified as having sustained an ACL tear requiring reconstruction. After applying the inclusion requirement of at least 58 games played in both the pre- and post-injury periods, 38 players remained eligible for analysis Figure 1. The 38 players in the ACLR group had a mean age at injury year of 24.76 ± 3.50 years, with 4.87 ± 2.81 seasons of NBA experience. Mean height and weight were 200.59 ± 8.21 cm (6 ft 7.0inches ±3.23 inches) and 219.66 ± 27.51 pounds, respectively. There was no significant predilection for injury side (left: 44.7%, n = 17) or limb dominance (dominant side: 47.4%, n = 18), showing a balanced distribution across the cohort. Furthermore, the positional breakdown included 36.8% forwards (n = 14), 44.7% guards (n = 17), and 18.4% centers (n = 7). Flow diagram of exclusion players: Of the 73 NBA players who tore their ACL and underwent ACL reconstruction (ACLR) during this period, 30 players were excluded due to insufficient game appearances in the post-surgery period. Additionally, 5 players, including 3 who sustained their injuries during their rookie year, were excluded due to insufficient performance data for the pre-surgery period.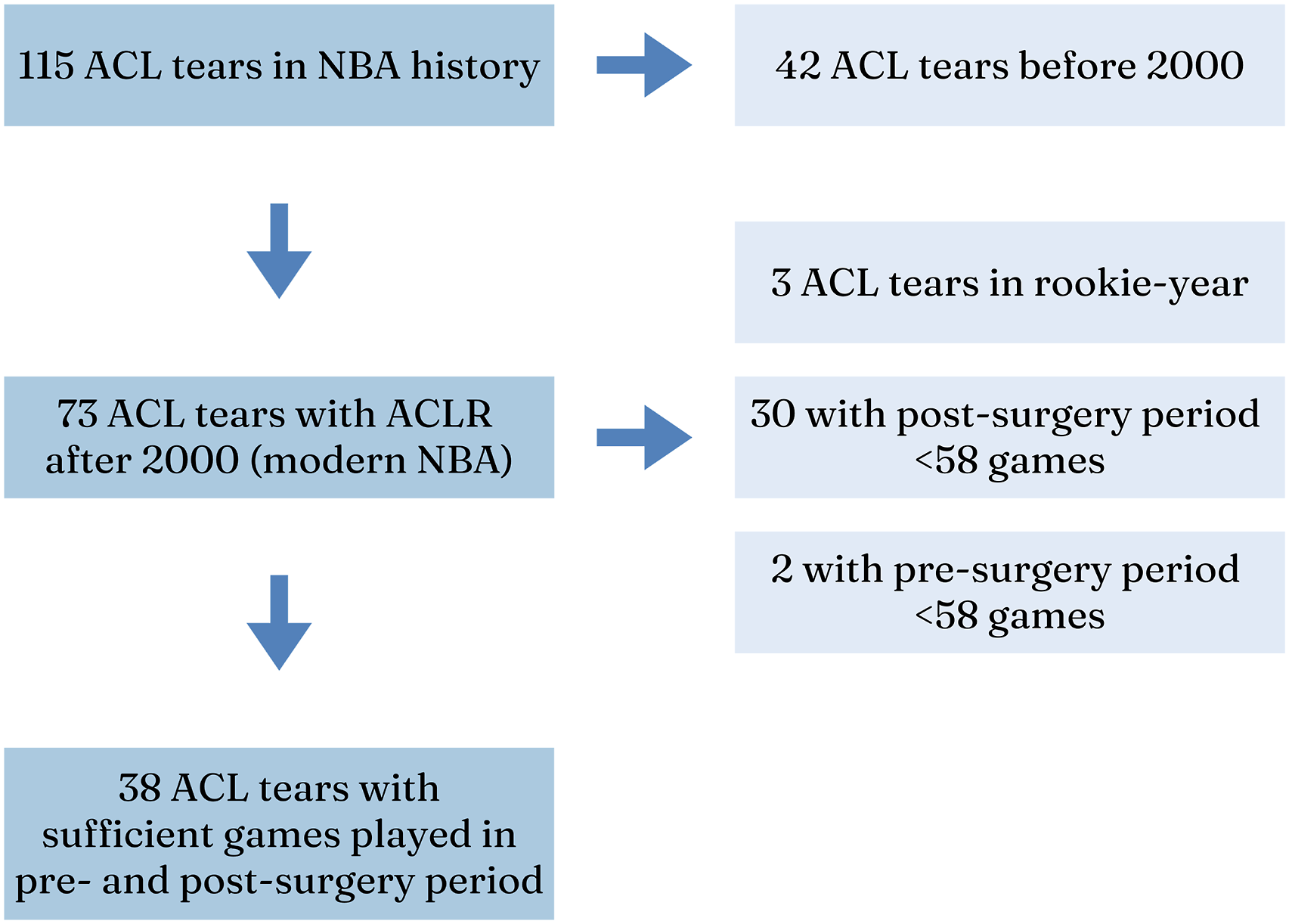
Demographic data.
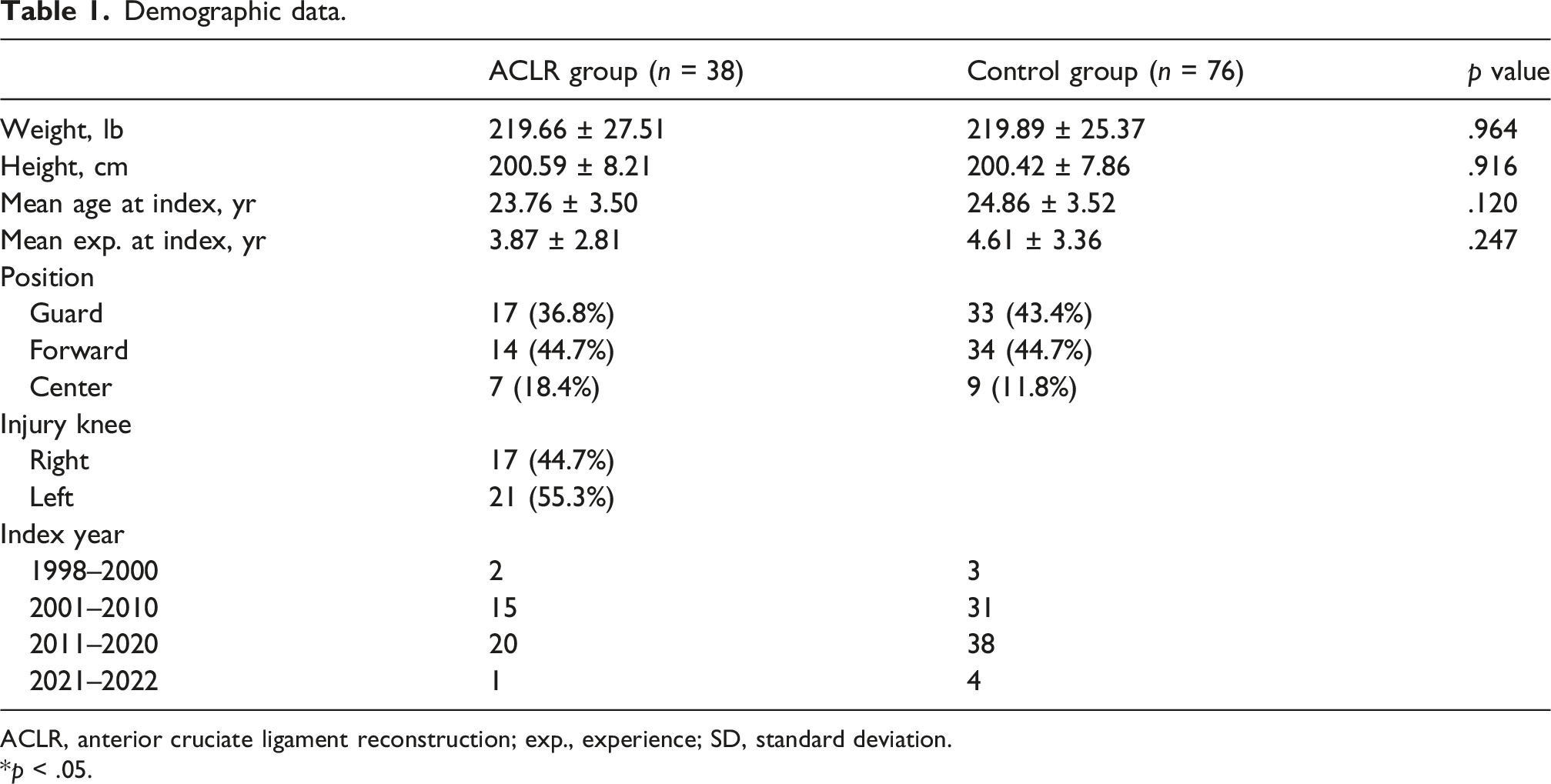
ACLR, anterior cruciate ligament reconstruction; exp., experience; SD, standard deviation.
*p < .05.
Performance analytics
We examined the performance metrics of NBA players who underwent anterior cruciate ligament reconstruction (ACLR) by comparing pre-surgery and post-surgery data across usage, minutes, attempting frequency and field goal percentages of various shot ranges or shot types. And moreover, we compare the players’ performance difference of pre- and post-surgery between ACLR group and control group, which could be seen more understandable in Figures 3 and 4.
Primary performance outcome: Minutes per game (MPG), usage, Dunk frequency
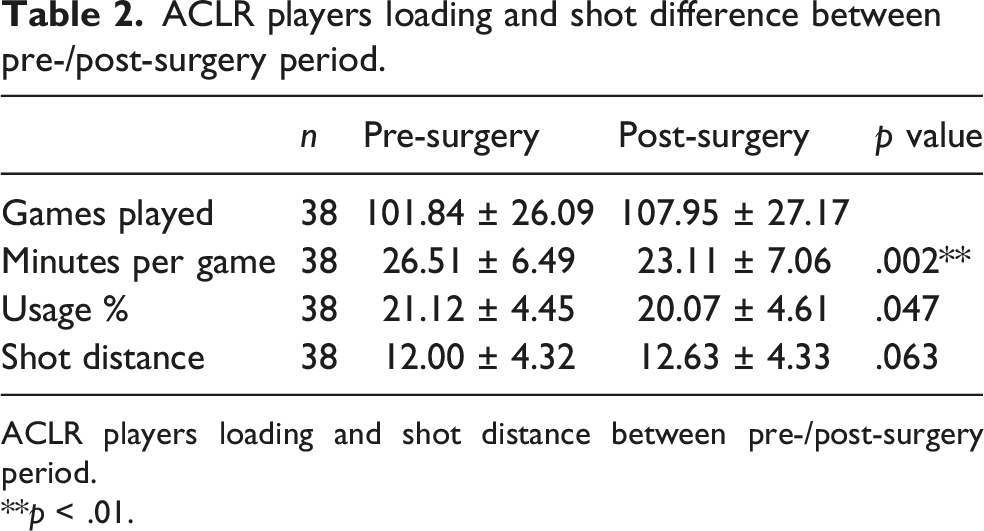
A significant reduction in minutes per game (MPG) was observed following ACL reconstruction, decreasing from 26.51 ± 6.49 to 23.11 ± 7.06 (p = .002; Figure 2). This decrease (−3.40 ± 6.35) was larger than the change observed in controls (−0.74 ± 5.45, p = .022). Usage rate (USG%) decreased modestly from 21.12 ± 4.45% to 20.07 ± 4.61%, though the between-group comparison did not reach statistical significance (p = .149). Results are presented in Table 2. Dunk attempt frequency decreased significantly after ACL reconstruction (p = .046) but did not differ from the control group (p = .184). MPG (minutes per game) Difference of ACLR group players between pre-/post-surgery period: After surgery, MPG of ACLR players dropped dramatically from 26.51 ± 6.49 to 23.11 ± 7.06 (p = .002). **, p < .01. ACLR players loading and shot difference between pre-/post-surgery period. ACLR players loading and shot distance between pre-/post-surgery period. **p < .01.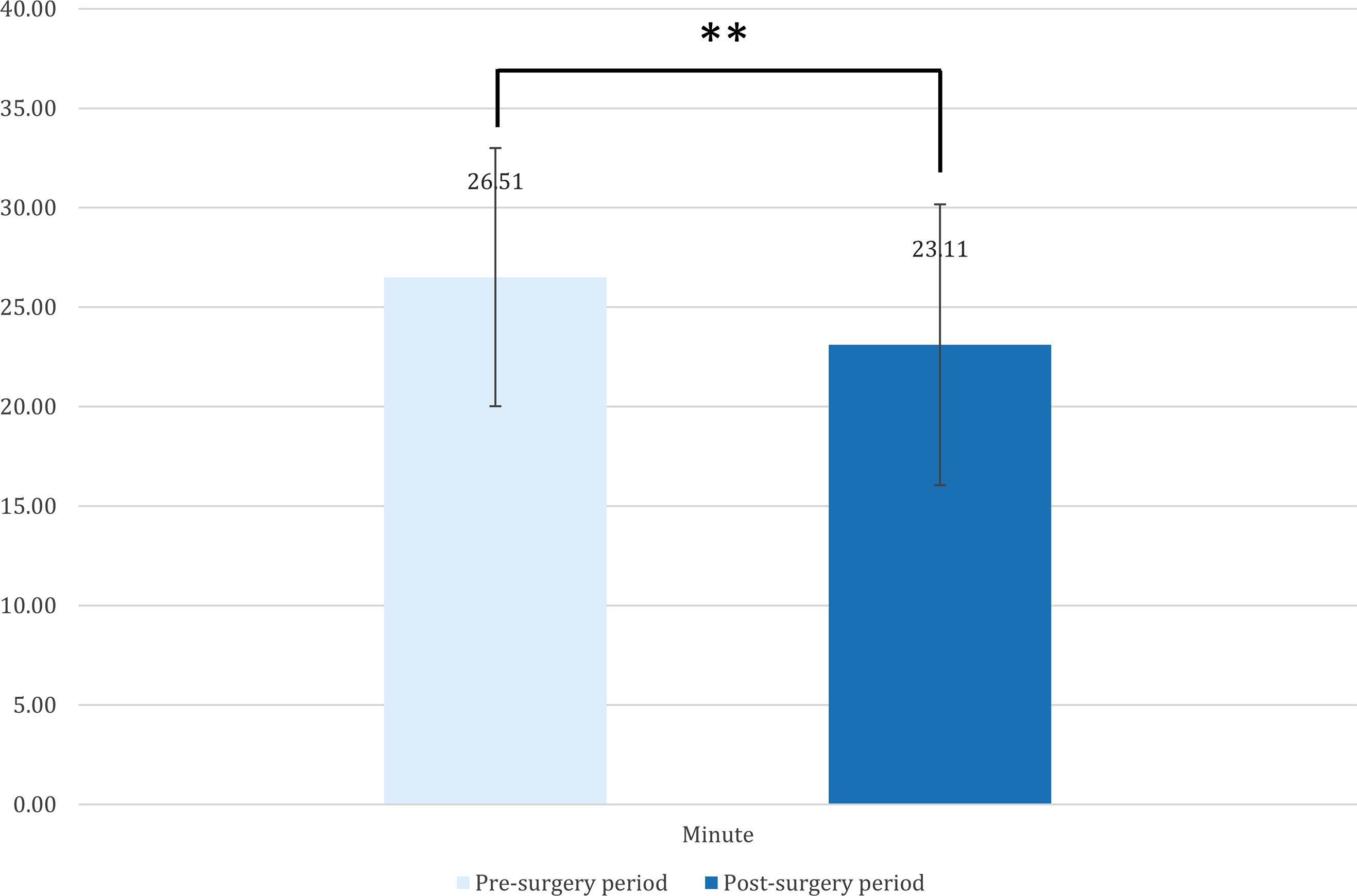
Shot selection: shot distance, shot distribution, and shot type
ACLR players shot frequency difference between pre-/post-surgery period.
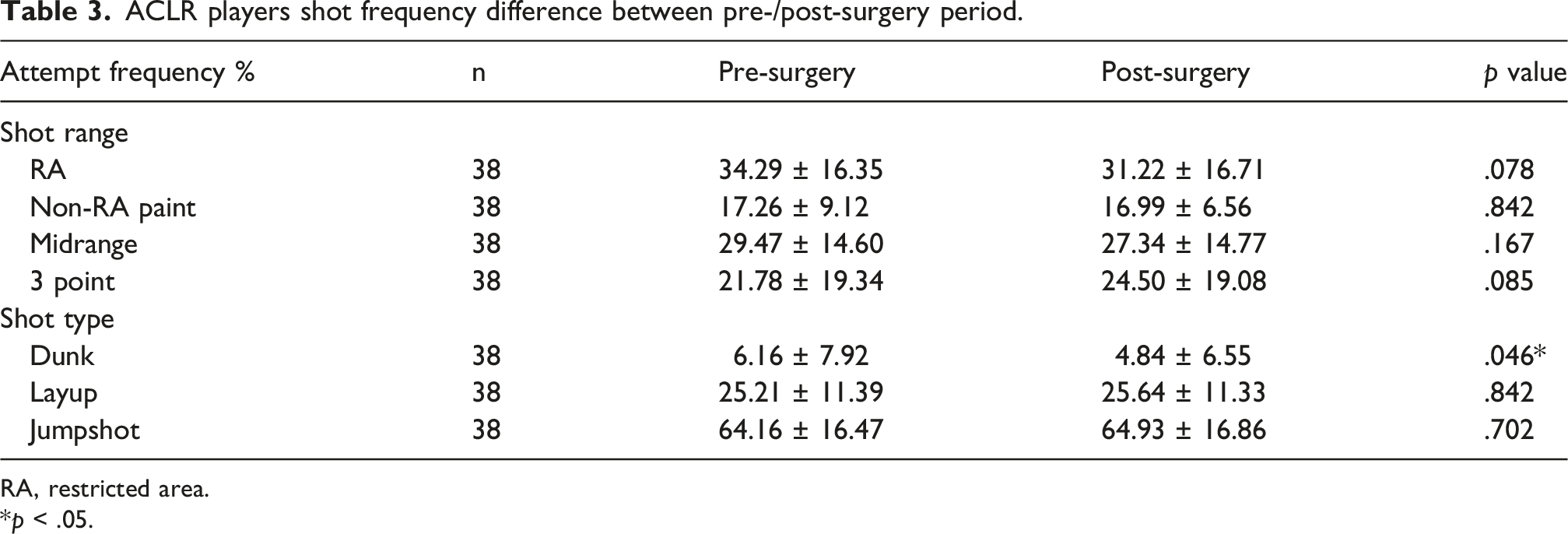
RA, restricted area.
*p < .05.
ACLR players shot efficiency difference between pre-/post-surgery period.
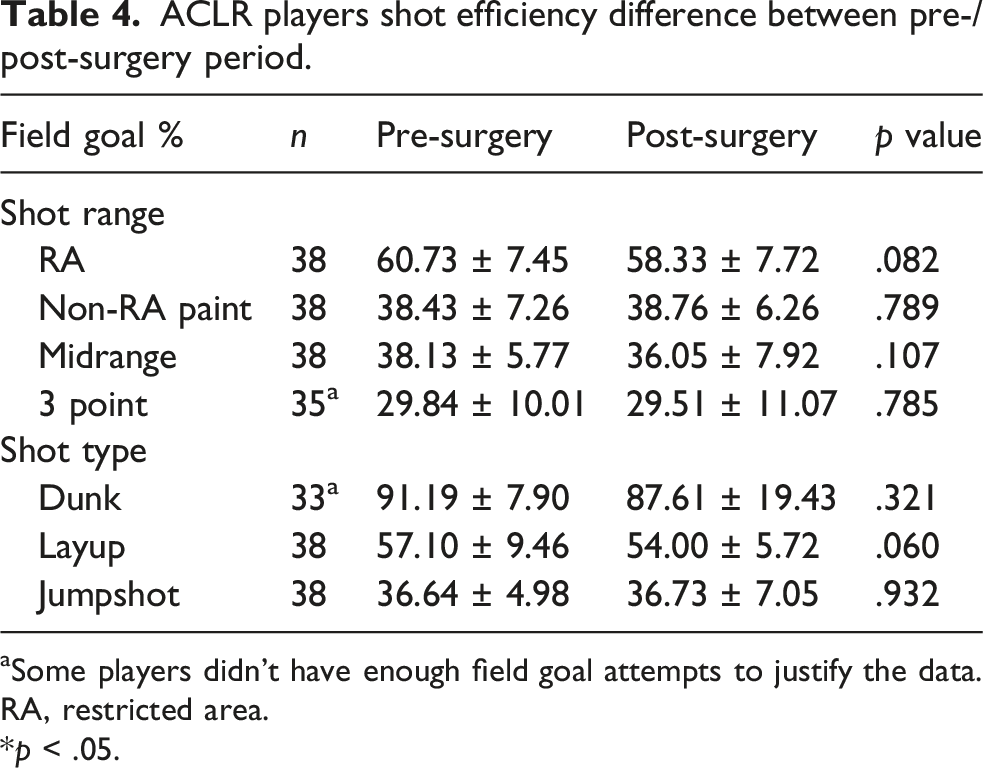
aSome players didn’t have enough field goal attempts to justify the data.
RA, restricted area.
*p < .05.
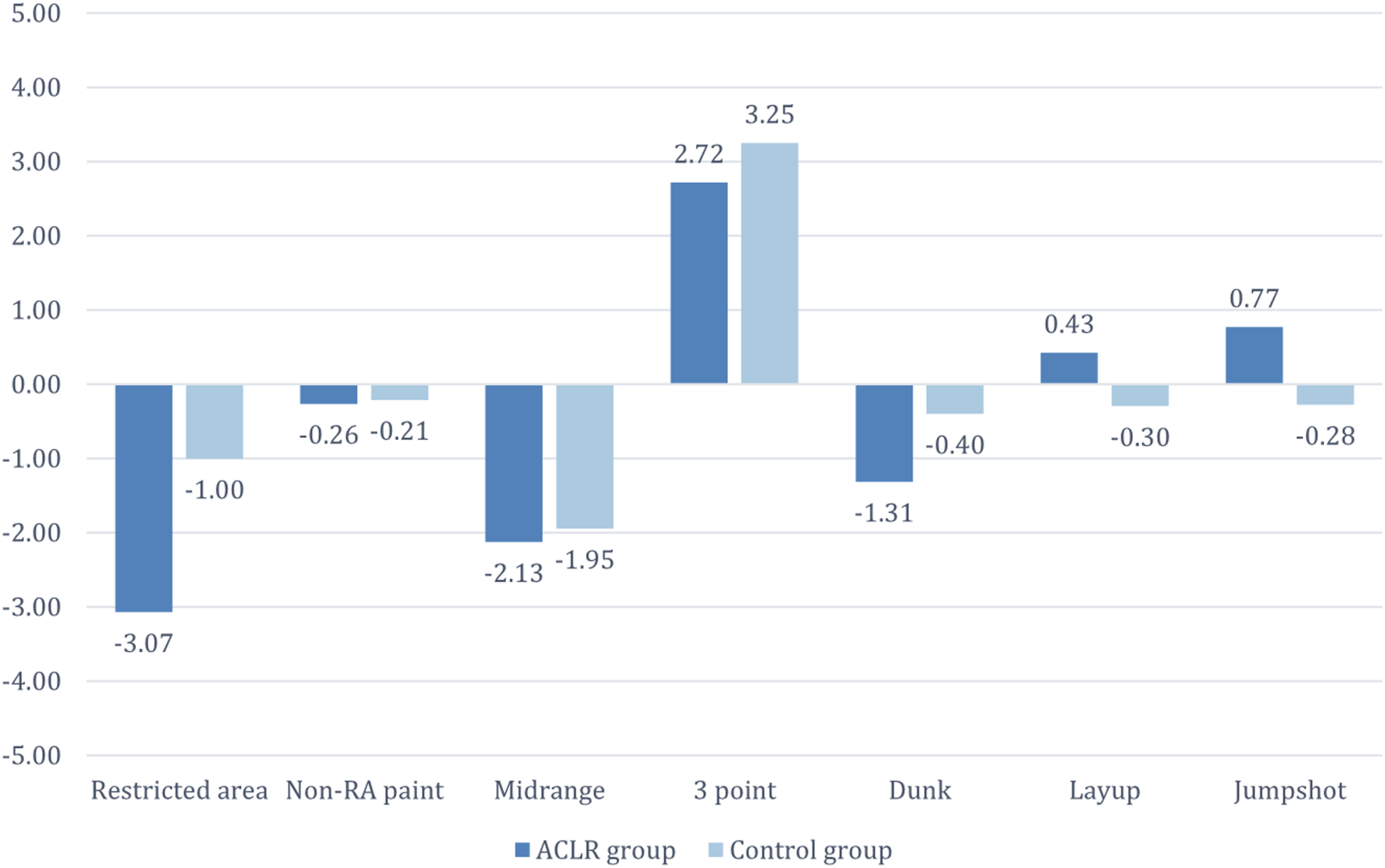
Shot Distribution Differences (Pre-vs Post-Surgery) between ACLR and Control groups: Data represent the change in the frequency percentage (Freq%) of total field goal attempts taken from specific court zones and shot types. Values are expressed as percentage points (%). Further comprehensive data interpretation is provided in section 3.2.2. Shot selection: shot distance, shot distribution, and shot type.
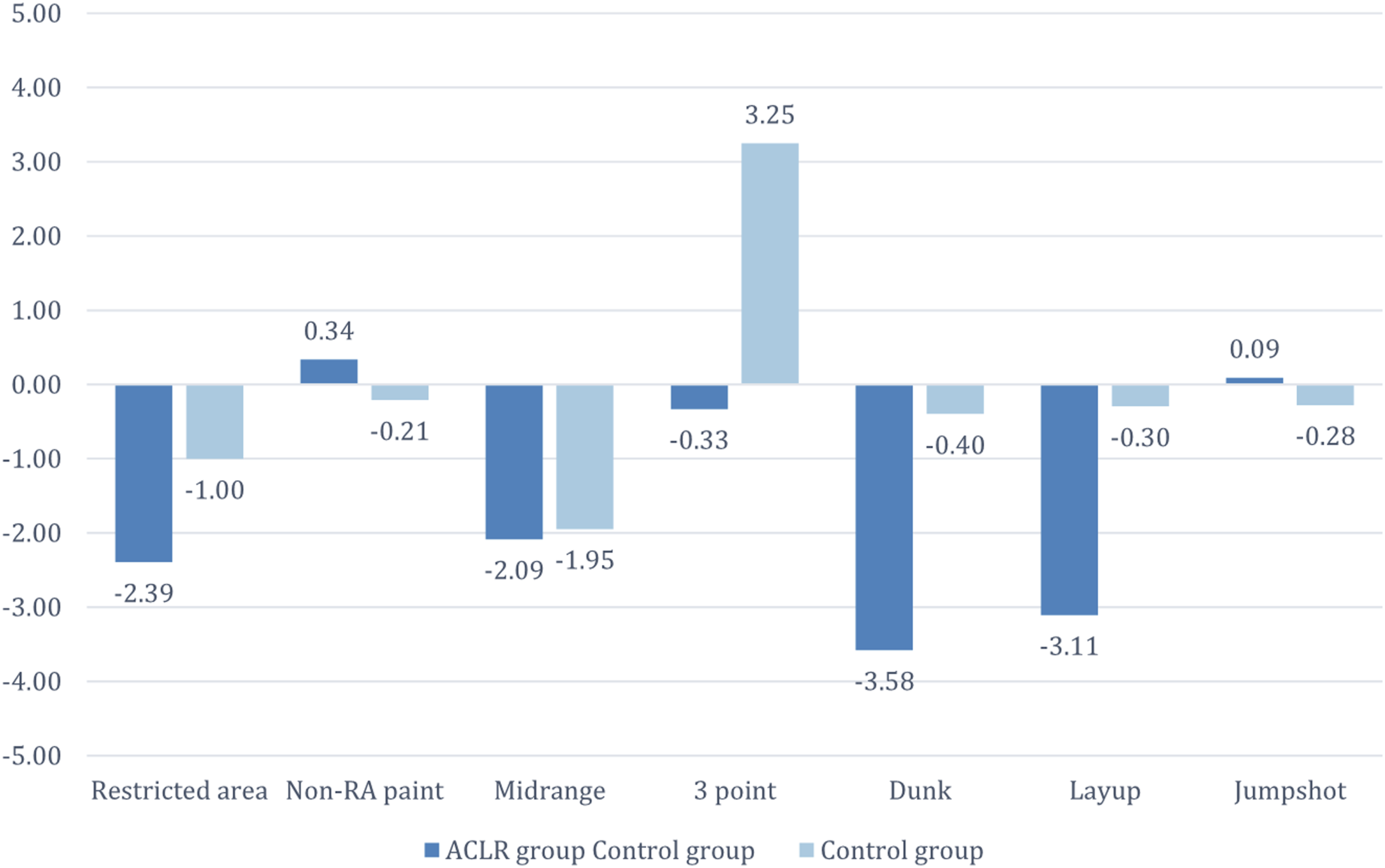
Shot Efficiency Difference (Pre-vs Post-Surgery) between ACLR and Control groups: Data represent the change in field goal percentage (FG%) across various court zones and shot types. Values are expressed as percentage points (%). Further comprehensive data interpretation is provided in section 3.2.2. Shot selection: shot distance, shot distribution, and shot type.
Tracking data (with limited data)
In players with available tracking data (post-2013 seasons), no statistically significant changes were detected in distance traveled per game, average movement speed, drive rate, and field-goal percentage on drives (all exact p > .05). Due to limited sample size of these metric, results should be interpreted cautiously (Figure 5). Tracking Data Difference of pre-/post-surgery period between ACLR group and control group: More comprehensive data interpretation in section 3.2.3. Tracking data.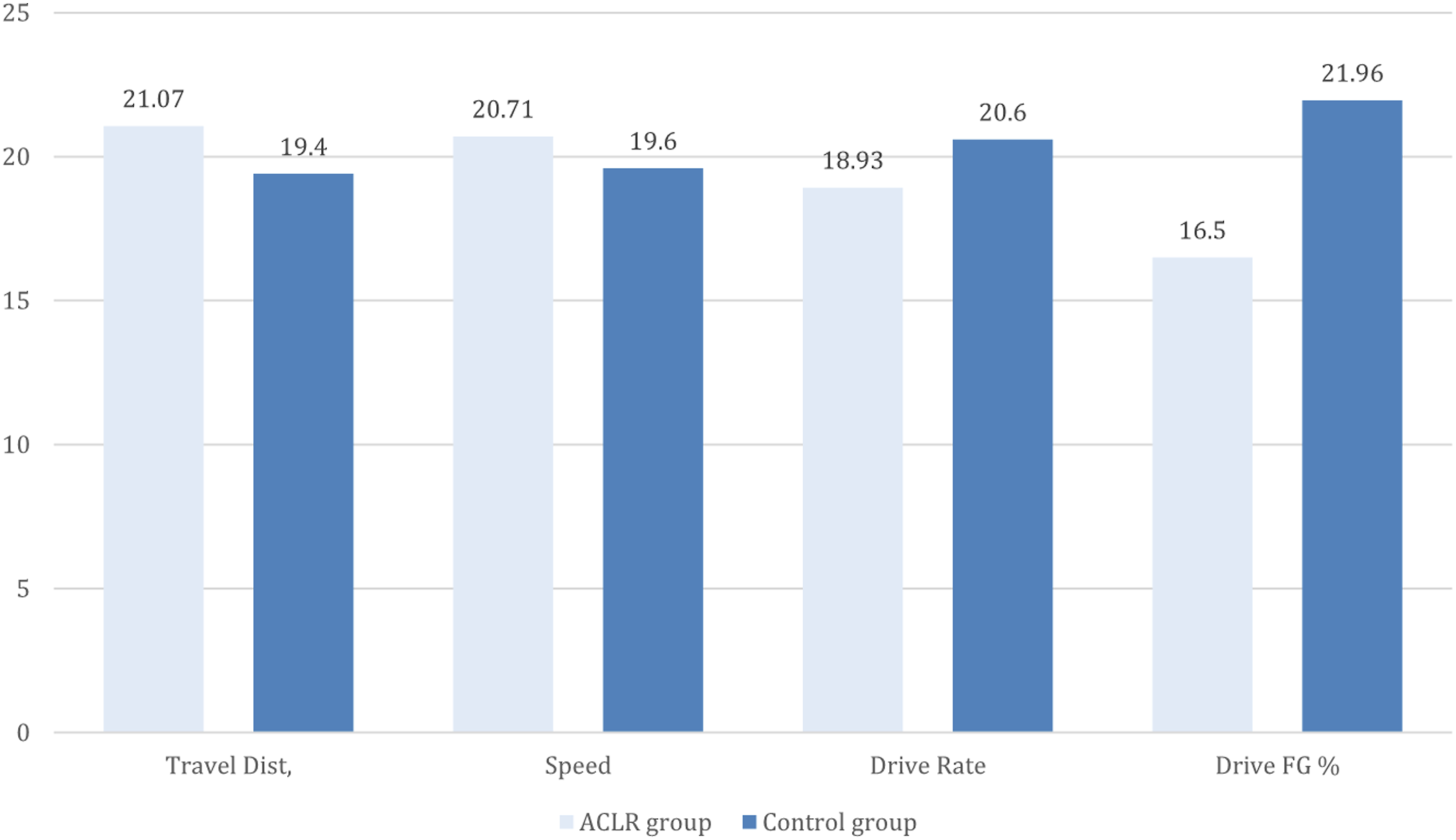
Discussion
This study demonstrates that even among the most successful recovery trajectories in the NBA, anterior cruciate ligament reconstruction (ACLR) is associated with significant longitudinal alterations in both workload and on-court performance. While our methodology inherently introduces survivorship bias by including only players who met the 58-game minimum criteria post-surgery, this bias actually reinforces the clinical significance of our findings. By exclusively analyzing the “best-case scenarios”—players who successfully maintained their careers—the significantly observed declines in minutes played per game (MPG), usage rate (USG%), and dunk frequency suggest that even an optimal clinical outcome may not fully restore an elite athlete’s pre-injury performance ceiling. Consequently, our results provide a conservative yet sobering estimate of the long-term functional prognosis following ACLR in professional basketball. The following discussion details the multifaceted impact of ACLR on player trajectories, exploring specific performance outcomes, biomechanical implications, and the inherent limitations of the study.
A significant reduction in MPG and USG% was observed in the ACLR group. In previous literature, such decreases in playing time and offensive load have often been attributed to diminished durability. 20 However, this causal inference must be made with caution, as these metrics were influenced by confounding factors including medical restrictions, coaching decisions, or player self-adjustment. Therefore, our data can only demonstrate an association with players’ durability.
Regarding play style, the most significant finding was the reduction in dunk frequency among ACLR players (p = .046). This observation aligns with our biomechanical hypothesis—that players may avoid high-impact movements—and may reflect a persistent deficit in vertical explosiveness or a psychological avoidance of high-risk actions.14,15,20 However, an unexpected finding was the lack of a significant compensatory shift (i.e., a significant increase in three-point or mid-range attempts) in the ACLR group. This non-significant result should not be misinterpreted as “no change in play style.” A more plausible explanation is that our study period (2000–2022) coincided with the NBA’s league-wide “three-point revolution.” This era was characterized by a substantial increase in three-point attempt rates, rising from 15.66% to 23.05% between the 2000s and 2010s, as established in previous literature. 21 Although we utilized a similarity-based control group to account for potential biases, the specific differential effects of ACLR may still have been masked by this overarching secular trend.
Despite these interpretive complexities, our findings retain clinical relevance. The concurrent declines in MPG and dunk frequency suggest that while current rehabilitation protocols are effective at “return-to-play” (RTP), they may not fully restore players to their pre-injury “role” or “explosiveness.” This highlights the importance of the late-stage rehabilitation and early return-to-competition phases. Rehabilitation should not conclude when a player is medically cleared; rather, it should continue through structured load management, persistent neuromuscular training, and sport-specific explosiveness drills to prepare the athlete for the long-term demands of an NBA season. 22 Setting a suitable goal for players to reach as a greenlight for return to play is also important, such as achieving the criteria for knee strength and jumping power. 23 Given the observed durability concerns post-ACLR, implementing load management programs that monitor workload distribution, training intensity, and recovery timelines could play a critical role in preventing recurrent knee injuries or even future contralateral ACL injuries.8,24,25
The conclusions of this study must be interpreted cautiously within the context of its significant methodological limitations. Survivorship Bias is arguably the primary limitation of our study. Our inclusion criterion requiring players to appear in at least 58 games both before and after surgery, while based on official NBA statistical minimums, unavoidably introduces severe survivorship bias. Our sample exclusively represents the “most successful” recovery trajectories—players who were able to maintain their careers—while excluding those with severe performance declines, reduced roles, or early retirement (i.e., the “worst outcomes”). Therefore, any conclusion of “achievable long-term functional recovery” drawn from this cohort likely overestimates the average prognosis for an NBA player following ACLR.
This study relied on publicly available media reports (e.g., ESPN, Bleacher Report) for injury and surgery data rather than official medical or league databases. These sources are susceptible to reporting bias, inaccuracies, and omissions (e.g., regarding concomitant injuries or surgical technique). The “Similarity Score” from CraftedNBA, while providing a pragmatic, multidimensional matching approach, has not been formally validated in peer-reviewed literature. As previously discussed, our model cannot disentangle the true physiological impact of the ACLR from external factors such as coaching decisions, team role, and league-wide tactical trends. Tracking Data Sample Size: The limited availability of player tracking data (post 2013-14 season) resulted in smaller sample sizes for these specific analyses, reducing statistical power and necessitating the use of non-parametric tests, which may limit the generalizability of those specific findings.
Based on these limitations, future research should aim to overcome these methodological hurdles. For instance, studies should employ more advanced statistical models (e.g., mixed-effects models) to analyze longitudinal data, which can better account for individual variability and temporal trends. Furthermore, research designs must find ways to quantify rather than exclude the impact of survivorship bias, perhaps by using survival analysis to model career longevity.
Conclusion
In conclusion, this study suggests that NBA athletes may experience shifts in playing time, offensive role, and explosiveness-related play styles following ACLR. However, due to the significant influence of survivorship bias and unmeasured confounders, we cannot draw firm casual conclusions, and can only suggest an association with “durability deficits” or “inevitable role changes.” Our findings underscore the necessity for future research with more robust designs to untangle the complex relationship between the injury, the rehabilitation process, and the evolving tactical environment of the NBA.
Supplemental material
Supplemental material - Impact of anterior cruciate ligament reconstruction on performance metrics and play style in NBA athletes: A matched case-control analysis
Supplemental material for Impact of anterior cruciate ligament reconstruction on performance metrics and play style in NBA athletes: A matched case-control analysis by Tzu-Ming Hon, Chan-Chun Kuo, Yu-Che Lee, Po-Chun Chi, Joe Chih-Hao Chiu, Yi Lu, Cheng-Pang Yang in Journal of Orthopaedic Surgery
Footnotes
Acknowledgments
The authors have no acknowledgments to declare.
Ethical considerations
This study used publicly available, de-identified data and did not involve interaction with human participants; therefore, institutional review board approval and informed consent were not required.
Author contributions
TMH, CCK, and YCL contributed equally to this work and share first authorship.
TMH, CCK, YCL, and PCC collected the data and performed the analyses.
TMH, CCK, and YCL drafted the manuscript.
JCHC, YL, and CPY critically revised the manuscript for important intellectual content.
CPY supervised the study. All authors reviewed and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data used in this study are publicly available. The derived dataset and analytic code are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.