
Abstract
Objective
To evaluate efficiency of a percutaneous opening-wedge osteotomy, realignment, and fixation for hand bone malunions.
Methods
From November 2020 to November 2023, the patients with hand bone malunions were treated. Fracture angulation was assessed on X-rays or CT scans. Range of motion of the digits was assessed based on the total active motion scale. The scales were graded as excellent (100%), good (75%–99%), fair (50%–74%), and poor (<50%) based on the total active motion.
Results
There were 47 patients (42 male and 5 female patients) with the mean age of 34 years (range, 17–58 years). The injured digits included thumb (n = 10), index finger (n = 6), long finger (n = 7), ring finger (n = 11), and little finger (n = 13). The mean duration from injury to surgery was 16 weeks (range, 3–58 weeks). Bone healing was achieved in all patients after a mean of 6 weeks (range, 4–12 weeks). The mean follow-up period was 26 months (range, 24–29 months). The mean preoperative apex angulation of the fingers was 43° (range, 11°–68°), and the mean angulation at the final follow-up was 2° (range, 0°–6°). The mean preoperative apex angulation of the thumbs was 40° (range, 32°–54°), and the mean angulation at the final follow-up was 0° (range, 0°–5°). At the final follow-up, the mean total active motion scale was 257° (range, 116°–283°). There were 36 excellent and 11 good results.
Conclusion
Hand bone malunions can be treated with a percutaneous opening-wedge osteotomy, realignment, and fixation, resulting in good functional outcomes.
Keywords
Introduction
Malunion is a common complication of hand bones, presenting a combination of a functional and aesthetic problem. 1 Open osteotomy and correction are the most common treatments, but the complications include infection, soft tissue injuries, and the possibility of implant removal. 2 Currently, the optimal treatment is still controversial.
Buchler et al. 3 found that the best method to correct lateral angulation, flexion, or extension deformities is an opening-wedge osteotomy, followed by internal fixation. Ring et al. 4 treated a malunion of the ring finger through a 3 mm incision but fixation with crossing K-wires is difficult and unstable. Del Piñal et al. 5 treated 4 metacarpal and phalangeal malunions 8 weeks after injury through a 5-mm open incision. They performed opening- or closing-wedge osteotomy followed by fixation with a cannulated headless screw. The drawbacks included damage to the articular surface of the metacarpal head, inability to restore the normal length of the bone, rotational instability that needed to control with a splint, and possibility of bone grafting. 6 Plate fixation can achieve a good or excellent result, but tendon irritation and possible implant removal are the major concerns. 7 Moreover, bone grafting is often required in opening-wedged osteotomy.
This retrospective study aimed to evaluate efficiency of the percutaneous opening-wedge osteotomy, realignment, and fixation of metacarpal and phalangeal malunions.
Materials and methods
The study was conducted in accordance with the Declaration of Helsinki for the ethical standards of the institutional review boards of the *** Hospital. Ethical approvals were obtained from the Ethical Review Board of the participating hospital, i.e., *** Hospital. Informed consent was obtained from each patient. Fund Project: Baoding City Science and Technology Plan Project (2441ZF034).
From November 2020 to November 2023, consecutive patients with hand bone malunion deformities were treated in our hospitals. Preoperative X-rays were obtained in all patients, CT scans were obtained as needed (Figure 1(a) and (b)). The inclusion criteria of the study were (1) patient age ≥17 years; (2) malunion of extra-articular metacarpal and phalangeal fractures; (3) fractures angulated >30°; and (4) rotational deformity. The exclusion criteria included (1) patient age <17 years due to immature bone; (2) patient age >70 years due to osteoporosis; (3) intra-articular fracture; (4) <3 weeks from injury because bone healing did not occur; (5) nonunion that required bone grafting; (6) minor deformities that did not affect hand function; (7) uncooperative patients; and (8) infectious condition, rheumatoid arthritis, or gout. All operations were performed by the same surgical team, including 4 hand surgeons (i.e., ZH, XZ, XY, and GZ). In case 1, a 26-year-old male patient suffers the first metacarpal malunion 5 weeks after injury. (a) Preoperative lateral X-ray. (b) Preoperative CT scan. (c) A sketch shows multiple holes made manually using a 10- or 1.2-mm K-wire. (d) The dorsal angulation is corrected by approaching two joystick K-wires. (e) A photo showing orientation of reduction power. (f) Fixation is complete by securing the wire ends using bone cement. (g) Bone healing occurs after 6 weeks.
Indications of the surgery were almost all patterns of extraarticular phalangeal and metacarpal malunion, and the patient has cosmetic and functional issues, especially malunions with dorsal apex angulation >45° and rotational malunions. Contraindications were intraarticular fractures, minimal cosmetic and functional problems, infection states, and medical conditions.
Surgical technique
Selecting osteotomy techniques based on fracture site and duration after fracture.
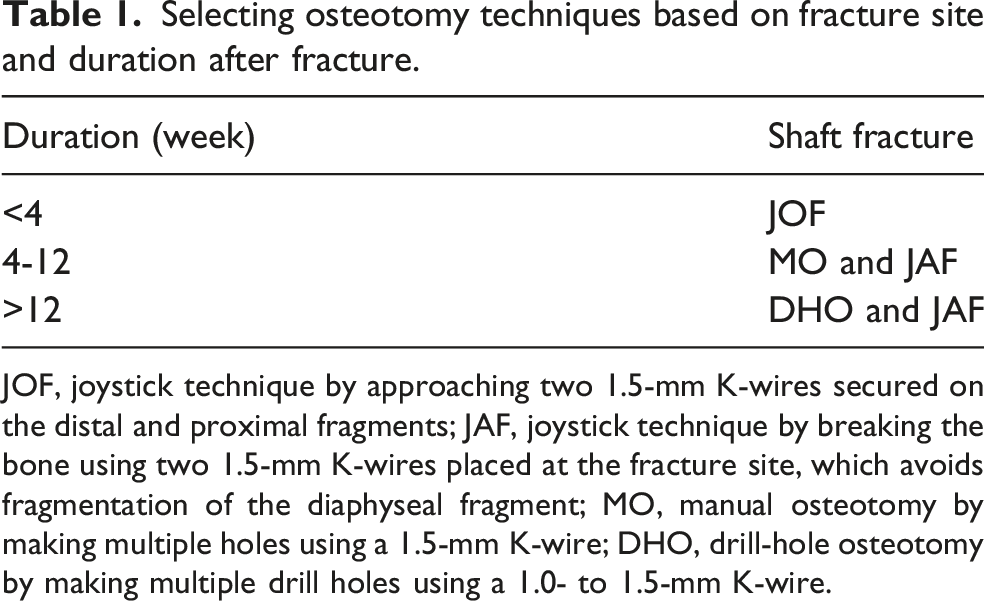
JOF, joystick technique by approaching two 1.5-mm K-wires secured on the distal and proximal fragments; JAF, joystick technique by breaking the bone using two 1.5-mm K-wires placed at the fracture site, which avoids fragmentation of the diaphyseal fragment; MO, manual osteotomy by making multiple holes using a 1.5-mm K-wire; DHO, drill-hole osteotomy by making multiple drill holes using a 1.0- to 1.5-mm K-wire.
Postoperative treatments
After surgery, we used a dorsal splint to protect the fixation system, but there was no restriction to joint motion. Active motion of the digits was started on the second postoperative day as tolerated. Pin care was done every 3–5 days as needed. Once bone healing with callus formation was observed on X-rays (Figure 1(g); Figure 2(a)–(c)), the K-wires were cut off and removed. Range of motion 6 weeks after surgery. (a) Extension. (b) Flexion. (c) Abduction.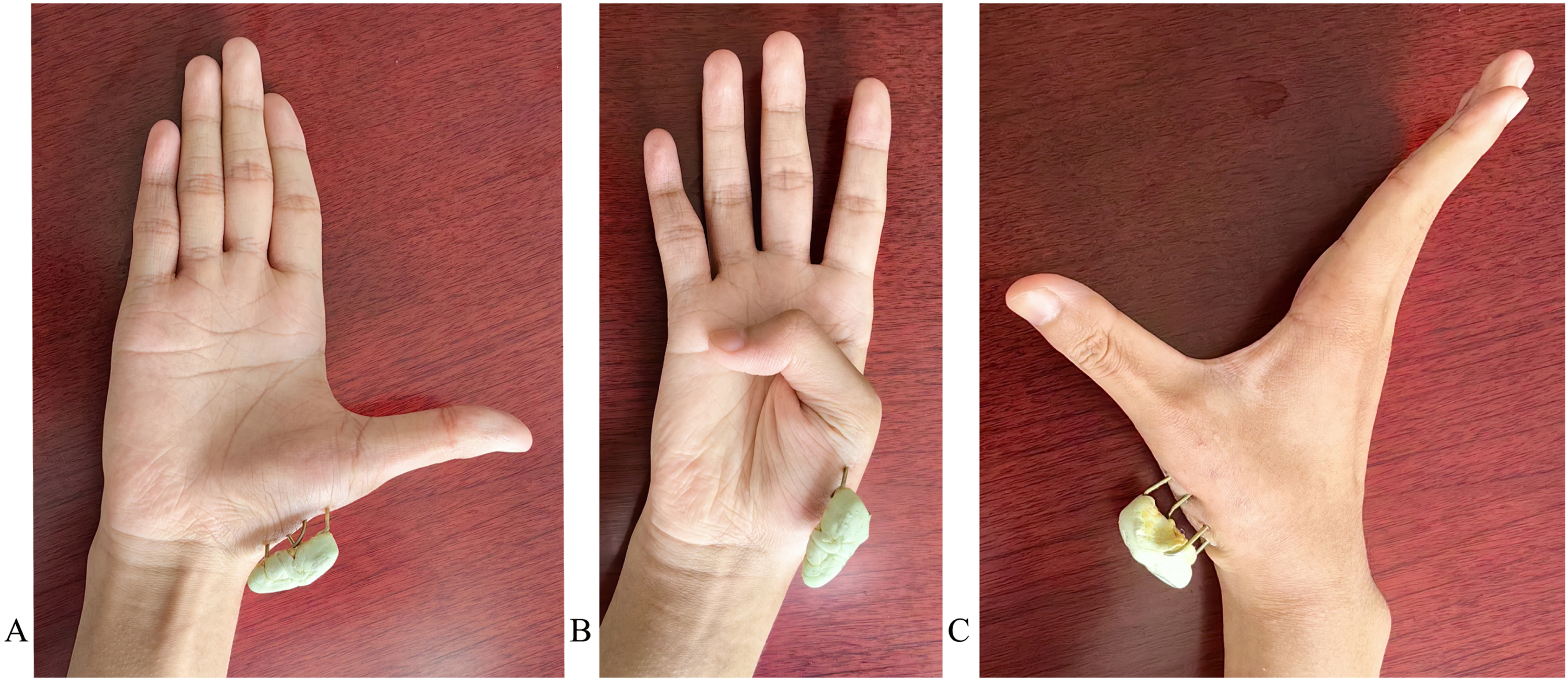
Outcome evaluation
Bone healing was confirmed when we observed a bridging callus across the fracture line on X-rays. Nonunion was defined as no evidence of bone healing observed 3 months after surgery. Bone shortening was measured by comparing the axial of the uninjured bone metacarpal on posteroanterior X-rays. We evaluated the angulation of the fractures on lateral X-rays by measuring the angle created by the dorsal cortical line of the distal and proximal fragments. 7 The rotational deformity was clinically assessed based on the extension of the axis of the digits toward the scaphoid tubercle or the existence of overlapping digits during flexion and orientation of the fingernail during extension.8,9 We evaluated the range of motion of the digits based on the total active motion scoring system of American Society for Surgery of the Hand. 10 The motion is calculated by adding the active range of motion of the metacarpophalangeal, proximal interphalangeal, and distal interphalangeal joints (recorded as 0° for a thumb). The motion was graded as excellent (100%), good (75%–99%), fair (50%–74%), and poor (<50%). 11 To exclude the strength discrepancy between the dominant and non-dominant hands, the grip strength of the dominant hand was 15% higher than that of the non-dominant hand. 12 Dorsal prominence, the pain of the injured site, and aesthetic appearance of the hand were evaluated based on the 10-cm visual analogue scale. Patient satisfaction was assessed using the Short Assessment of Patient Satisfaction (SAPS; 0–10, very dissatisfied; 11–18, dissatisfied; 19–26, satisfied; 27–28, very satisfied). 13
Statistical analysis
Variables were presented as mean and standard deviation and range. We used the chi-square test to analyze data. A p < 0.05 was considered statistically significant. All statistical analyses were performed using SPSS version 24.0 (IBM Corp., Armonk, NY, USA).
Results
Demographic and clinical characteristics for 47 patients.
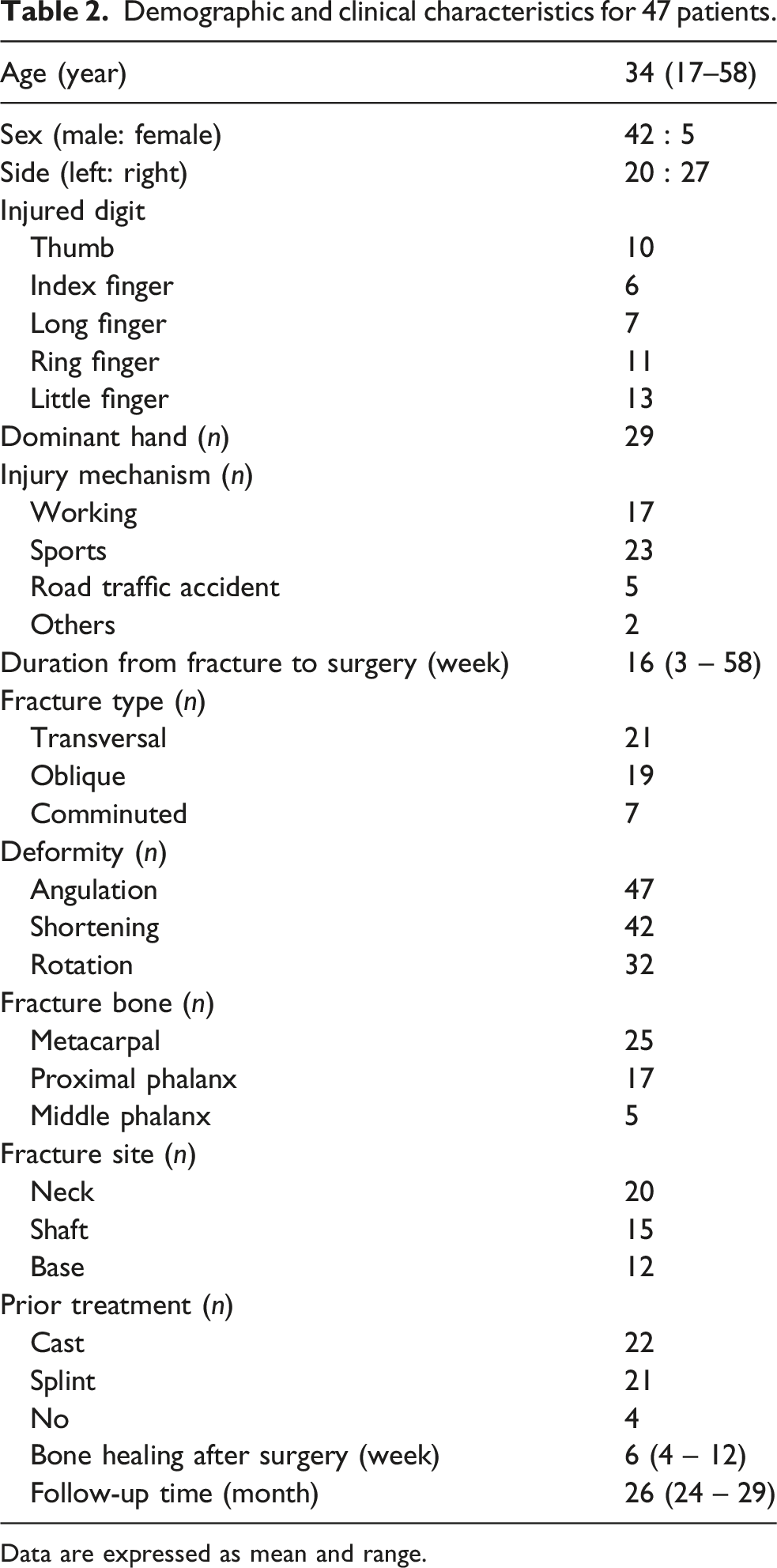
Data are expressed as mean and range.
Before versus after malunion correction.

Data are shown as mean ± standard deviation (range); *, measured using the angle between the middle and ring fingernail during extension.
Outcomes of 47 patients 2 years after surgery.
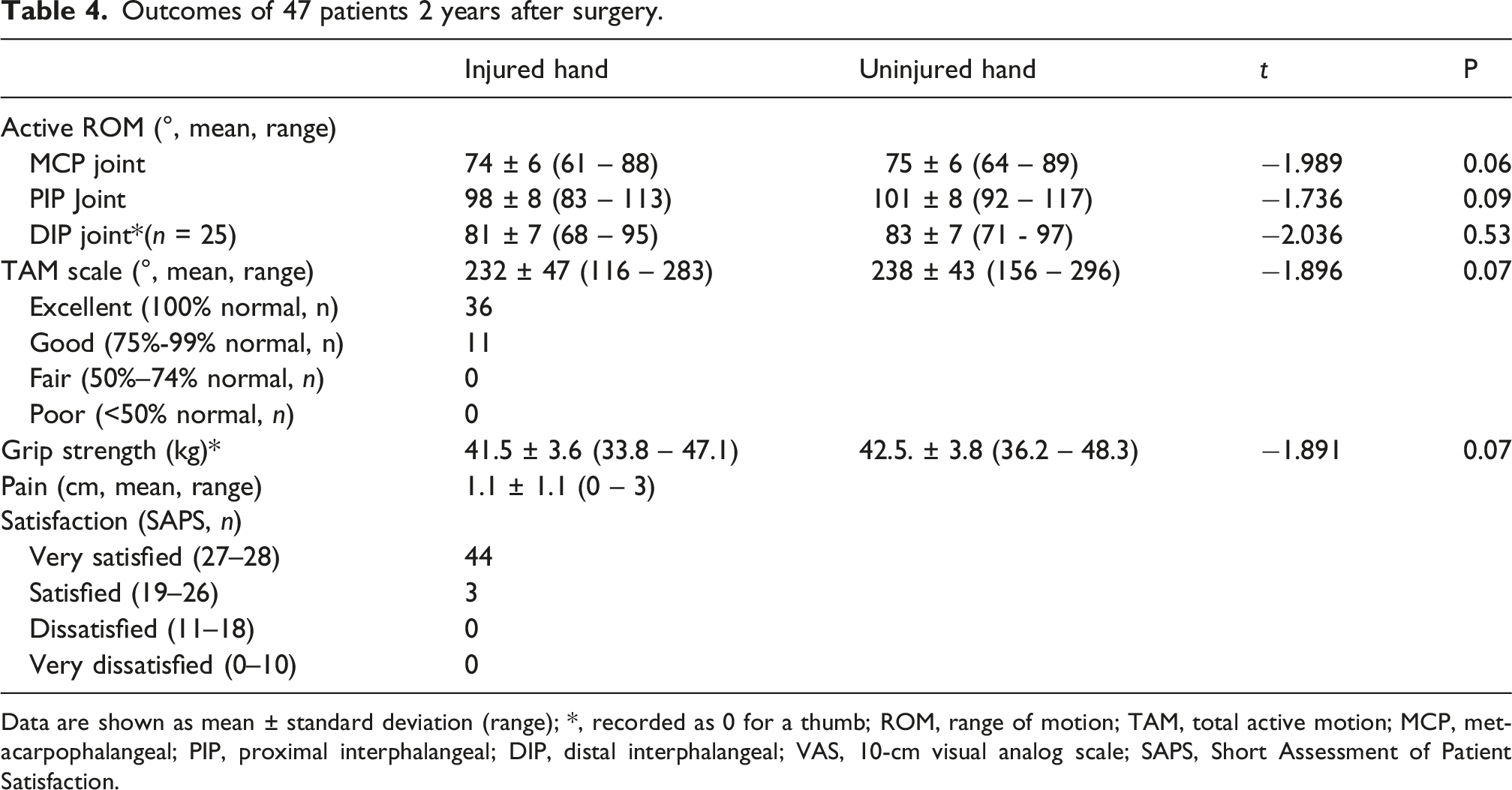
Data are shown as mean ± standard deviation (range); *, recorded as 0 for a thumb; ROM, range of motion; TAM, total active motion; MCP, metacarpophalangeal; PIP, proximal interphalangeal; DIP, distal interphalangeal; VAS, 10-cm visual analog scale; SAPS, Short Assessment of Patient Satisfaction.
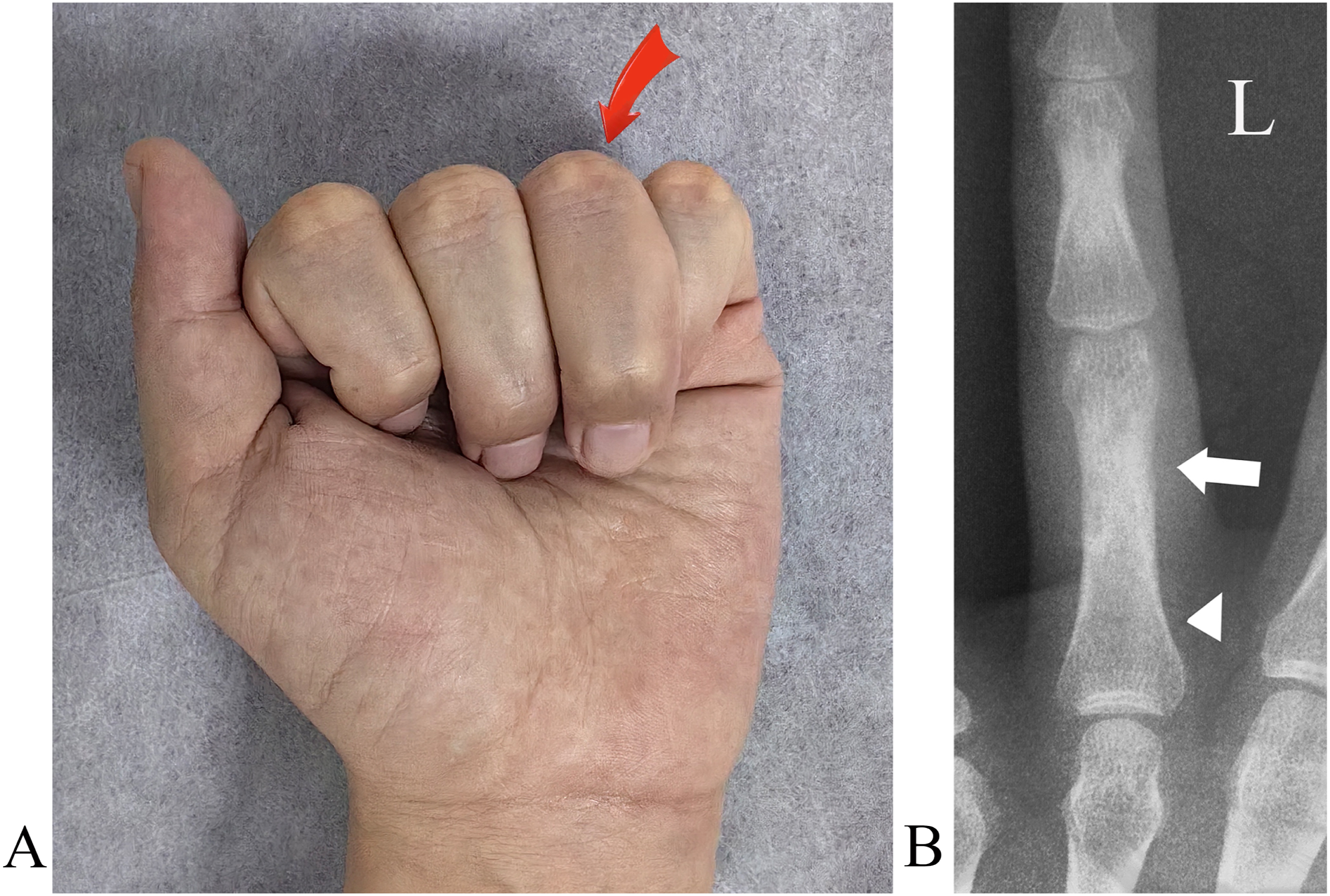
In case 2, a 31-year-old male patient suffers injury to the proximal phalanx of the left ring finger 1 year ago. (a) Malunion and malrotation of the ring finger (arrow). (b) Malunion site (arrow) and osteotomy level (arrow head) as planned on preoperative posteroanterior X-ray.
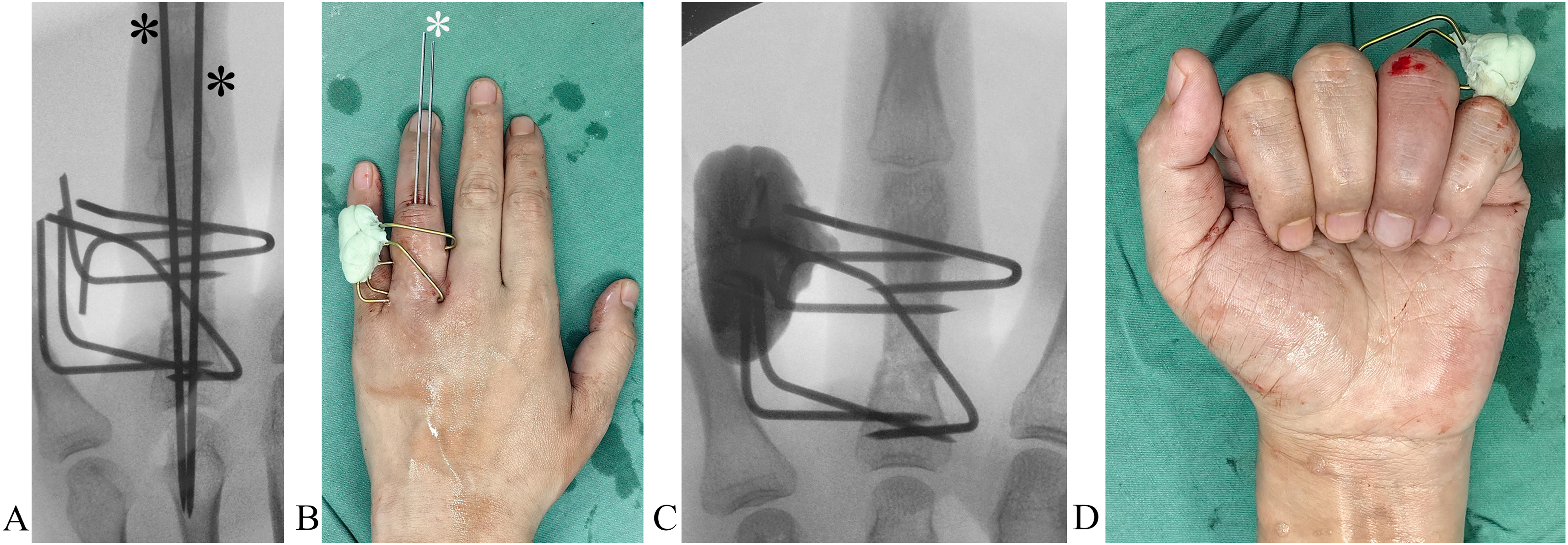
Surgical procedures. (a) Drill-hole osteotomy is complete and temporarily stabilization with K-wires (*) secured on the soft tissues. (b) A photo show fixation with bone cement. (c) Fixation on posteroanterior X-ray. (d) Rotational deformity is corrected.
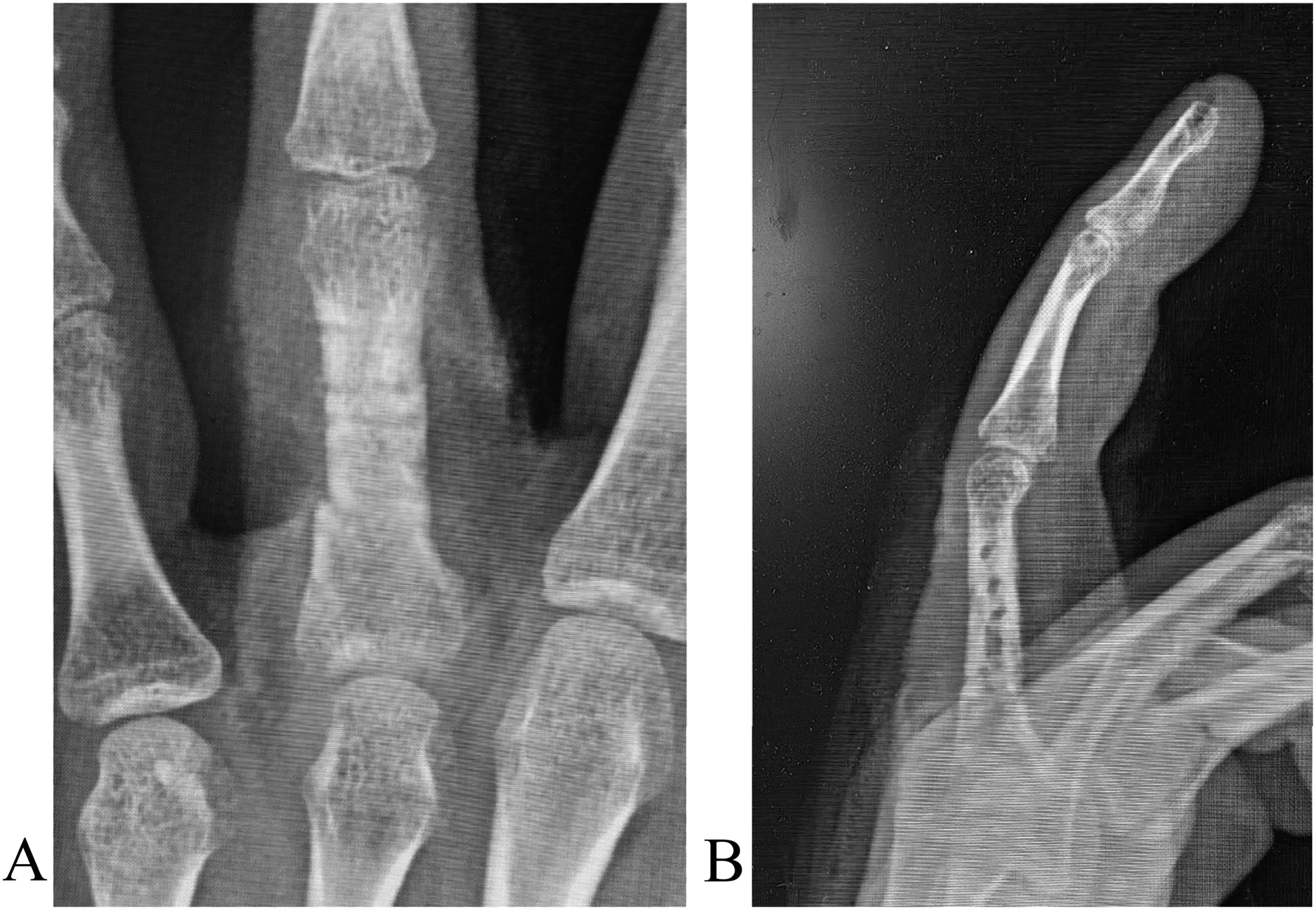
Bone healing 6 weeks after surgery. (a) Posteroanterior X-ray. (b) Lateral X-ray.
Discussion
Hand bone malunion deformities can be successfully treated with closed open wedge-osteotomy, realignment, and fixation. The minimally invasive technique avoids open surgery, severe periosteum injuries, bone grafting, and related complications. Perpendicular K-wire placement decreases the risk of pin site infection. Range of motion exercise allows to perform immediately after surgery, resulting in good functional recovery. Hand movement and grip strength are nearly fully restored with satisfactory functional recovery.
Angulation of the proximal phalanx may lead to a mechanical block of flexion. 14 An angulation exceeds 15° may cause an extensor lag because of bone length shortening and consequential increase in the length of the extensor tendon. 15 Whereas when it exceeds 25°, both extension and flexion are affected. 16 This extensor lag may cause a fixed flexion contracture, which in turn results in a pseudo-claw deformity.17,18 Malrotation is mostly present in the index, long, ring, and small fingers, which may cause symptomatic finger scissoring or impingement. 19 Conflicting information exists as to the degree of fracture displacement that is acceptable while still achieving good results in pain relief, range of motion, and angular and rotational deformity. 5
Nonsurgical treatments are a choice for a mild deformity due to acceptable outcomes with less complications. Indications for surgery mainly include bone shortening <2 mm. Dorsal angulations <25° (ring finger), 30° (5th metacarpal) or 10° (long and index fingers) are acceptable, depending on the patient’s wishes and cosmetic need. 4 Shortening in metacarpal fractures is also poorly tolerated. For every 2 mm in shortening, there is a 7° extensor lag. Malrotation mostly present in the ring and small fingers, which transmits the rotation distally to affect the whole digit and causes functional impairment, specifically on making a fist. 20
Malunions can be realigned through a closing or opening-wedge osteotomy though open surgery. Closing wedge osteotomies may cause bone shortening. An opening-wedge osteotomy implies the use of a bone graft to fill the void. Zhang et al. 21 treated 21 patients who had fifth metacarpal malunions with an opening wedge osteotomy. The results showed healing at an average of 2 months. Pinch strength and grip strength were comparable with the uninjured hand. Haider et al. 22 treated 11 phalangeal and metacarpal malunions through open surgery with a multiple drill hole osteotomy instead of the usual oscillating saw. In one case, a broken drillbit was observed, but no other complication was observed. Fixation was achieved with a plate and screw system. The outcomes are acceptable, but tendon adhesion and the need for bone grafting are possible. Hirsiger et al. 23 used CT scans for preoperative 3 D printing. Average rotational deformity improved from 10° to 2°, and translational malposition went from 1.4 mm to 0.4 mm. Eleven patients with malunited proximal phalanx accompanied by flexor tendon adhesion were examined retrospectively. 24
Several issues need to be addressed. Owing to the nature of our technique, only opening-wedge osteotomy can be performed. Although a between-fragment gap may occur after realignment, the periosteum may be intact, which benefits gap healing. Bone fragmentation may happen during reduction maneuver, but gentle manipulation may decrease the risk. Nevertheless, minor fragmentation rarely affects bone healing and remodeling. Like an external fixator, our cemented K-wire system provides strong rigidity in bending, compression, and torque. If percutaneous osteotomy and reduction have failed, the technique can be converted to open surgery.
The advantages of the technique are a minimally invasive procedure, no need for bone grafts, and no implant-related tendon irritation. Opening-wedged osteotomy avoids further bone shortening. The fixation is rigid, allowing joint motion. A cemented frame prevents rotational deformity. The major disadvantages are the inconvenience of the cement frame for a patient’s daily life. Pin site infection is rare when the K-wire is inserted into skin perpendicularly, compared to oblique placement. We do not attempt to restore normal length of the bone in all cases because minor bone shortening is often acceptable.
Limitations of the study are a small patient group, retrospectively design and lack of kinematics of the fixation system. The study lacks a comparison between the bone cement frame and conventional external fixator in construct stability, such as pin loosening, pin migration, joint stiffness, and early joint motion. Surgeons’ preferences, judgment, experience, and ability may affect the treatments and outcomes.
Declarations
Ethics approval or consent to participate: The study was conducted in accordance with the Declaration of Helsinki for the ethical standards of the institutional review boards of the *** Hospital. Ethical approvals were obtained from the Ethical Review Board of the participating hospital, i.e., *** Hospital. Informed consent was obtained from each patient.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Baoding City Science and Technology Plan Project, 2441ZF034.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.