
Abstract
Background
Pelvic tilt (PT) is a key spinopelvic parameter, but direct measurement may be limited on routine lateral radiographs when the femoral heads are obscured. Anterior pelvic plane angle (APPA) and iliac tilt (IT) may serve as alternative descriptors of pelvic orientation, but the optimal IT-derived metric for estimating PT remains unclear.
Methods
We retrospectively reviewed 977 consecutive individuals who underwent standardized standing lateral whole-spine radiography between February 2024 and November 2025. Only radiographs without radiographically evident structural spinal pathology and with directly measurable PT were included. Pelvic state was classified by APPA. Candidate IT measurements, including superior iliac tilt (ITS), inferior iliac tilt (ITI), and mean iliac tilt (ITM), were compared in terms of measurability, reliability, and estimation error. Linear regression models were then developed to estimate PT from ITM and internally validated using 10-fold cross-validation.
Results
Of the 977 individuals, 660 (67.6%) showed pelvic retroversion, 311 (31.8%) anteversion, and 6 (0.6%) a neutral state. APPA-defined retroversion was more frequently observed in older age groups, reaching 85.7% in participants aged ≥70 years. ITM provided the most favorable overall performance, with 94.2% measurability, high reproducibility, the lowest mean absolute error (3.17°), and the narrowest 95% limits of agreement (−8.21° to 8.21°). PT correlated most strongly with ITM (r = 0.87, P < 0.001). The model incorporating ITM, age, and sex showed the best internally validated performance (R2 = 0.79, RMSE = 3.91°, MAE = 3.01°).
Conclusions
In this cohort with directly measurable PT, APPA-defined retroversion was more frequent in older age groups. ITM may provide an approximate PT estimate when direct PT measurement is limited, but further validation is needed in PT-nonmeasurable radiographs.
Keywords
Introduction
Sagittal spinal alignment is central to the human capacity to remain upright and to walk with relatively low energy expenditure. When the deviation from ideal alignment is small, overall balance can often be preserved because the body recruits compensatory adjustments across the spine, pelvis, and lower extremities.1,2 As the imbalance progresses beyond what these mechanisms can accommodate, clinical consequences become more apparent: pain tends to intensify, functional performance declines, and the risk of perioperative complications may increase.3,4 The pelvis plays a pivotal role in this process. It functions as the structural bridge between the trunk and the lower extremities and, through rotation in the sagittal plane, contributes directly to compensatory postural control. Accordingly, assessment of pelvic status is important not only for classifying spinal deformity and defining corrective targets, but also for guiding clinical decision-making in which hip–spine interaction is a key consideration.5,6 From an imaging standpoint, a pattern of increasing pelvic retroversion accompanied by greater anterior trunk inclination is often paralleled by a decline in patient-reported quality of life. 5 In the classic framework, pelvic incidence (PI) is viewed as a relatively stable morphologic parameter, whereas pelvic tilt (PT) and sacral slope (SS) are positional measures that can shift with posture and compensatory demands. Together, PI, PT, and SS form the PI–PT–SS geometric chain, which in turn shapes lumbar lordosis and overall sagittal alignment.7–9 Therefore, PT serves not only as an index of compensatory pelvic retroversion but also as a parameter closely associated with functional outcomes in adult spinal deformity.5,10,11
However, Tyrakowski et al. reported that classic parameters such as PT, PI, SS are susceptible to pelvic rotation and changes in body position, leading to variability and increased measurement error.12–14 In their synthesis of pelvic orientation measurement systems, Veilleux et al. likewise emphasized that, because PT and SS depend on posture, they may become “variable and even unreliable”. They therefore suggested several alternative metrics that place greater emphasis on pelvic morphology, including the anterior pelvic plane (APP) and APP-derived angles such as the sacropubic angle and pelvic–Lewinnek angle (corresponding to SPA and PLA, respectively).15–17
Against this backdrop, investigators have sought new parameters that characterize pelvic state more robustly, ideally remaining stable even when pelvic rotation occurs or when key anatomic landmarks are not clearly visible. The APP-based angular framework described by Ohashi et al. offers a way to depict pelvic state more directly. It has been used to report normative values in healthy populations and to examine relationships with spinopelvic parameters.18–20 In parallel, Doi et al. 21 proposed constructing an iliac tilt angle (IT) from an iliac cortical density line and using IT to estimate PT, thereby avoiding the prerequisite that the femoral head center must be identifiable. This point is clinically consequential. In routine radiographs, the femoral head is not uncommonly difficult to delineate because of field-of-view truncation, overlap, or image quality, and PT measurability drops accordingly. By contrast, IT relies more heavily on visualization of iliac morphology. In principle, it could increase the proportion of images that remain usable for assessment.
Building on these considerations, our group pursued two lines of preliminary work. First, Zhao et al. 22 supplemented and standardized the measurement procedure for pediatric IT. Haoqi et al. 23 examined APP-related angles in pediatric and adolescent cohorts, providing initial experience to support pelvic-state stratification. Second, while reviewing the APP framework, we noted that pelvic orientation can be categorized into three states based on APP direction—anterior tilt, near-neutral, and posterior tilt—consistent with the observations reported by Pizones et al.15,24
Therefore, the primary aim of this study was to evaluate whether IT could provide a measurable, reliable, and clinically interpretable estimate of PT on standing lateral radiographs. The secondary aim was to characterize APPA-defined pelvic state in a large standing radiographic cohort and to explore whether pelvic state was associated with IT distribution and IT–PT estimation performance. Through this framework, APPA-defined pelvic state was used as a descriptive and stratified radiographic context, whereas IT-based PT estimation represented the main analytical focus of the study.
Methods
Study population and eligibility criteria
This retrospective radiographic study reviewed consecutive individuals who underwent standardized standing lateral whole-spine radiography at the spine outpatient clinic of the Third Hospital of Hebei Medical University between February 2024 and November 2025. Because the study cohort was derived from a clinical outpatient population, it should not be considered representative of asymptomatic healthy individuals. Rather, eligible radiographs were those showing no evident structural spinal pathology that would substantially interfere with sagittal spinopelvic assessment. For model development and error assessment, direct PT measurement was required because measured PT served as the reference standard against which iliac tilt–derived estimates were evaluated. Accordingly, radiographs in which PT could not be directly measured because of inadequate visualization of the femoral heads were excluded from the analytic cohort. The study was approved by the Ethics Committee of the Third Hospital of Hebei Medical University (K2022-067-1), and all procedures were performed in accordance with the Declaration of Helsinki. Written informed consent to participate was obtained from all participants and/or their legal guardians, as appropriate.
Eligible individuals had standardized standing lateral radiographs with sufficient visualization of the pelvis and sagittal alignment parameters. Exclusion criteria were: (1) inadequate image quality, unidentifiable key anatomic landmarks, or substantial rotational malposition; (2) inadequate visualization of the femoral heads precluding direct PT measurement; (3) radiographic evidence of spinal deformity or other spinal abnormalities, including scoliosis defined as a coronal Cobb angle ≥10°, 25 congenital vertebral anomalies, prior spinal trauma, spinal infection, tumor, or previous spinal surgery; and (4) pelvic, hip, or lower-extremity abnormalities that could affect pelvic orientation measurements.
Imaging measurements and parameter definitions
All patients were examined using a standardized radiographic protocol. Radiographs were obtained in a comfortable standing position, with both shoulders and elbows placed in front of the body. All imaging data were stored and retrieved through the Picture Archiving and Communication System (PACS). Measurements were performed using Surgimap software. Parameters were defined as follows (Figure 1). • Pelvic tilt (PT): the angle between a vertical line and the line connecting the midpoint of the sacral endplate to the center of the femoral head, reflecting pelvic spatial orientation. • Pelvic incidence (PI): the angle between the line perpendicular to the superior endplate of S1 at its midpoint and the line connecting this point to the bicoxofemoral axis (line joining the centers of the bilateral femoral heads). • Sacral slope (SS): the angle between the superior endplate of S1 and the horizontal line, indicating the inclination of the sacral endplate. • Lumbar lordosis (LL) and thoracic kyphosis (TK): LL was measured from the superior endplate of L1 to the superior endplate of S1, and TK from T5 to T12, using the Cobb method. • Anterior pelvic plane angle (APPA): The angle between the vertical line and the anterior pelvic plane (APP). APP is defined as the plane passing through the pubic symphysis and the anterior superior iliac spines. APPA is negative when the APP lies anterior to the vertical line and positive when the APP lies posterior to the vertical line; APPA is recorded as 0° when the APP coincides with the vertical line. The APPA = 0 group was retained only as a mathematical neutral reference and was not interpreted as an independent clinical phenotype. • Proximal spinal angle (PSA): the angle between the horizontal line and the line connecting the pubic tubercles to the sacral promontory. • Sagittal vertical axis (SVA, C7–S1): the horizontal offset from a plumb line dropped from the center of C7 to the posterosuperior corner of S1. SVA is positive when the C7 center of mass is anterior to the posterosuperior corner of S1 and negative otherwise. • Iliac tilt (IT): the angle between the iliac cortical density line and a vertical line. If the iliac cortical density lines on both sides did not coincide, angles were recorded separately as IT superior (ITS) and IT inferior (ITI). The mean of ITI and ITS was defined as ITM. If only one iliac cortical density line was present on the radiograph (i.e., ITS coincided with ITI), the value was recorded as ITS by default, and ITS equaled ITM. Schematic illustration of the measurement methods for each parameter.

Reliability assessment
Radiographic measurements were performed independently by three fellowship-trained spine surgeons using Surgimap software. To assess intraobserver reliability, each observer repeated the measurements after an interval of 2–3 weeks and was blinded to the initial results. To assess interobserver reliability, the measurements obtained by the three observers were compared independently under blinded conditions. Reliability was quantified using intraclass correlation coefficients (ICCs) with 95% confidence intervals based on a two-way random-effects model and absolute-agreement definition. ICC values were interpreted according to conventional criteria, with higher values indicating stronger reproducibility. 26
Statistical analysis and model development
All analyses were performed using SPSS version 26.0 (IBM Corp., Armonk, NY, USA). Continuous variables are presented as mean ± standard deviation, and categorical variables as counts and percentages. Normality was assessed using the Shapiro–Wilk test. Between-group comparisons were performed using the independent-samples t test for normally distributed variables and the Mann–Whitney u test for non-normally distributed variables. Categorical variables were compared using the chi-square test or Fisher’s exact test, as appropriate. All tests were two-sided, and p < 0.05 was considered statistically significant.
For descriptive analyses, participants were stratified into predefined age groups (<18, 18–29, 30–39, 40–49, 50–59, 60–69, and ≥70 years). Pelvic state was classified according to APPA as retroversion (APPA > 0), neutral (APPA = 0), or anteversion (APPA < 0) (Figure 2). Because the neutral group was very small, it was included in descriptive summaries only and excluded from inferential comparisons between the retroversion and anteversion groups. Pelvic positional states. (a) Pelvic retroversion (APPA >0); (b) neutral pelvic position (APPA = 0); (c) pelvic anteversion (APPA <0).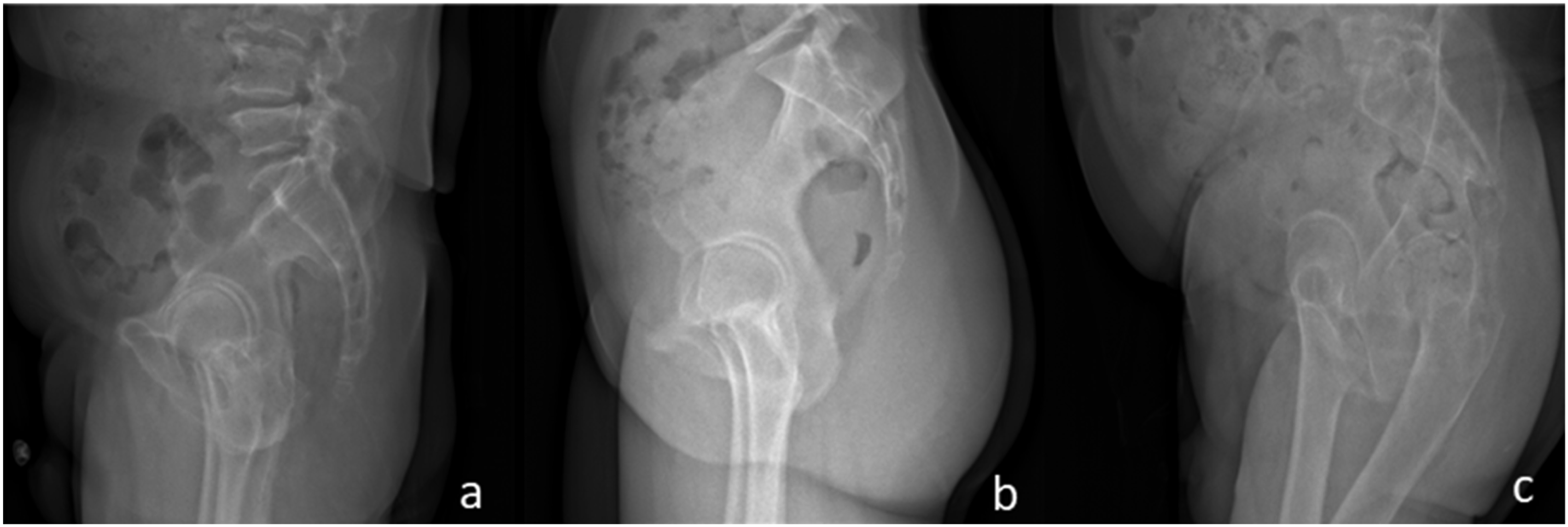
Candidate iliac tilt metrics (ITS, ITI, and ITM) were first compared in terms of measurability and estimation error relative to measured PT. Measured PT served as the reference standard for evaluating IT-derived PT estimates; therefore, these analyses were performed in radiographs in which PT was directly measurable. Estimation error was summarized using mean absolute error (MAE), mean prediction error (bias), standard deviation of the error, and 95% limits of agreement. 27 Available-case analysis was used for each IT-derived metric, and radiographs in which a specific IT metric could not be measured were excluded only from analyses involving that metric. Correlations among radiographic parameters were assessed using Pearson correlation coefficients. To examine age-related trends in ITM within APPA-stratified groups, linear regression was performed with age entered as a continuous variable and regression coefficients expressed per 10-years increase.
For PT estimation, linear regression models were developed with measured PT as the dependent variable. Model 1 included ITM alone, and Model 2 additionally included age and sex. Since ITM was the predictor of interest in both models, only radiographs with measurable ITM were included in the ITM-based regression analyses. Linear regression assumptions were assessed using residual-versus-fitted plots, Q–Q plots of standardized residuals, and variance inflation factors (VIFs). Model performance was evaluated using R2, root mean square error (RMSE), and mean absolute error (MAE). Internal validation was performed using 10-fold cross-validation based on out-of-fold predictions. Calibration was assessed using calibration-in-the-large and calibration slope. 28
Results
Demographic characteristics and baseline sagittal radiographic parameters stratified by APPA sign.
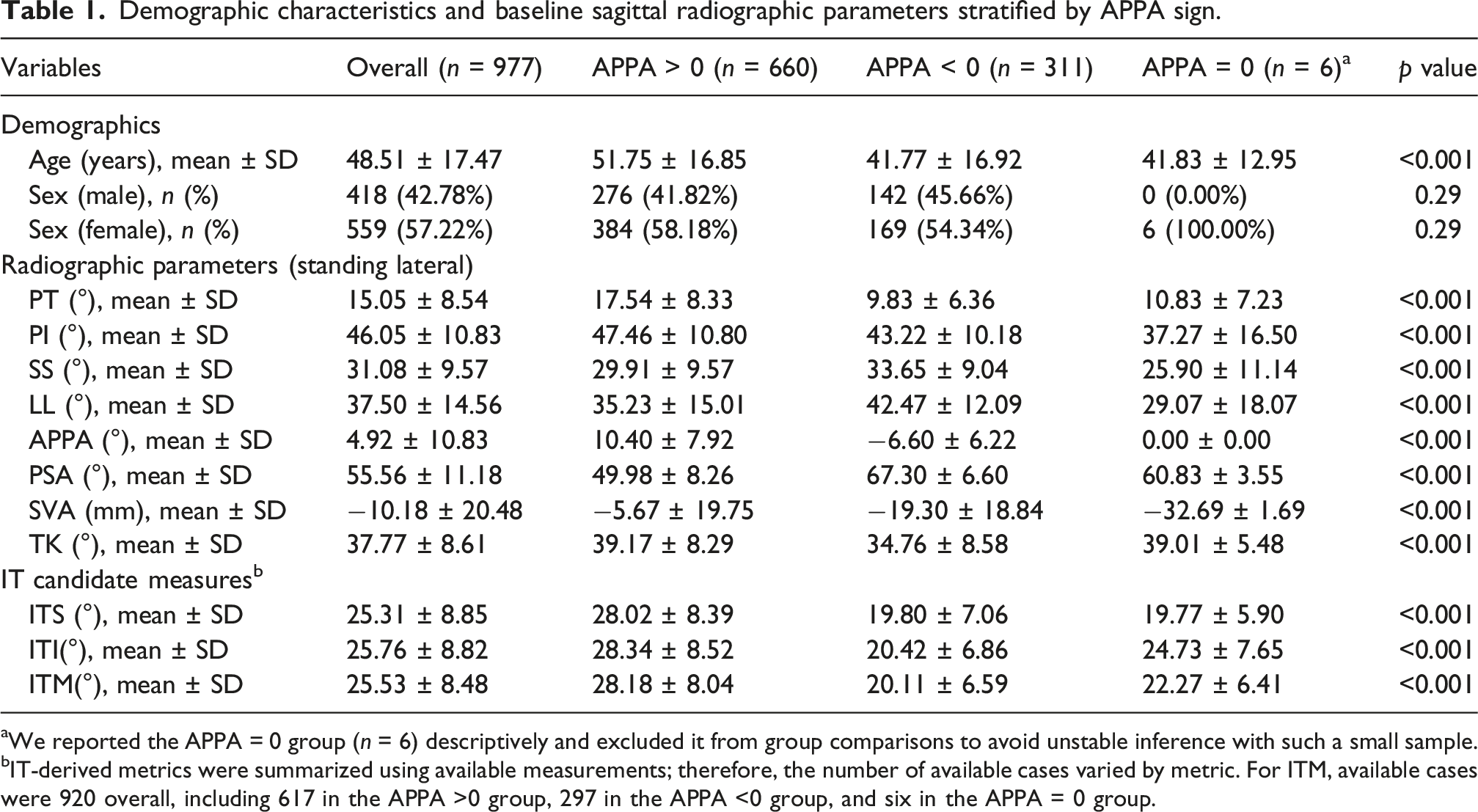
aWe reported the APPA = 0 group (n = 6) descriptively and excluded it from group comparisons to avoid unstable inference with such a small sample.
bIT-derived metrics were summarized using available measurements; therefore, the number of available cases varied by metric. For ITM, available cases were 920 overall, including 617 in the APPA >0 group, 297 in the APPA <0 group, and six in the APPA = 0 group.
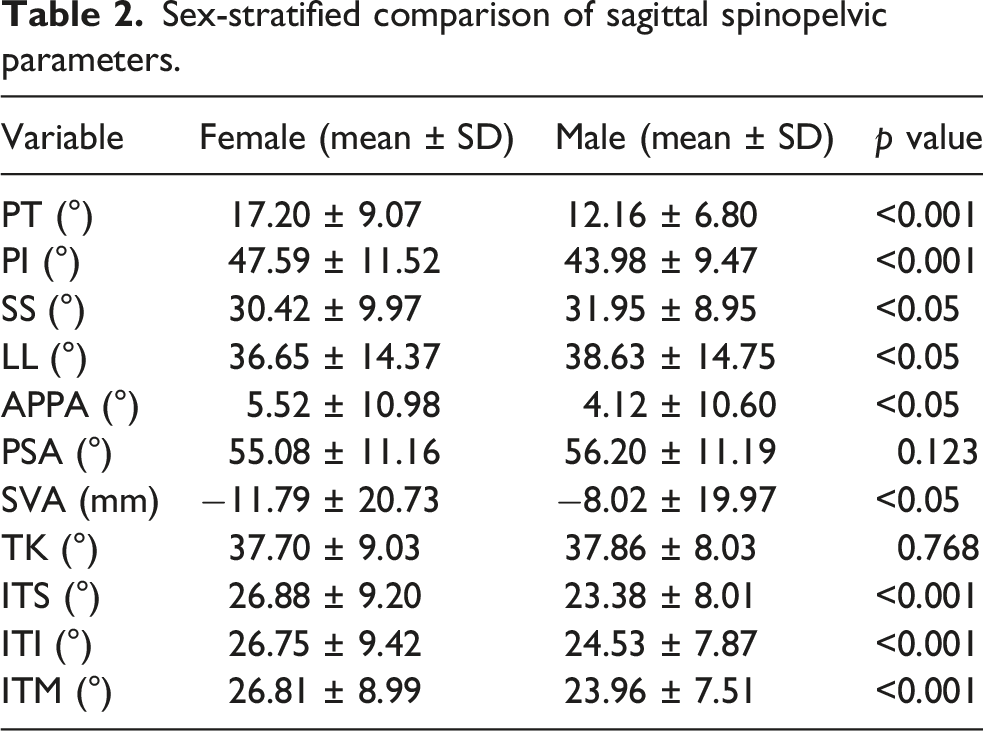
Sex-stratified comparison of sagittal spinopelvic parameters.
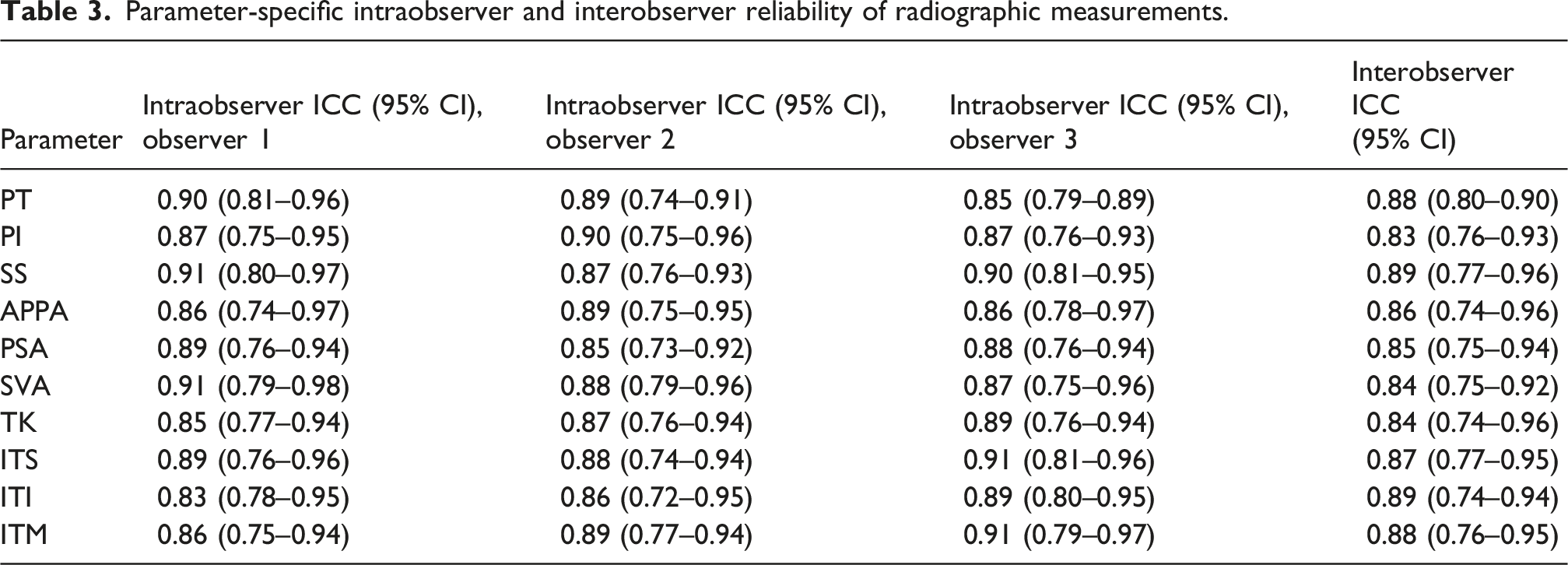
Parameter-specific intraobserver and interobserver reliability of radiographic measurements.
Comparison of candidate IT metrics for measurability and univariable PT estimation performance.

aEstimation error was calculated from metric-specific univariable linear regression predictions. Bias = mean (Predicted PT − Measured PT); 95% LoA = bias ± 1.96 × SD of the prediction error.
Age-stratified distribution of APPA.

ITM distribution across age groups stratified by APPA and the age-related trend (β per 10 years).

Correlation analysis showed that PT was most strongly correlated with ITM (r = 0.87, p < 0.001). APPA was moderately correlated with ITM (r = 0.62, p < 0.001) and PT (r = 0.59, p < 0.001), supporting the use of APPA-defined pelvic state as a stratified radiographic context. The full Pearson correlation matrix and heatmap are provided in Supplemental Figure S2 and Table S1.
Regression models to estimate PT from ITM: coefficients and internal validation performance.

Equations: Model 1: PT = −7.29 + 0.87·ITM, Model 2: PT = −6.36 + 0.83·ITM +0.03·Age −2.86·Sex.
aSex was recorded as male/female (self-reported/medical record) and coded as male = 1, female = 0.
Notes. Apparent performance is computed on the development data used to fit the model. Internal validation uses 10-fold cross-validation with out-of-fold predictions. Bias = mean(Pred−Measured); 95% LoA = bias ± 1.96 × SD.
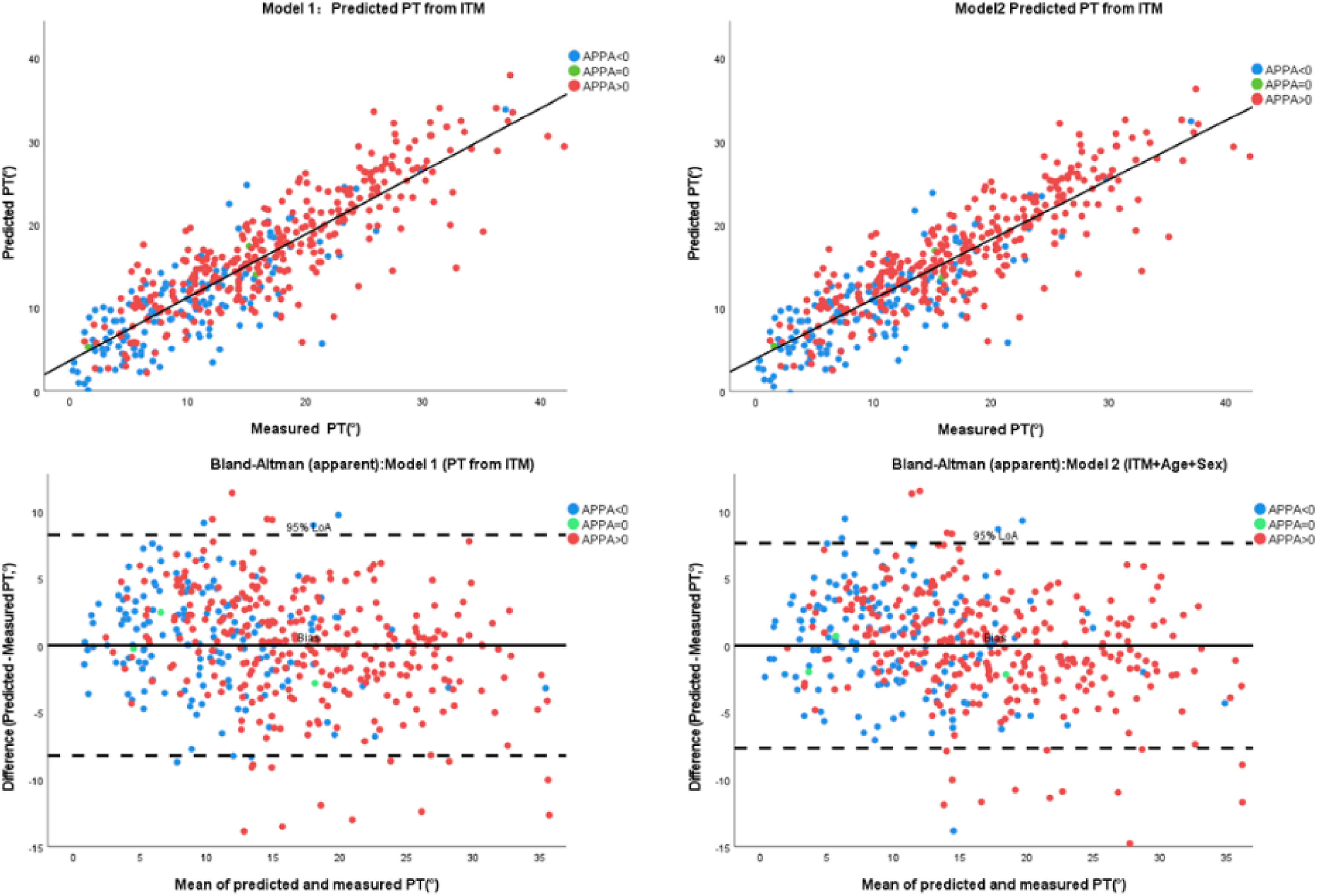
Model performance for estimating PT based on ITM.
Discussion
This study yielded three main findings. First, among the candidate iliac tilt metrics, ITM showed the most favorable overall balance of measurability, reproducibility, and agreement with measured PT. Second, APPA-defined pelvic retroversion was more frequently observed in older age groups, whereas the APPA = 0 group was rare and was retained only as a mathematical neutral reference. Third, ITM was strongly correlated with measured PT, and an ITM-based regression model incorporating age and sex provided internally validated PT estimation with modest average error. Together, these findings support ITM-based PT estimation as the main analytical focus of this study, with APPA-defined pelvic state serving as a descriptive and stratified radiographic context.
The selection of ITM as the primary IT-derived metric was supported by both measurement feasibility and agreement metrics. ITM was measurable in 920 of 977 radiographs and showed the lowest MAE among the candidate IT measurements, with narrower limits of agreement than ITS or ITI. The reliability analysis also supported the reproducibility of IT-derived measurements. In particular, ITM showed high intraobserver and interobserver reliability, suggesting that it can be measured consistently using the iliac cortical density line. These results are consistent with prior work suggesting that iliac tilt may provide a useful approximation of PT when conventional pelvic landmarks are difficult to assess.21,22 However, direct PT measurement remains preferable when the femoral heads are clearly visible.
APPA-defined pelvic state served as a descriptive framework for pelvic orientation in this cohort. APPA-defined retroversion was more frequently observed in older age strata, consistent with previous radiographic studies reporting age-related differences in sagittal spinopelvic parameters.29–31 Within this stratified framework, ITM showed a stronger age-related trend in the APPA >0 group than in the APPA < 0 group: ITM increased by 1.22° per 10 years in the retroversion group (p < 0.001), whereas the trend was weaker and not statistically significant in the anteversion group (β = 0.42° per 10 years, p = 0.067). These findings suggest that APPA-defined pelvic state may help contextualize age-related differences in ITM distribution, although they should be interpreted as cross-sectional associations rather than longitudinal evidence of progressive pelvic retroversion with aging. APPA = 0 was interpreted as a geometric neutral reference, indicating that the anterior pelvic plane coincides with the vertical line on the sagittal view, rather than as an independent clinical phenotype. Because sagittal pelvic orientation varies continuously and can be affected by posture and radiographic positioning, an exact 0° value is unlikely to define a stable subgroup in real-world radiographs.32–34 Given the small size of the APPA = 0 group, it was retained for descriptive purposes only and excluded from inferential comparisons. In this context, APPA is best understood as a stratified radiographic descriptor rather than as a separate primary endpoint.
The correlation analysis further supports ITM’s role as a PT-related surrogate. PT showed the strongest correlation with ITM (r = 0.87, p < 0.001), while APPA correlated moderately with both ITM and PT. These findings are consistent with previous observations that PT and SS are posture-dependent and may show measurement variability, thereby motivating pelvic metrics based on bony landmarks and reference planes.12,13,15 They also support the use of APPA-defined pelvic state as a stratified context for interpreting ITM distribution and ITM–PT relationships. The full Pearson correlation matrix and heatmap are provided in the Supplemental Material.
At the model level, the ITM-only model already explained most of the variance in measured PT, and adding age and sex produced a modest but consistent improvement in internal validation. The MAE of approximately 3° indicates that the predicted PT differed from measured PT by a small average amount, which may be acceptable for approximate estimation, cohort-level analyses, and missing-parameter approximation.
From a practical perspective, the ITM-based model may help approximate PT when direct PT measurement is limited by inadequate visualization of the femoral heads on lateral radiographs. This interpretation is consistent with prior work proposing iliac tilt–based equations for estimating PT, including sex-stratified models. 21 Zhao et al. 22 reported a negative correlation between PT and IT in adolescents, and this discrepancy may be partly explained by differences in age group, angle definition, sign convention, or measurement direction. Nevertheless, the clinical use of the model should be interpreted with caution. Although the average estimation error was modest, the limits of agreement indicate non-negligible individual-level error. 35 Therefore, ITM-based estimation may be more appropriate for cohort-level analyses, missing-parameter approximation, and preliminary sagittal stratification than as a replacement for direct PT measurement when the femoral heads are clearly visible. Moreover, because measured PT was required as the reference standard, the model was developed and internally validated only in radiographs with directly measurable PT. Its application to PT-limited or PT-nonmeasurable radiographs should therefore be considered potential and requires further validation.
Limitations
Several limitations should be acknowledged. First, this was a single-center retrospective study based on a clinical outpatient radiographic cohort and a relatively consistent acquisition protocol. Although 10-fold cross-validation was used for internal validation, no independent external validation cohort was available; therefore, the proposed equation should be considered internally validated only. Second, the analytic cohort required directly measurable PT because measured PT served as the reference standard for evaluating IT-derived estimates. As a result, radiographs in which PT could not be directly measured were excluded from model development and internal validation. Thus, although the ITM-based model may be useful when direct PT measurement is limited, its accuracy in PT-nonmeasurable radiographs requires further validation. Third, we did not directly test how pelvic rotation, lower-limb positioning, or technical differences in radiographic acquisition influence ITM. Prior work indicates that posture and positioning can change sagittal parameter readings, so future studies should incorporate these factors as covariates or sensitivity conditions.32–34 Finally, the APPA = 0 subgroup was too small to support reliable inference and was therefore retained only as a mathematical neutral reference. Overall, the ITM-based model should be viewed as an approximate estimation tool rather than a complete replacement for direct PT measurement when the femoral heads are clearly visible.
Conclusions
In this large standing radiographic cohort with directly measurable PT, APPA-defined pelvic retroversion was more frequently observed in older age groups. Among candidate iliac tilt measurements, ITM provided the most favorable overall balance of measurability and estimation error. An ITM-based model may provide an approximate estimate of PT, help reduce information loss when direct PT measurement is limited, and offer a consistent entry point for subsequent sagittal alignment assessment and stratified research. Further validation is required before applying the model to radiographs in which PT is not directly measurable.
Supplemental material
Supplemental material - APPA-defined pelvic state and iliac tilt–based estimation of pelvic tilt in a large standing radiographic cohort
Supplemental material for APPA-defined pelvic state and iliac tilt–based estimation of pelvic tilt in a large standing radiographic cohort by Siyuan Wang, Shuo Yang, Hao Qi, Chenxi Wang, Chenjie Dai, Wei Chen, Di Zhang in Journal of Orthopaedic Surgery
Footnotes
Ethical considerations
This study was approved by the Ethics Committee of the Third Hospital of Hebei Medical University (K2022-067-1). All procedures were performed in accordance with the Declaration of Helsinki and relevant institutional requirements.
Consent to participate
Written informed consent to participate was obtained from all participants and/or their legal guardians, as appropriate.
Author Contributions
Siyuan Wang: Conceptualization, Methodology, Formal analysis, Investigation, Writing – original draft, Writing – review & editing. Shuo Yang: Data curation, Formal analysis, Investigation, Writing – original draft. Hao Qi: Investigation, Technical support for experiments. Chenxi Wang: Data analysis, performed the experiments. Chenjie Dai: Visualization, tables and figures preparation. Wei Chen: Technical support for experiments. Di Zhang: Supervision, Project administration, Funding acquisition, Writing – review & editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. All Authors have not received any financial support or other benefits from commercial sources for the work reported in the manuscript, nor do they have any other financial interests which could create a potential conflict of interest or the appearance of a conflict of interest with regard to the work.
Data Availability Statement
All data and materials related to this article will be made available upon request by contacting the first author via email.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.