
Abstract
Objective
To assess the effectiveness of operating room nursing pathways based on the nine-grid thinking model in older adults undergoing total knee arthroplasty (TKA).
Methods
110 older adults scheduled for TKA were randomly assigned to either a control group, which received conventional operating room nursing, or a intervention group, which received nursing care guided by the nine-grid thinking model. Key outcomes included surgical efficiency, nursing quality, satisfaction among patients and physicians, incidence of complications, and rehabilitation outcomes were compared between the two groups.
Results
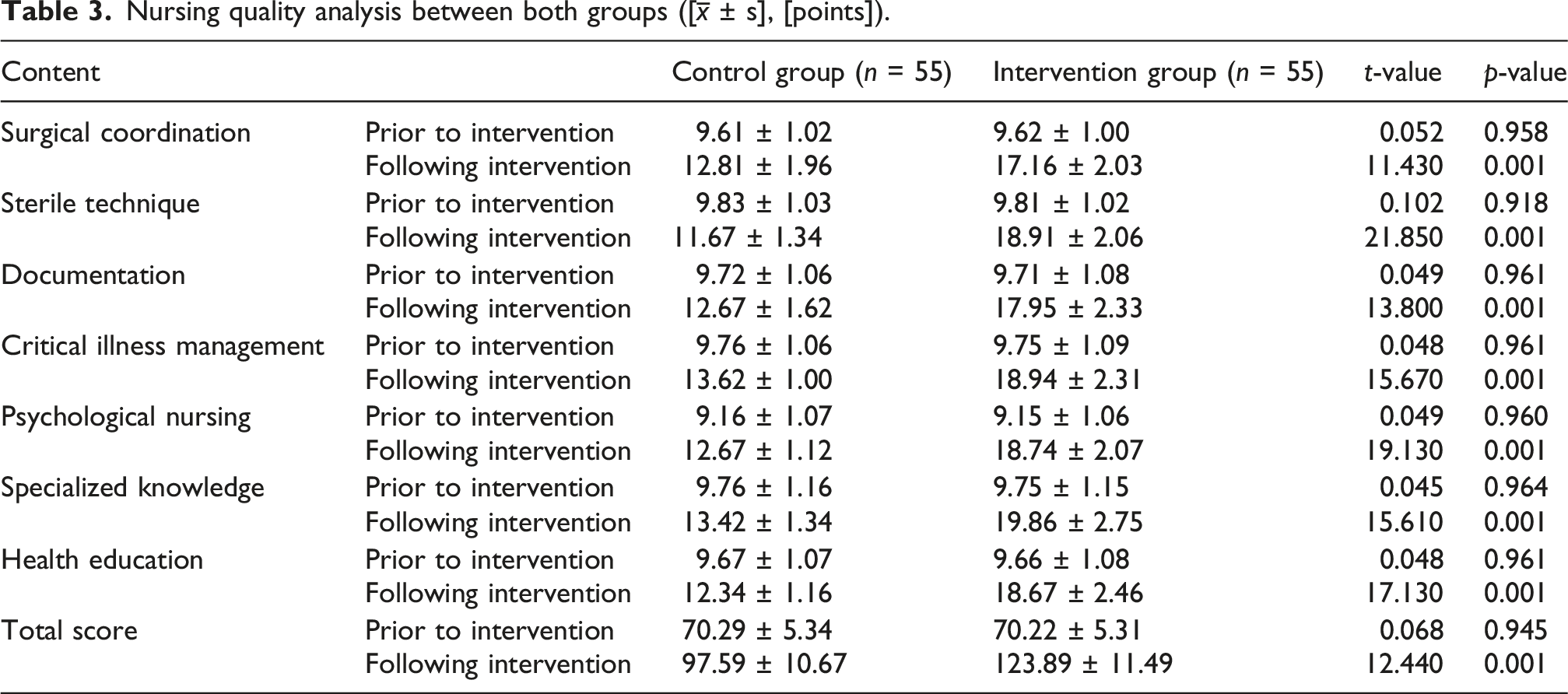
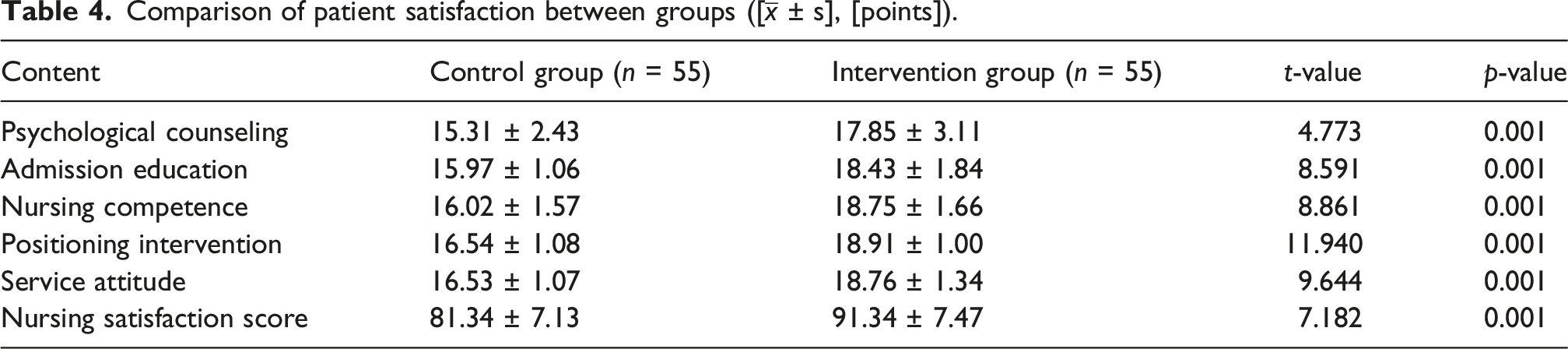
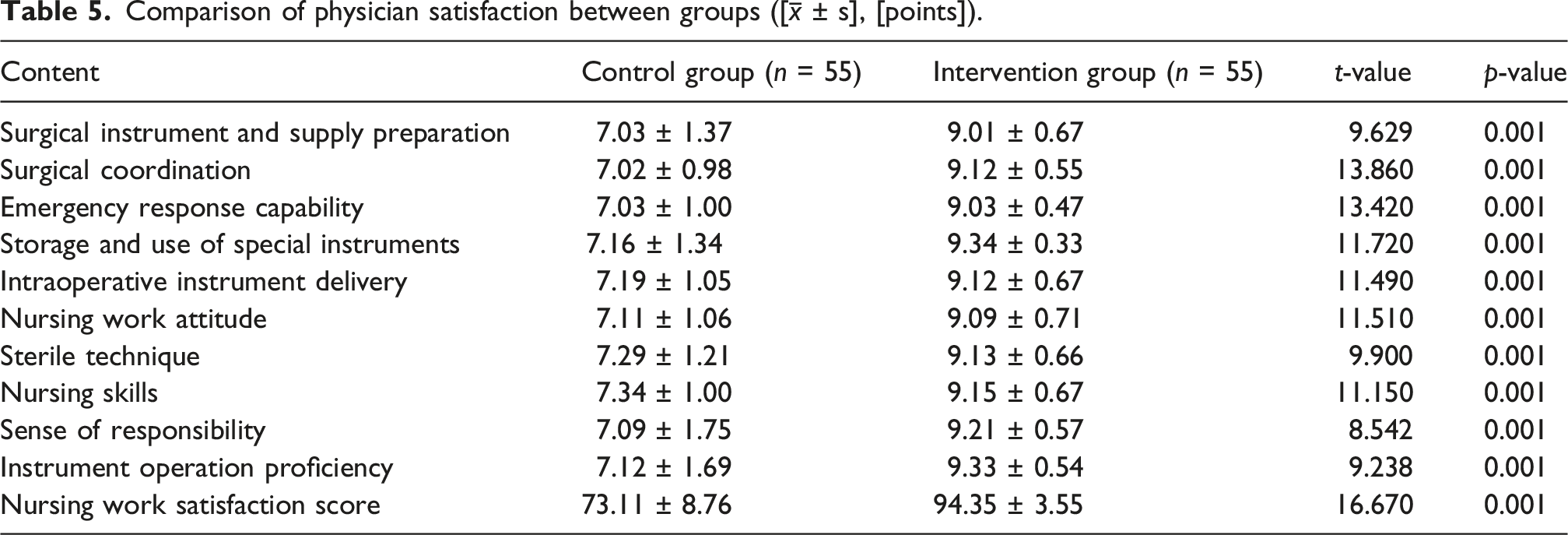
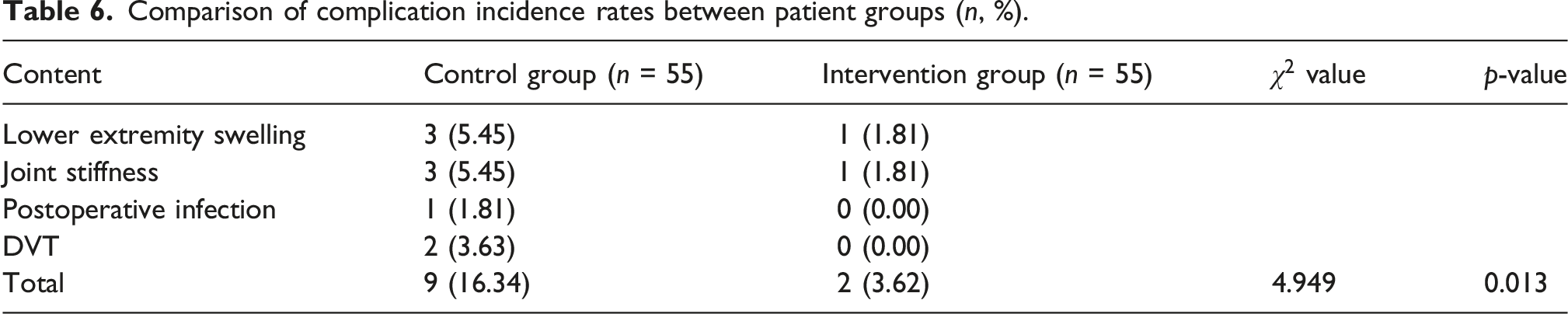
The intervention group had significantly shorter surgical prep (t = 9.106), operative (t = 5.294), and turnover times (t = 14.110) than controls (p < 0.05). After the intervention, the intervention group scored higher on sterile technique (t = 21.850) and overall nursing performance (t = 12.440). Their nurses also reported greater satisfaction with admission education (t = 8.591), positioning (t = 11.940), and overall care (t = 7.182) (p < 0.05). Surgeons rated the intervention group higher for instrument prep (t = 9.629), intraoperative coordination (t = 13.860), instrument delivery (t = 11.490), and overall satisfaction (t = 16.670) (p < 0.05). Deep-vein-thrombosis incidence was lower (χ2 = 4.949), postoperative pain scores were lower (t = 39.980), and ambulation and functional-recovery scores were higher in the intervention group (all p < 0.05).
Conclusion
The application of the nine-grid thinking model significantly enhanced the quality and efficiency of perioperative care for older adults undergoing TKA.
Keywords
Introduction
Total knee replacement procedures were first introduced in the mid-19th century; however, modern knee arthroplasty techniques began taking shape in the 1950s. 1 Current data indicate that approximately 400,000 knee arthroplasty procedures are performed annually in China. Globally, more than one million individuals undergo hip and knee replacement surgeries each year, with this number continuing to rise. 2 This upward trend underscores the growing clinical acceptance of total knee arthroplasty (TKA) as an effective intervention for advanced knee joint pathology. The prevalence of knee joint disease increases significantly with advancing age. 3 Despite this, operating room nursing care for older adults undergoing TKA remains associated with several challenges, including procedural complexity, elevated risk of complications, and variability in nursing quality. Although certain studies have addressed operating room nursing care in this population, many lack specificity and fail to establish standardized, evidence-based protocols, thereby limiting their applicability in clinical practice. 4
In domestic research, operating room nursing for older adults undergoing TKA has demonstrated substantial progress in reducing postoperative pain, minimizing complications, and enhancing surgical success rates. Studies have found that systematic operating room nursing interventions can effectively shorten both surgical duration and length of hospital stay in this population, increase the rate of grade A incision healing, and significantly alleviate anxiety and depression symptoms. For example, one study reported that older adults who received structured intraoperative nursing care had shorter operative and hospitalization times, improved incision healing, and more stable psychological status compared to those who received conventional nursing care. 5 Domestic research has emphasized the relevance of components such as preoperative assessments, intraoperative thermal management, and postoperative pain control in accelerating recovery through evidence-based and comprehensive nursing interventions. 5
Scholars have examined various models, techniques, and assessment strategies in operating room nursing, promoting patient-centered approaches that prioritize thorough preoperative assessment, meticulous intraoperative management, and individualized postoperative rehabilitation planning.6,7 Some studies have integrated enhanced recovery after surgery protocols into intraoperative nursing for TKA, aiming to mitigate surgical stress, reduce complication rates, and support postoperative recovery by enhancing perioperative care. Additionally, research has widely implemented advanced pain management strategies, including multimodal analgesia and patient-controlled analgesia pumps, to improve postoperative comfort and pain outcomes among older adults. 8
This study aimed to develop a high-quality operating room nursing protocol specifically designed for older adults undergoing TKA, using the Nine-Grid Thinking Model, and to assess its clinical effectiveness. The Nine-Grid Thinking Model applies a systematic and structured analytical framework, segmenting operating room nursing management into nine core dimensions: personnel, equipment, environment, process, quality, risk, cost, data, and efficiency. This model facilitates precise coordination and control throughout the surgical process. 9 The objective is to enhance the quality of intraoperative nursing care, support accelerated postoperative recovery, and offer both theoretical and practical guidance for implementing a comprehensive, high-quality nursing model throughout the continuum of care for older adults undergoing TKA.
Methods
Study participants
This study was a single-center, parallel-group, randomized controlled trial (RCT) conducted between November 2023 and November 2024 at our Hospital. Eligible older adults who underwent TKA were randomly assigned to either the intervention group (n = 55) or the control group (n = 55) using a 1:1 allocation ratio via simple randomization with a random number table method. To ensure methodological rigor, we implemented strict inclusion/exclusion criteria, dual-consent procedures for elderly participants, and blinded outcome assessment where feasible. Baseline data, including sex, age, body mass index (BMI), and preoperative range of motion (ROM), were subjected to statistical analysis for both groups. The control group received conventional operating room nursing care, while the intervention group received nursing guided by the nine-grid thinking model based on conventional operating room nursing, enabling direct comparison of the two approaches under controlled conditions (Supplemental Table 1–3). To ensure adequate statistical power, an a priori power analysis was conducted using GPower 3.1. A medium effect size (Cohen’s d = 0.5), significance level α = 0.05 (two-tailed), and target power of 0.80 were specified. The power analysis was performed using GPower 3.1.9.7 (Faul et al., 2009) and PASS 2023 (NCSS, LLC) software, with parameters set at α = 0.05 (two-tailed) and Power = 1-β = 0.80; sensitivity analysis was conducted at 0.90 when target power was not achieved. A random seed number (20240115) was used to ensure reproducibility. Sample size calculation was based on an expected between-group difference in VAS scores of 1.5 points, standard deviation of 2.0 points, α = 0.05, power = 80%, and anticipated dropout rate of 20%. G*Power 3.1 analysis indicated that 55 participants per group were required, resulting in a total planned recruitment of 110 participants. This sample size ensured the stability and reliability of the study findings.
Inclusion and exclusion criteria
Inclusion criteria
(1) Surgical indications for TKA were met; (2) Age between 60 and 80 years; (3) First-time unilateral or bilateral knee replacement surgery was performed; (4) BMI < 35 kg/m2, with varus or valgus deformity <10°.
Exclusion criteria
(1) History of previous knee replacement or tibial/femoral osteotomy; knee flexion range of motion <90°; (2) Varus or valgus deformity >10°; (3) Presence of other lower extremity diseases; (4) Documented emotional or psychiatric disorders; (5) History of serious primary conditions, including cardiovascular or cerebrovascular diseases, that could preclude completion of the study protocol. Provision of informed consent was required for participation. The study was conducted in strict accordance with medical ethical standards and received approval from the Medical Ethics Committee of Shandong Provincial Third Hospital (approval number: [KYLL-2025037]). A dual-confirmation mechanism was implemented for older adult participants; along with the signature of the participant, informed consent from an immediate family member or legal guardian was required.
Intervention methods
Control group
Conventional surgical nursing was implemented according to the following procedures:
(1) Preoperative management: Verification of the wristband ID, surgical site, procedure name, and surgical markings was conducted prior to patient entry into the operating room. The availability of necessary surgical instruments, medications, and equipment was ensured. (2) Anesthesia care: Assistance was provided to the anesthesiologist following the administration of anesthesia, and the patient’s vital signs were continuously monitored. (3) Positioning care: Appropriate positioning was applied according to surgical requirements. (4) Skin preparation: The surgical site was thoroughly cleansed and disinfected. (5) Intraoperative nursing care: Intraoperative changes were managed promptly as they occurred. (6) Postoperative nursing: The pain level, body temperature, respiratory rate, and blood pressure of the patients were monitored. Analgesic and anti-infective therapies were administered in a timely and appropriate manner. (7) Discharge education: Guidance on medication usage and follow-up visit arrangements was provided. Post-discharge health status was monitored.
Intervention group
1. Focused on the head nurse
The head nurse was assigned comprehensive oversight responsibilities over eight other nursing roles. A radial management structure was implemented, wherein adjacent nurses mutually supervised one another and performed cross-checks following the completion of assigned surgical tasks. A departmental zero-tolerance policy was communicated in advance through the internal email system of the hospital or designated WeChat workgroups. Through the application of the multidisciplinary thinking model, a dual-focus approach was adopted, emphasizing both real-time guidance and supervision of operating room nursing staff. This approach promoted individual self-discipline as well as mutual accountability, ensuring timely and effective communication. Feedback and actionable suggestions from nursing staff at all levels were actively solicited and incorporated, supporting a management structure characterized by “upward reporting and downward communication” and “top-down role modeling.” These strategies contributed to a balanced and person-centered approach to nursing management.
From the functional roles of each team, enhancements were made to professional competencies, workflow processes, and operational models. Standardized communication protocols were established among operating room nurses, along with the development of a designated nursing safety section. Continuous evaluations of existing problems were conducted, with corresponding improvement strategies formulated regularly.
In accordance with the N0–N4 nursing competency classification system, a pairing strategy was implemented whereby less experienced nurses were assigned to work with more experienced staff. Each surgical case included the presence of at least one specialist team leader. Nursing personnel were allocated based on appropriate criteria, ensuring that both staffing levels and professional competencies aligned with the surgical demands, thereby minimizing resource inefficiencies.
Centralized team meetings were held regularly to clarify shift responsibilities. These meetings addressed role qualifications, standard operating room nursing procedures for joint surgeries (2024 revised edition), coordination templates for both conventional and robot-assisted TKA, and the standardization of perioperative nursing care for older adults undergoing TKA. Regular brainstorming sessions were conducted to identify improvements, particularly in relation to intraoperative autologous blood transfusion workflows, simplification of the Ruimei blood transfusion system, the on-site counting of more than 100 surgical instruments used in knee replacement procedures, and adherence to critical position protocols. Quarterly and annual professional technical assessment scores were established to assess nursing competencies.
2. Focused on older adults with TKA
Under the leadership of the head nurse, nursing staff participated in delivering this care. Within the nine-grid layout, nurses who were not designated as primary caregivers remained actively involved in supporting the care of these patients. This nursing structure ensured full implementation of substitute emergency rotation responsibilities in the event of personal absences or unforeseen circumstances, thereby reducing the risk of complaints related to the quality of nursing services.
By using the nine-grid thinking model, a person-centered care approach was emphasized, requiring operating room nurses to consider the specific needs of older adults. A health education video accessible via QR code was developed, enabling patients to gain a rapid understanding of the surgical procedure and operating-room environment through mobile scanning.
To optimize patient positioning during surgery and to continuously enhance intraoperative nursing competencies, “Today, I Am the Patient” experiential activities were conducted. In these sessions, nurses were guided to personally experience various TKA surgical positions, facilitating peer learning and reflective practice. This experience enabled faster and more accurate positioning of patients in safe and comfortable postures, contributing to both surgical efficiency and the prevention of neuromuscular and pressure-related injuries associated with prolonged surgeries. Throughout the surgery, intraoperative conditions were closely monitored by nursing personnel. Rapid assessments and early identification of abnormalities were carried out, and coordination with physicians was undertaken as necessary to maintain patient safety. A supportive and welcoming operating room environment was maintained, and a “three-zero” service standard—zero errors, zero complaints, and zero disputes was upheld, contributing to continuous improvement in patient satisfaction with the surgical experience.
High-quality dynamic continuity of care was delivered through structured preoperative visits, intraoperative collaboration, documentation of postoperative follow-up, and satisfaction surveys involving assigned patients. Problems and improvement measures identified by the quality control team were clearly communicated on a monthly basis through a designated WeChat group, ensuring all nursing staff remained informed and capable of accurately recalling and addressing these issues.
Monthly review meetings were convened by the nursing quality management team to review and summarize identified concerns. These sessions were followed by in-depth discussions and evaluations aimed at further enhancing the quality of nursing services.
3. Efficient coordination centered on the surgeons
Patient positioning was conducted by nursing staff in accordance with the placement plan established during preoperative discussions with the physicians, thereby facilitating a prompt initiation of surgical procedures. Preoperative communication with the surgical team was conducted to review patient conditions, planned surgical approaches, and any required specialized supplies. During the procedure, surgical progress was closely monitored by nurses. Surgical items were provided promptly as needed, synchronized intraoperative collaboration with the surgeons was ensured, and the stability of both vital signs and equipment functionality was ensured. TKA was classified as a level 4 procedure and conducted within a Class 100 laminar flow operating room. A minimum interval of 10 min was maintained between consecutive procedures, followed by a 30-min air purification process. All required time points and full-name signatures were documented appropriately. Enhanced environmental monitoring and control measures within the operating room were implemented to ensure compliance with established hygiene standards and surgical protocol requirements. Support was provided to the surgical team in confirming scheduled case start times and coordinating patient entry into the operating room, thereby supporting seamless procedural transitions and minimizing patient wait times.
Regular invitations were extended to the director of the joint surgery department to deliver professional lectures, and all course materials were archived for future reference. Detailed explanations of the procedural steps involved in robotic arm-assisted TKA were provided, and the necessary specialized instruments were prepared in advance. Standardized templates for intraoperative medication administration during TKA were developed based on the documented surgical preferences of the four joint surgery department directors at the institution. These templates were designed for two specific intraoperative time points: before prosthesis insertion and after closure of the joint capsule. The 2024 edition of the Shandong Provincial Third Hospital Joint Replacement Standardized Medication Use was revised accordingly. For example: Director Lin’s cocktail: ropivacaine (2 vials) + 20 mL normal saline.
Director Lin’s tranexamic acid (TXA): ropivacaine (4 vials) + 30 mL normal saline.
Director Hao’s cocktail: ropivacaine (2 vials) + epinephrine hydrochloride (2-3 drops) + compound betamethasone (1 vial) + ketorolac tromethamine (1 vial) + normal saline (78 mL) = 100 mL.
Director Hao’s TXA: ropivacaine (4 vials) + 90 mL normal saline prepared to make up 100 mL.
Prior to prosthesis insertion, a drug cocktail was prepared, the irrigation gun was primed, and hemostatic agents were prepared. These measures enhanced intraoperative coordination and established a standardized process that could be implemented by nurses across varying competency levels. As a result, surgical efficiency was improved, intraoperative disorganization was avoided, and operative time was reduced.
When high-value consumables, prosthesis models, and other surgical requirements were identified, the planned quantities were confirmed with the surgeon. Following the initiation of the case, items introduced into the surgical area were re-verified with the lead surgeon prior to entering the sterile field to prevent unnecessary patient-incurred out-of-pocket expenses. Traceable barcodes from consumables were retained by the circulating nurse and affixed to the complete medical record to allow for verification in the event of an adverse event.
In unanticipated situations, rapid, synchronous collaboration with the surgical team was carried out, with patient safety prioritized throughout the process.
4. Strengthened professional development and standardized training for nursing staff
Based on the analysis of practical experience, monthly training sessions and seminars were conducted regularly, incorporating interactive questioning, group discussions, and heuristic teaching methods. These activities were designed to enhance both the professional knowledge and practical skills of the nursing team. Specialized surgical cases involving TKA were analyzed in depth by senior chief preceptors to deliver expert knowledge, promote critical thinking, and guide nursing staff in identifying and resolving key challenges in clinical practice. Emphasis was placed on nursing career development, with a designated platform for individual growth established. Career planning lectures, TKA-specific technical training, and related activities were implemented to support personalized development pathways. Support for both professional advancement and psychological well-being was provided by the head nurse, who facilitated comprehensive developmental assistance. To strengthen practical competencies and emergency response capabilities, role-reversal experiential training and scenario-based simulation training for TKA procedures were introduced. These simulations enabled nursing staff to become familiar with surgical workflows and to improve responsiveness to unexpected intraoperative events. Monthly assessments were aligned closely with training content and performance outcomes, thereby encouraging active participation.
Standards for operating room nursing procedures and intraoperative medication management modules for TKA were revised annually by specialized joint surgery nurses, based on the preferences of attending surgeons. The standardized TKA surgical nursing coordination “pocket reference guides” were updated to ensure consistency in practice. These guides were disseminated through the “Operating Room Knowledge Exchange Group” and were implemented according to institutional standards.
Statistical methods
Data were analyzed using SPSS version 27.0. Continuous variables were expressed as mean ± standard deviation. Comparisons of continuous variables (e.g., operative time, length of hospital stay) between groups were conducted using independent samples t-tests. Categorical variables (e.g., incidence of complications) were compared using the chi-squared (χ2) test. For repeated measures data, such as quality of life (QOL) scores, repeated measures analysis of variance was used to assess differences across time points and between groups. When appropriate, Pearson’s correlation coefficients were calculated to assess associations between variables. A two-sided α level of 0.05 was used, and p < 0.05 was considered statistically significant.
Results and analysis
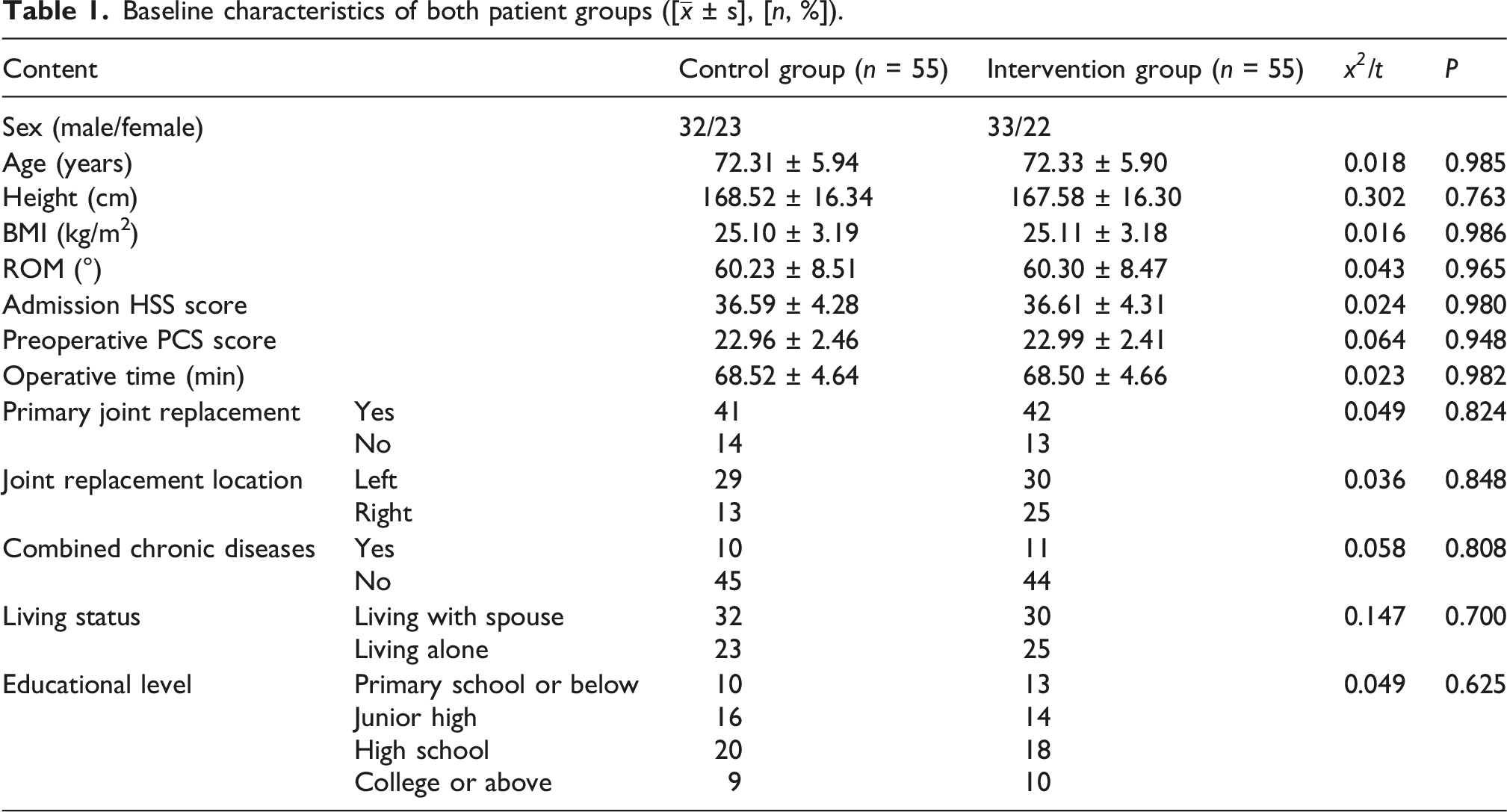
Analysis of general data of both patient groups
Baseline characteristics of both patient groups ([
Analysis of surgical efficiency between both patient groups
Comparison of surgical efficiency between patient groups ([

Analysis of nursing quality between both groups
Nursing quality analysis between both groups ([
Analysis of patient satisfaction between both groups
Comparison of patient satisfaction between groups ([
Analysis of physician satisfaction between both groups
Comparison of physician satisfaction between groups ([
Analysis of complication incidence rate between both patient groups
Comparison of complication incidence rates between patient groups (n, %).
Analysis of rehabilitation outcomes between both patient groups
Comparison of rehabilitation outcomes between patient groups ([

Discussion
The nine-grid thinking model is structured around the subdivision of a specific problem into nine fundamental dimensions: personnel, equipment, environment, process, quality, risk, cost, data, and efficiency. Through comprehensive, multi-dimensional analysis and management, this model facilitates the identification of optimal problem-solving strategies, enhances surgical efficiency, and supports evidence-based improvements in operating room nursing quality for older adults undergoing TKA.10–12 Within personnel management, the clarification of role responsibilities and the reinforcement of team collaboration have been associated with reduced communication inefficiencies and decreased time lost due to ambiguous task allocation, thereby promoting more effective intraoperative coordination. 13 In the area of equipment management, regular inspection and maintenance of surgical instruments has ensured their immediate availability and helped prevent procedure delays caused by equipment malfunctions. 14 For environmental management, the optimization of operating room layout and refinement of cleaning and disinfection protocols have contributed to a reduced risk of surgical site infections. 15 Despite these advantages, notable gaps and limitations remain in the current literature regarding the application of the nine-grid thinking model.
First, limitations were identified in the rigor of research design and the transparency of methodological reporting. For example, several studies did not clearly specify the study design type (e.g., cohort, cross-sectional), thereby raising concerns regarding the credibility and reproducibility of their conclusions.4,5,7 Although one study referenced the impact of multidisciplinary collaboration, specific mechanisms of collaboration and the criteria used for evaluation were insufficiently described, leaving the operationalization of intervention measures undefined. 10 This lack of methodological clarity may limit the generalizability of the findings.
Second, the application of the nine-grid thinking model has largely remained at the theoretical level and lacks sufficient empirical validation. Although several studies have proposed that the model may optimize specific aspects like data management, rehabilitation planning, or pain management, few studies have systematically evaluated its effectiveness. One study proposed the use of the nine-grid model for optimizing data management but did not specify how relevant variables or indicators should be integrated. 3 Similarly, another study proposed incorporating pain management within the model but did not design a controlled experiment to assess its efficacy. 2 This trend of frequent theoretical recommendations without corresponding practical implementation highlights the absence of bridging studies that translate conceptual frameworks into clearly defined and actionable intervention strategies.
Third, the measurement of key variables and the analysis of influencing factors in existing research have often lacked comprehensiveness. For instance, one study examined factors influencing psychological resilience and empathetic understanding related to patients’ perioperative psychological stress but did not incorporate additional relevant variables such as social support or economic status. 5 Another study conducted a comparison of suturing methods without accounting for the potential impact of comorbid complications in patients with diabetes (e.g., microcirculatory disorders), which may have affected clinical outcomes. 6 Omission of these variables may obscure underlying associations and result in biased interpretations. Furthermore, the absence of standardized measurement tools such as the Connor-Davidson Resilience Scale for assessing psychological resilience was noted in most studies, thereby limiting the comparability and generalizability of findings across different research settings.
Fourth, a lack of long-term follow-up and insufficient diversity in outcome assessments were also identified in existing research. Most studies have concentrated on short-term effects, such as length of hospital stay or immediate postoperative cognitive function, while long-term outcomes like prosthesis survival rates or QOL have been largely overlooked. For example, one study reported that transcutaneous electrical acupoint stimulation improved postoperative cognitive dysfunction, yet cognitive function was not assessed beyond a three-month follow-up period. 1 Another study examined only the effects of pre-admission management using the 5A nursing model, without assessing postoperative rehabilitation quality at six months. 16 This emphasis on short-term results may lead to an overestimation of the clinical value of certain intervention strategies.
The incorporation of an assessment and feedback loop addresses the limitations associated with traditional empirical management approaches, thereby enhancing the scientific validity and specificity of quality improvement measures. This process not only facilitates the continuous refinement of nursing standards but also fosters quality awareness within the team, ultimately guiding operating room nursing practices along a progressive and upward developmental trajectory of iterative improvement. 17
Finally, limitations have been noted in the cross-cultural adaptability and personalized application of the nine-grid thinking model. Most studies have been conducted within a single medical institution or geographic region, which may reflect localized hospital workflows without accounting for variations in healthcare resource availability or the cultural backgrounds of patients. 10 In one study, the home-based rehabilitation program was not accompanied by an explanation of how it could be adapted to meet the needs of rural or low-income populations. 7 Although the nine-grid thinking model is centered on systematization, its adaptability across diverse healthcare settings and patient populations has not been comprehensively examined in current research.
Moreover, the sample size calculation was primarily based on the between-group difference in postoperative pain scores (VAS), which yielded 55 participants per group with 80% power; however, this may have been underpowered to detect clinically meaningful differences in secondary outcomes with lower event rates, such as complication incidence and specific satisfaction subdomains. Additionally, as a single-center study conducted at a tertiary-grade A hospital with specialized joint replacement expertise, the findings may have limited external validity, as the homogeneous patient population, standardized surgical protocols, and experienced nursing teams may not reflect the variability in clinical practice across different healthcare settings, warranting cautious interpretation when generalizing these results to broader populations. Finally, this study was limited by its short follow-up period, which precluded assessment of critical long-term TKA outcomes including chronic pain, prosthesis survival, and readmission rates; future research should incorporate extended follow-up protocols to validate the sustained effectiveness of the nine-grid thinking model.
In summary, future research should be directed toward the following areas of improvement: (1) clarification of the operational definition of the nine-grid thinking model and the implementation of empirical validation studies; (2) enhancement of research design transparency and the establishment of long-term follow-up mechanisms; (3) inclusion of more comprehensive variables alongside the use of standardized measurement instruments; and (4) examination of the adaptability of the model across diverse healthcare environments. By addressing these existing limitations, the transition of the nine-grid thinking model from a theoretical framework to a practical tool for clinical application may be more effectively achieved.
The nine-grid thinking model enables precise control of the surgical process through the application of systematic and structured analytical methods. Within this model, nursing personnel are assigned to positions corresponding to the nine-grid layout, with each individual responsible for one or more specific areas of work. Mutual supervision and cross-checking are conducted, allowing for the prompt identification and correction of deviations. This adjacent arrangement promotes closer collaboration among nursing staff, thereby contributing to improvements in the overall quality of nursing care. 18 The model is characterized by a strong patient-centered orientation, with its design originating from the perspective of the patient and shifting the focus of nursing practice toward the prioritization of patient needs. The principle of placing the patient first is upheld, requiring nursing personnel to rapidly adjust their approach to empathetically recognize the psychological stress commonly experienced by surgical patients during the perioperative period, including manifestations of tension, anxiety, and fear. 19 To support this goal, emphasis must be placed on improving the overall quality of surgical nursing and implementing a comprehensive care model that ensures each patient receives individualized, high-quality care within the operating room setting, thereby enhancing the overall healthcare experience and satisfaction.
Conclusion
The operating room nursing pathway developed using the nine-grid thinking model resulted in improved efficiency across the entire surgical period through systematic process optimization. This approach contributed to sustained improvements in nursing quality, reciprocal enhancement of physician–patient satisfaction, effective prevention and management of complication risks, and continuous optimization of rehabilitation outcomes. However, as this study was observational in nature and conducted within a single tertiary-grade A hospital, its generalizability remains limited. Further investigation and validation are required to assess the external applicability of these findings.
Supplemental material
Supplemental material - Implementation of a nine-grid thinking model to optimize operating room nursing pathways for older adults undergoing total knee arthroplasty
Supplemental material for Implementation of a nine-grid thinking model to optimize operating room nursing pathways for older adults undergoing total knee arthroplasty by Yuquan Tian, Meng Qi, Qing Wang, Huijun Zhang, in Journal of Orthopaedic Surgery
Footnotes
Ethical considerations
This study was conducted in accordance with the declaration of Helsinki.This study was conducted with approval from the Ethics Committee of Shandong Provincial Third Hospital (Approval number:KYLL-2025037). A written informed consent was obtained from all participants.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data generated or analysed during this study are included in this article. Further enquiries can be directed to the corresponding author.
Supplemental material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.